JAN
THEORETICAL PAPER
Postoperative recovery: a concept analysis
Renée Allvin1, Katarina Berg2, Ewa Idvall3 & Ulrica Nilsson4
Accepted for publication 11 October 2006
1
Renée Allvin MSci RNA
Doctoral Student
Department of Anaesthesiology and Intensive
Care, Örebro University Hospital and
Department of Clinical Medicine, Örebro
University, Örebro, Sweden
2
Katarina Berg MSci RNA
Doctoral Student
Department of Medicine and Care,
Linköping University, Linköping, Sweden
3
Ewa Idvall PhD RNT
Associate Professor
Scientific Tutor and Senior Lecturer, Research
Section, Kalmar County Council, Kalmar and
Department of Medicine and Care, Linköping
University, Linköping, Sweden
4
Ulrica Nilsson PhD RNA
Senior Lecturer
Department of Anaesthesiology and Intensive
Care, Örebro University Hospital and
Department of Cardiothoracic Surgery,
Örebro University Hospital and Department
of Health Sciences, Örebro University,
Örebro, Sweden
Correspondence to Ewa Idvall:
e-mail: evaid@ltkalmar.se
ALLVIN R., BERG K., IDVALL E. & NILSSON U. (2007)
Postoperative recovery: a
concept analysis. Journal of Advanced Nursing
doi: 10.1111/j.1365-2648.2006.04156.x
Abstract
Title. Postoperative recovery: a concept analysis
Aim. This paper presents a concept analysis of the phenomenon of postoperative
recovery.
Background. Each year, millions of patients throughout the world undergo surgical
procedures. Although postoperative recovery is commonly used as an outcome of
surgery, it is difficult to identify a standard definition.
Method. Walker and Avant’s concept analysis approach was used. Literature retrieved from MEDLINE and CINAHL databases for English language papers
published from 1982 to 2005 was used for the analysis.
Findings. The theoretical definition developed points out that postoperative
recovery is an energy-requiring process of returning to normality and wholeness. It
is defined by comparative standards, achieved by regaining control over physical,
psychological, social and habitual functions, and results in a return to preoperative
level of independence/dependency in activities of daily living and optimum level of
psychological well-being.
Conclusion. The concept of postoperative recovery lacks clarity, both in its
meaning in relation to postoperative recovery to healthcare professionals in their
care for surgical patients, and in the understanding of what researchers in this area
really intend to investigate. The theoretical definition we have developed may be
useful but needs to be further explored.
Keywords: concept analysis, definition, nursing, postoperative, recovery
Introduction
A wide range of procedures are available to treat patients who
require surgical intervention. An important part of the patient
experience, irrespective of the type of procedure, is postoperative recovery. Research in this field is extensive and includes
studies of postoperative recovery as an outcome measure, e.g.
factors associated with length of hospitalization (Kehlet &
Dahl 2003), specific surgical procedures (Bay-Nielsen et al.
2004), and the use of specific pain management techniques
(Pavlin et al. 2005, Werawatganon & Charuluxanun 2005).
The emphasis in qualitative studies is on patient experiences in
postoperative recovery, and primarily factors associated with
specific diseases, e.g. gastrointestinal cancer (Olsson et al.
2002), gastro-oesophageal reflux (Nilsson et al. 2002) and
prostate cancer (Burt et al. 2005). Although postoperative
recovery is commonly used as a concept, it is difficult to identify
a standard definition. A conventional concept runs the risk of
being used without reflection. Furthermore, different disciplines may attribute different meanings to the same concept.
Concept analysis is a means to clarify over-used or vague
concepts that are prevalent in clinical practice, hence enabling
2007 The Authors. Journal compilation 2007 Blackwell Publishing Ltd
1
R. Allvin et al.
those using the term to perceive it in the same way. The
purpose of concept analysis in nursing research is to examine
the basic elements of a concept by revealing its internal
structure and critical attributes (Walker & Avant 2005).
Knowledge changes over time. Hence, the understanding of a
concept should be considered as a dynamic, ongoing process
that is responsive to new knowledge and experiences (Meleis
2005).
Early discharge from hospital requires patients to handle
much of the postoperative recovery process on their own.
Defining recovery from a holistic perspective is essential for
nursing and for the advancement of postoperative care.
Formulating a definition of postoperative recovery promotes
understanding of its use in postoperative care and the factors
that influence it. Therefore, the aim of this study was to present
a concept analysis of the phenomenon postoperative recovery.
Methods
The scientific literature was searched to produce a definition
that explains the concept of postoperative recovery. We
searched the MEDLINE and CINAHL databases for English
language papers published from 1982 to October 2005 that
contained the following search terms: concept analysis,
recovery, anaesthesia, anesthesia, postsurgical, postoperative,
recovery process, post discharge, convalescence, rehabilitation used separately and in combination with each other.
The reference lists of all retrieved articles were searched for
additional studies. The papers included in the analysis
described and highlighted the phenomenon postoperative
recovery, i.e. the meaning of recovery. Papers were excluded
for example, where intervention and descriptive studies used
postoperative recovery as an outcome measure for pain,
nausea, mobilization, etc. Dictionaries and textbooks were
also searched for a definition of the concept. Walker and
Avant’s (2005) approach to concept analysis was used as the
method to define the concept postoperative recovery and a
total of 26 publications, one textbook and two dictionaries
were used in the analysis.
Findings
Dictionary and thesaurus definitions
Initial information about recovery was found in dictionaries
and a thesaurus. The Encarta World English Dictionary,
North American Edition (2005) defines recovery as:
The return to normal health of somebody who has been ill or
injured, the return of something to a normal or improved state after
2
a setback or loss, the regaining of something lost or taken away, the
extraction of useful substances from waste or refuse (environment),
the obtaining of something by the ruling of a court (law), a return
to the guard position after making an attack (fencing), and the
bringing forward of the arm to make another stroke (rowing
swimming).
According to the Wordsmyth English Dictionary – Thesaurus
(2005), synonyms for recovery are: recoup, salvage, return,
convalescence and cure.
Uses of the concept
In ambulatory surgery, postoperative recovery can be divided
into three phases: early, intermediate and late recovery
(Steward & Volgyesi 1978, Korttila 1995). The early phase
lasts from discontinuation of anaesthesia until patients have
recovered their vital protective reflexes. The intermediate
phase lasts from when patients have regained stable vital
functions until readiness for discharge home. The late phase
lasts from discharge until the patients reach preoperative
health and well-being (Steward & Volgyesi 1978, Marshall
& Chung 1999). Presumably, the three phases of recovery
would also apply to hospital inpatients.
From a holistic perspective, postoperative recovery is
described as a process defined by improvement in functional
status and the perception that one is recovering (Zalon 2004).
Another description is a return to wholeness that occurs by
conservation of energy and reinstatement of integrity (Levine
1991). Pain, depression and fatigue are related to patients’
self-perceptions of postoperative recovery after abdominal
surgery and after coronary artery by-pass graft surgery
(Zalon 2004). Patients have also major concerns about
returning to independence in activities in daily life (Kirkevold
et al. 1996, Moore 1997). Physical sensations associated with
fatigue, pain from chest and leg incisions, pain in shoulder
and neck muscles, and pain while coughing are part of the
recovery process (Moore 1997). Pain and fatigue are the most
common and severe symptoms in postoperative recovery
(Moore 1997, Hodgson & Given 2004, Zalon 2004, Nilsson
et al. 2006) and indicate impaired structural integrity after
surgery (Zalon 2004). According to Levine (1991), fatigue is
a sign of limited energy resources, which is described as both
physical and psychological energy loss (Nilsson et al. 2006).
Postoperative fatigue may be caused by reduced energy and
preoperative anxiety (Nilsson et al. 2006). Pain, depression
and fatigue are also significantly related to functional status
and self-perception of recovery in older postoperative
abdominal patients (Zalon 2004). Psychological sensations,
e.g. negative emotions including depression, anger and
2007 The Authors. Journal compilation 2007 Blackwell Publishing Ltd
JAN: THEORETICAL PAPER
anxiety are also part of the recovery process (Moore 1997).
Depression reduces the conservation of personal integrity and
has been associated with lower functional status after surgery
(Zalon 2004).
Signs of recovery include a continuous decrease in discomforting bodily symptoms (Olsson et al. 2002). Physical
symptoms that overwhelm patients in the first months after
surgery are described as a kind of prison (Olsson et al. 2002)
and patients’ experiences from surgery can be an extensive
personal shock (Theobald & McMurray 2004).
As a psychosocial phenomenon, recovery has been studied
as abandoning the sick role (Parsons 1975). In a study by Kasl
and Cobb (1966), recovery was associated with discharge, as
an outcome measure for factors associated with the length of
hospitalization. This study examined the sick role at a
behavioural level, in which recovery was defined as leaving
the sick role to resume normal social obligations. A decade
later, a study of abandoning the sick role after cardiac bypass
surgery extended the research beyond hospitalization, and
recovery was described as returning to work (Brown &
Rawlinson 1977). The psychosocial recovery process also
involves interacting with other people and is more complex
and time-consuming than recovery of self-oriented activities.
Patients seem to focus on regaining physical, cognitive and
practical functions before focusing on relating to others
(Kirkevold et al. 1996). When an individual becomes
disabled, it is expected that treatment will be sought. When
this happens, the individual becomes dependent on others for
care. After a shorter or longer period, caregivers help the
patient develop the skills needed to take responsibility for
self-care (Andreoli 1990, Nilsson et al. 2006). To optimize
the recovery process, some patients require more detailed
discharge information on what to expect after surgery
(Theobald & McMurray 2004).
The availability of social support is important for
psychological well-being during the recovery process (Baker
1990, Nilsson et al. 2006). Psychological well-being is
influenced by met or unmet expectations, positive or
negative physical symptoms and positive or negative feelings
of personal competence (Baker 1990). This has also been
shown to be a significant factor influencing functional
recovery when controlling for age, comorbidities, site of
disease and symptoms (Hodgson & Given 2004). Recovery
can be described as regaining one’s optimum level of wellbeing (Andreoli 1990).
Baker (1989) conceptualized recovery as a phenomenon
that extended beyond discharge. Postdischarge recovery was
described as a process of returning to normal, as defined by
pre-illness comparative standards of physical, social and
psychological well-being. This process moves successively
Postoperative recovery
through three phases: passivity, activity resumption and
stabilization. Passivity is a time of rest to support physical
convalescence. During activity resumption, people prepare
for their return to a full range of activities. Stabilization starts
when they have returned to a full range of pre-illness, social
role functions. Reasons for resuming, or not resuming,
activity are dependent on cues and pressure. Those who
experienced congruence of cues and pressures reported
positive feelings about the recovery process. People who
perceived negative physical symptoms, especially fatigue, and
who were unable to respond to pressures, expressed frustration (Baker 1989).
The recovery process includes turning points, or recovery
indicators, defined as recovery trajectories. ‘Critical junctures’ in the trajectory can be identified as either improvements or setbacks in relation to the expected outcome. The
recovery trajectory is based on the belief that the patient will
recover. There is a wide recovery trajectory, but also multiple
smaller trajectories, e.g. concerning mobility and personal
hygiene. Each particular trajectory corresponds with the
progression and control of bodily functions as patients move
towards recovery, and these shifts in control are defined as
‘recovery markers’. Recovery could be described as becoming
independent and regaining control over one’s bodily functions and body care (Lawler 1991).
Defining attributes
Concept analysis requires the determination of the defining
attributes of characteristics that are most frequently associated with the concept and appear repeatedly in references to
it, according to Walker and Avant (2005). Based on their
approach, the defining attributes of recovery after surgery
are: (a) an energy-requiring process, (b) a return to a state of
normality and wholeness defined by comparative standards,
(c) regaining control over physical, psychological, social and
habitual functions, (d) returning to preoperative levels of
independency/dependency in activities of daily living and
(e) regaining one’s optimum level of well-being.
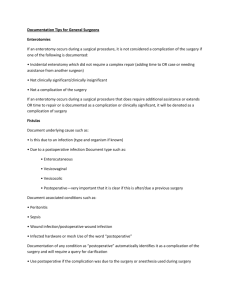
Several dimensions emerge from the literature. The
postoperative recovery process is divided into four dimensions, i.e. physiological, psychological, social and habitual
recovery (Table 1). In physiological recovery, patients
improve their functional status by regaining control over
reflexes and motor activities, normalized and controlled
bodily functions, loss of pain and fatigue and conservation
of energy. Passivity is also a part of physiological recovery.
Psychological recovery includes returning to psychological
well-being and wholeness, reinstated integrity, transition
from illness to health, loss of depression, anger, anxiety,
2007 The Authors. Journal compilation 2007 Blackwell Publishing Ltd
3
R. Allvin et al.
Table 1 Dimensions of postoperative recovery found in the literature
nausea, but was completely exhausted and had little muscle strength.
She was happy to have her family, who supported her in practical
Physiological
Regain control over reflexes and motor activities
Normalize and control bodily functions
Loss of pain and fatigue
Conservation of energy
Experience of passivity
Psychological
Experience of passivity
Return to psychological well-being
Return to wholeness
Reinstate integrity
Transition from illness to health
Loss of depression, anger, anxiety, fatigue and passivity
Experience of pressures and cues
Social
Becoming independent
Stabilize at full social function
Functioning in interaction with other people
Habitual
Stabilizing the full range of activities
Take responsibility for and controlling activities in daily care
Restoration of normal eating, drinking and toilets habits
Returning to work and driving
activities, e.g. buying food, cleaning the house, and caring for the
dog. Successively, she managed to return to the activities she
performed prior to surgery. Four weeks after surgery she returned
to work. By that time her wound was healed, and she had no
remaining physical symptoms. She was satisfied with the outcome of
surgery, as the bleeding had ceased. She was also relieved to know
that she did not have cancer. Fatigue was the only remaining
problem, since she was still tired and had little strength. She was
unable to manage even minor tasks after coming home from work.
This fatigue continued for about three months, after which she
regained normal strength in relation to her preoperative standard and
expectations.
This case demonstrates the defining attributes. Lisa’s recovery
was a process over time. She achieved effective treatment for
her physical symptoms. She experienced fatigue, which
forced her to rest and conserve energy. Successively, she
regained control over her physical and habitual functions. She
managed to return to work and to various activities. Also,
Lisa was happy with the result of her operation and felt
relieved that she did not have cancer.
fatigue and passivity. Psychological recovery also includes
experiences of pressures and cues. In the dimension of social
postoperative recovery, the patient strives to become independent and to stabilize at full social function, which
includes interacting with other people. In the habitual part
of recovery, the patient works towards stabilizing the full
range of activities by taking responsibility for and controlling activities in daily care, normal eating and drinking
habits, returning to work and driving.
Borderline case
Borderline cases are examples that contain most, but not all,
of the defining attributes (Walker & Avant 2005), for
example:
A 67-year-old man was in the garden with his wife and friends when
he suddenly experienced intense stomach pain. His wife called for an
ambulance, and he was taken to hospital. He was operated on
immediately, and the surgeon found that he suffered a colon rupture
Model case
caused by a tumour. During the early postoperative phase he
According to Walker and Avant (2005), a model case
demonstrates all of the defining attributes of the concept. A
model case for postoperative recovery appears below:
experienced severe pain. He was also shocked by the fact that he
had been operated on, and that he had a cancerous tumour. After a
few days it became clear that he had a wound infection. He was very
tired and had to remain in hospital for about two weeks. During this
Lisa is a 47-year-old woman who had a hysterectomy to treat
time he successively progressed regarding mobilization and intake of
bleeding. There were no complications during anaesthesia and
fluid and food. After discharge, he feared that something else could
surgery, and the entire procedure went smoothly. Lisa woke up in
happen to the wound. He was exhausted and needed a great deal of
a postanaesthesia recovery unit and was transported to the surgical
rest. In the first weeks, before he had the courage to leave the house,
ward a few hours later. Thanks to effective pain treatment she did not
he exercised indoors. Because of the cancer he required chemother-
experience pain, but was bothered by mild postoperative nausea. She
apy, which caused him considerable problems with diarrhoea and
managed to drink and eat and made successive progress in mobil-
nausea. After six months he had regained control over his physical
ization, toileting, and personal hygiene. Before surgery she had been
and practical functions and was able to return to independence in
worried about her diagnosis. She feared that a cancer disease caused
activities of daily living. However, because of the chemotherapy he
her symptoms. Afterwards, she was able to relax when a biopsy
had not returned to optimum psychological well-being. He experi-
revealed no malignancy. Lisa was discharged from the hospital four
enced side effects from the treatment and was still bothered by the
days after her operation. At that time she did not experience pain or
fact that he had cancer. He did not know what to expect in the future.
4
2007 The Authors. Journal compilation 2007 Blackwell Publishing Ltd
JAN: THEORETICAL PAPER
This man had reached the turning point for recovering
physical and habitual functions, but had not recovered
emotionally.
Related case
Related cases are similar to the concept and relate to it in
some way, but do not contain all the defining attributes
(Walker & Avant 2005). The following is an example:
A 39-year-old man was restoring his house. He was working alone
when he suddenly fell from a ladder. His wife found him lying
unconscious on the floor. An acute operation was necessary to stop
the bleeding in his brain. After surgery, he successively regained
control over physical functions. The process took several months. He
needed considerable rest, but managed to return to independence in
daily activities. The wound healed, and he does not have any residual
Postoperative recovery
surgery, caused by injury, illness or other factors. Surgery
leads to physical, psychological, habitual and social interruption.
Consequences are those events or conditions that occur as a
result of the concept (Walker & Avant 2005). Postoperative
recovery is an energy-demanding process with turning points
starting directly after surgery and extending beyond discharge. The intended consequence is to return to preoperative
physical, psychological, habitual and social status, an
optimum level of well-being, and preoperative levels of
independence/dependency in activities of daily living. Lawler
(1991) states that recovery means returning to independence
and regaining of control over bodily functions. We think that
a person needing assistance in activities of daily living can
also recover, not to a level of independence, but to their
former level of dependence.
conditions. However, this traumatic experience caused him to reflect.
It brought out other issues that had nothing to do with the surgery.
Empirical referents
This case is similar to the model case, but the process evolved
beyond the specific recovery from surgery. He searched for
meaning in his experience. The recovery process evolved into
more of a healing process.
According to Walker and Avant (2005), ‘Empirical referents
are classes or categories of actual phenomena that by their
existence or presence demonstrate the occurrence of the
concept itself’ (p. 73). In some cases, the empirical referents
are identical to the attributes (Walker & Avant 2005).
Several instruments are available that purport to measure
quality of recovery after anaesthesia and surgery (Myles et al.
1999, 2000a, Myles et al. 2000b, 2001, Leslie et al. 2003).
Also, several studies report on the development of instruments to evaluate the effectiveness of different interventions
during the recovery period (Aldrete & Kroulik 1970, Wolfer
& Davis 1970, Hogue et al. 2000, Kleinbeck 2000). Lee and
Steven (2000) reviewed the literature to discuss and describe
different approaches towards measuring recovery. They
stated that recovery is a process occurring over several
months, affected by factors such as adequate information;
anaesthetic and surgical techniques; restoration of normal
eating, drinking and toilet habits; loss of anxiety, depression
or fatigue; mobilization and rehabilitation to full social
functioning; and changing from a state of illness to a state of
health (Lee & Steven 2000).
Contrary case
Contrary cases are examples of what the concept is not
(Walker & Avant 2005). For example:
A 70-year-old woman was treated by knee replacement surgery. It
was an elective procedure, and she was well-prepared both
physically and mentally. The operation was performed using a
combined spinal-epidural block. When the ward nurse was doing
her routine postoperative monitoring on the first evening after
surgery she discovered that the patient had a total muscle
blockade. This appeared to be the result of bleeding in the
epidural space. Surgery was performed, but too late to avoid tissue
damage. The woman needed to spend the rest of her life in a
wheelchair.
This case demonstrates the opposite of recovery. A healthy
woman underwent elective surgery, which resulted in serious
tissue damage. She did not return to a preoperative level of
wholeness, but developed a new condition. Her situation was
much worse after the operation than before.
Antecedents and consequences
Antecedents are those events or incidents that must occur
prior to the occurrence of the concept (Walker & Avant
2005). With recovery in this context, the antecedent is
Discussion
A limitation in our study was the number of papers found,
and presumably the papers not found, through our search
strategy using search terms for postoperative recovery.
Valuable information might have gone undetected. Another
problem concerns synonyms. Convalescence is one of the
synonyms for recovery, according to the Wordsmith English
Dictionary. In a study (Jakobsen et al. 2003) aimed at
2007 The Authors. Journal compilation 2007 Blackwell Publishing Ltd
5
R. Allvin et al.
What is already known about this topic
• The term postoperative recovery is commonly used, but
it is not a clearly defined concept.
• Postoperative recovery is often associated with discharge from care, as an outcome measure for factors
associated with the length of hospitalization.
• Several instruments have been developed to measure
different aspects of postoperative recovery.
What this paper adds
• A definition of the concept postoperative recovery.
• Postoperative recovery is an energy-requiring process
that has four dimensions – physiological, psychological,
social and habitual recovery.
• Postoperative recovery is complex and includes different
turning points in the return to normality and wholeness.
describing convalescence after laparoscopic sterilization, the
data collected included time until return to work and
performance of core activities of daily living. These parameters could also be included in the definition of recovery
according to our concept analysis. Jakobsen et al. (2003) did
not define or describe the concept of convalescence, but used
different parameters as outcome measures for convalescence.
Similar papers using the concept of convalescence, or other
synonyms, were not included in our analysis. This also
highlights the complexity of a concept analysis and the
importance of describing the meaning of the different
concepts used in research.
We used Walker and Avant’s (2005) approach to define the
concept of postoperative recovery. This approach was useful
because of the systematic method. We also think that, for the
nurses in clinical practice, the cases clarify the complexity of
the concept. However, it is important for all healthcare
professionals to understand this complexity. Postoperative
recovery is a process starting directly after surgery and
existing beyond discharge and including different turning
points; it does not only involve cessation of physical
symptoms. Our definition of postoperative recovery has a
holistic perspective, which helps the nurses and other
healthcare professionals to support, treat, inform and understand surgical patients on their way back to preoperative
levels of independence/dependency.
Although the scientific literature commonly refers to the
concept of postoperative recovery, a theoretical definition of
the concept is difficult to find. Hence, in this concept analysis,
we aimed to formulate a definition of recovery in this specific
context, i.e. after surgery. The attributes have been identified,
6
four dimensions of recovery have been described, and the
definition of postoperative recovery produced from this
concept analysis is as follows:
Postoperative recovery is an energy-requiring process of returning to
normality and wholeness as defined by comparative standards,
achieved by regaining control over physical, psychological, social,
and habitual functions, which results in returning to preoperative
levels of independence/dependence in activities of daily living and an
optimum level of psychological well-being.
According to Walker and Avant (2005, p. 64), a concept
analysis should never be viewed as a finished product and ‘the
best one can hope for is to capture the critical elements of it at
the current moment in time’. We believe that the current
critical elements of postoperative recovery have been captured in our definition. Our concept analysis could be a first
approach in a theory-building process for postoperative
recovery. A practice-oriented theory could, for example, be
useful for nurses in clinical practice aimed at guiding actions
in this complex area. Our ongoing research projects concerned with postoperative recovery will give more knowledge
and should be useful in a future theory synthesis (Walker &
Avant 2005).
Conclusion
The concept of postoperative recovery lacks clarity, both in
terms of what postoperative recovery means to healthcare
professionals in their care for surgical patients, and in
understanding what researchers really intend to investigate.
The theoretical definition we have developed may be useful
but needs to be further explored.
Author contributions
RA, KB, EI and UN were responsible for the study conception
and design and the drafting of the manuscript. RA and UN
performed the data collection and data analysis. EI and UN
provided administrative support. RA, KB, EI and UN made
critical revisions to the paper. EI and UN supervised the study.
References
Aldrete J.A. & Kroulik D. (1970) Postanesthesia recovery score.
Anesthesia and Analgesia 49(6), 924–933.
Andreoli K.G. (1990) Key aspects of recovery. In Key Aspects of
Recovery (Funk S., Tornquist E. & Champagne M., eds), Springer
Publish, New York, pp. 308–314.
Baker C.A. (1989) Recovery: a phenomenon extending beyond discharge. Scholarly Inquiry for Nursing Practice 3(3), 181–194.
2007 The Authors. Journal compilation 2007 Blackwell Publishing Ltd
JAN: THEORETICAL PAPER
Baker C.A. (1990) Postoperative patients’ psychological well-being:
implications for discharge preparation. In Key Aspects of Recovery
(Funk S., Tornquist E. & Champagne M., eds), Springer Publish,
New York, pp. 308–314.
Bay-Nielsen M., Thomsen H., Andersen F.H., Bendix J.H., Sorensen
O.K., Skovgaard N. & Kehlet H. (2004) Convalescence after inguinal herniorrhaphy. British Journal of Surgery 91(3), 362–367.
Brown J.S. & Rawlinson M.E. (1977) Sex differences in sick-role
rejection and in work performance following cardiac surgery.
Journal of Health and Social Behaviour 18, 276–292.
Burt J., Caelli K., Moore K. & Anderson M. (2005) Radical prostatectomy: men’s experiences and postoperative needs. Journal of
Clinical Nursing 14(7), 883–890.
Encarta World English Dictionary, North American Edition.
Retrieved from http://www.encarta.msn.com/encnet/features/
dictionary/0550126 on 25 January 2005.
Hodgson N.A. & Given C.W. (2004) Determinants of functional
recovery in older adults surgically treated for cancer. Cancer
Nursing 27(1), 10–16.
Hogue S.L., Reese P.R., Colopy M., Fleisher L.A., Tuman K.J.,
Twersky R.S., Warner D.S. & Jamerson B. (2000) Assessing a tool
to measure patient functional ability after outpatient surgery.
Anesthesia Analgesia 91, 97–106.
Jakobsen D.H., Callesen T., Schouenberg L., Nielsen D. & Kehlet H.
(2003) Convalescence after laparoscopic sterilization. Journal of
Ambulatory Surgery 10, 95–99.
Kasl S.V. & Cobb S. (1966) Health behaviour, illness behaviour, and
sick-role behaviour. Archives of Environmental Health 12, 532–
541.
Kehlet H. & Dahl J.B. (2003) Anaesthesia, surgery, and challenges in
postoperative recovery. The Lancet 362(6), 1921–1928.
Kirkevold M., Gortner S.R., Berg K. & Saltvold S. (1996) Patterns of
recovery among Norwegian heart surgery patients. Journal of
Advanced Nursing 24, 943–951.
Kleinbeck S.V.M. (2000) Self-reported at-home postoperative
recovery. Research in Nursing and Health 23, 461–472.
Korttila K. (1995) Recovery from outpatient anaesthesia. Factors
affecting outcome. Anaesthesia 50(Suppl), 22–28.
Lawler J. (1991) The body in recovery, dying and death. In Behind
the Screens. Nursing, Somology, and the Problem of the Body
(Lawler J., ed.), Churchill Livingstone, Singapore, pp. 177–193.
Lee J. & Steven R. (2000) Recovery from surgery: grappling with an
elusive concept. Hospital Medicine 61(3), 189–192.
Leslie K., Troedel S., Irwin K., Pearce F., Ugoni A., Gillies R.,
Pemberton E. & Dharmage S. (2003) Quality of recovery from
anaesthesia in neurosurgical patients. Anaesthesiology 99, 1158–
1165.
Levine M.E. (1991) The conservation principles: a model for health. In
Levine’s Conservation Model: A Framework for Practice (Schaefer
K.M. & Pond J.B., eds), FA Davis, Philadelphia, pp. 1–11.
Marshall S.I. & Chung F. (1999) Discharge criteria and complications after ambulatory surgery. Anesthesia and Analgesia 88(3),
508–517.
Meleis A I. (2005) Theoretical Nursing: Development and Progress,
3rd ed. Lippincott-Raven, Philadelphia.
Postoperative recovery
Moore S.M. (1997) Effects of interventions to promote recovery in
coronary artery bypass surgical patients. Journal of Cardiovascular
Nursing 12(1), 59–70.
Myles P.S., Hunt J.O., Nightingale C.E., Fletcher H., Beh T., Tanil
D., Nagy A., Rubinstein A. & Ponsford J.L. (1999) Development
and psychometric testing of a quality recovery score after general
anesthesia and surgery in adults. Anesthesia Analgesia 88, 83–90.
Myles P.S., Reeves M.D.S., Anderson H. & Weeks A.M. (2000a)
Measurement of quality of recovery in 5672 patients after anaesthesia and surgery. Anaesthesia Intensive Care 28, 276–280.
Myles P.S., Weitkamp B., Jones K., Melick J. & Hensen S. (2000b)
Validity and reliability of a quality of recovery score: the QoR-40.
British Journal of Anaesthesia 84(1), 11–15.
Myles P.S., Hunt J.O., Fletcher H., Solly R., Woodward D. & Kelly
S. (2001) Relation between quality of recovery in hospital and
quality of life at 3 months after cardiac surgery. Anesthesiology 95,
862–867.
Nilsson G., Larsson S. & Johnsson F. (2002) Randomized clinical
trial of laparoscopic versus open fundoplication: evaluation of
psychological well-being and changes in everyday life from a
patient perspective. Scandinavian Journal of Gastroenterology
37(4), 385–391.
Nilsson U., Unosson M. & Kihlgren M. (2006) Experience of postoperative recovery before discharge – patient’s views. Journal of
Advanced Perioperative Care 2, 97–106.
Olsson U., Bergbom I. & Bosaeus I. (2002) Patients’ experiences of
the recovery period 3 months after gastrointestinal cancer surgery.
European Journal of Cancer Care 11, 51–60.
Parsons T. (1975) The sick role and the role of the physician
reconsidered. Milbank Memorial Fund quarterly. Health and
society 53, 257–278.
Pavlin D.J., Pavlin E.G., Horvath K.D., Amundsen L.B., Flum D.R.
& Roesen K. (2005) Perioperative rofecoxib plus local anesthetic
field block diminishes pain and recovery time after outpatient
inguinal hernia repair. Anesthesia and Analgesia 101(1), 83–89.
Steward D J. & Volgyesi G. (1978) Stabilometry: a new tool for the
measurement of recovery following general anaesthesia for outpatients. Canadian Anaesthetists’ Society Journal 25, 4–6.
Theobald K. & McMurray A. (2004) Coronary artery bypass graft
surgery: discharge planning for successful recovery. Journal of
Advanced Nursing 47(5), 483–491.
Walker L.O. & Avant K.C. (2005) Strategies for Theory Construction in Nursing, 4rd ed. Pearson Prentice Hall, New Jersey.
Werawatganon T. & Charuluxanun S. (2005) Patient controlled
intravenous opioid analgesia versus continuous epidural analgesia
for pain after intra-abdominal surgery. Cochrane Database of
Systematic Reviews CD004088, doi: 10.1002/14651858.
CD004088.pub2.
Wolfer J.A. & Davis C.E. (1970) Assessment of surgical patients’
preoperative emotional condition and postoperative welfare.
Nursing Research 19(5), 402–414.
Wordsmyth English Dictionary. Retrieved from http://www.
wordsmyth.net/live/home/050126 on 25 January 2005.
Zalon M.L. (2004) Correlates of recovery among older adults after
major abdominal surgery. Nursing Research 53(2), 99–106.
2007 The Authors. Journal compilation 2007 Blackwell Publishing Ltd
7