Muscle Mutability
advertisement

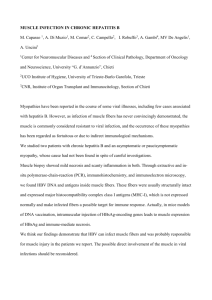
Muscle Mutability Part 1. General Concepts and Adaptations to Altered Patterns of Use STEVEN J. ROSE and JULES M. ROTHSTEIN During the past two decades investigators have shown that muscle fiber is highly mutable. A variety of stimuli ranging from patterns of use to the nutritional state of the organism may lead to alterations in fiber structure and function. The purpose of this review is to provide the information necessary to understand muscle fiber mutability (ie, terms and muscle fiber classification schemes) and to critically review the literature about mutability in response to altered patterns of use. The relevance of these studies to physical therapy is discussed, and suggestions for clinical applications are made. Key Words: Motor units; Muscle fiber types, predominance of; Muscle mutability. During the past 20 years animal and human studies have demonstrated that the muscle cells (fibers) of the skeletal motor unit have adaptive potential.1"3 This capacity of muscle fibers to adapt is remarkable in view of the muscle cell's high degree of biological specialization.4 Muscle is probably the most adaptable tissue in the body in response to a wide variety of stimuli involving patterns of use, pathological conditions, drugs, or metabolic factors. Many of the changes experimentally produced in muscle have been accomplished through procedures used in physical therapy, such as electrical stimulation, immobilization with cast, and exercise. The results of musclemutability experiments provide knowledge that can be used to develop guidelines for the more precise application of these treatment modalities. Clinically useful knowledge may also be gained from the work of investigators who have used animal models to mimic clinical conditions, such as disuse atrophy. In addition, researchers have examined the changes that take place in human muscle as a result of various diseases, metabolic conditions, and aging.5"8 Knowledge of muscle mutability allows the therapist to devise scientifically based treatment programs for correcting and preventing movement dysfunction. The purpose of this review is to present a selected summary of the vast body of literature pertaining to muscle fiber mutability in response to patterns of use and disuse. The response of muscle fibers to other stimuli, such as aging, drugs, and metabolic factors, are discussed elsewhere in this issue. However, to understand mutability of muscle fibers, regardless of the cause, an understanding of muscle fiber classifiVolume 62 I Number 12, December 1982 cation schemes and terms (eg, muscle fiber predominance) is essential. Knowledge of fiber classification schemes and of concepts such as predominance is needed for scientifically based clinical practice because therapeutic procedures apparently can lead to rather selective changes in different types of motor units.1'9'10 MUSCLE FIBER CLASSIFICATION SCHEMES A skeletal motor unit consists of a single alpha motoneuron and all the muscle fibers innervated by its axon.11 The innervated skeletal muscle fibers of the motor unit have been termed the muscle unit.12 A skeletal muscle, such as the biceps brachii or the quadriceps femoris, is made up of muscle units. A muscle unit is always associated with a specific type of motoneuron.13"16 The pairing of muscle units and neurons with complementary physiological properties produces a functionally unified biological element.12 For example, muscle fibers that are fatigue-resistant and can sustain tension for long periods of time are matched with motoneurons that are frequently activated.12 Through the use of standard histochemical17, 18 and biochemical19, 20 techniques, muscle biologists have demonstrated that in the absence of disease or injury, all muscle fibers within a motor unit are apparently identical. Therefore, muscle units are homogeneous. Each skeletal muscle, however, is heterogeneous; that is, it is composed of different types of muscle units.21 When mammalian muscle was shown to contain musclefiberswith different anatomical, physiological, 1773 Figure. Staining characteristics of human muscle fibers as regards myosin ATPase. Comparisons of serial sections allow for the classification of fibers into four categories: type I, the only dark staining fiber at the lowest pH; type HA, the only fiber that does not stain at a pH of 4.6; type IIB, the fiber that stains at a pH of 4.6 but not at a pH of 4.3; and type IIC, the fiber that stains intensely at pH levels of 10.3 and 4.6 but only moderately at a pH of 4.3. histochemical, and biochemical properties, the need to classify motor units and muscle units became essential. During the past 20 years, many schemes have been used to characterize the differences between the various kinds of units. Although there has been controversy and confusion concerning the validity or interpretation of the proposed classifications, three schemes seem to have gained the most acceptance. The differences between the schemes lie in the use of different variables for the classifications. Peter and colleagues examined muscle only and classified fibers (muscle units) according to biochemical, physiological, and histochemical properties.22 In contrast, Burke examined entire motor units and based his classification scheme on the physiological properties of the motoneuron and muscle fibers, as well as on the histochemistry of identified muscle fibers.12 Brooke and Kaiser used only histochemistry to classify fibers.23 Peter et al developed their classification scheme using whole and relatively homogeneous muscle.22 They studied animal muscles that consisted mainly of a single fiber type and compared the biochemical, histochemical, and physiological elements of these different "pure" muscles. Three classes of fibers were 1774 described based on contraction times and enzyme capacities, specifically oxidative and glycolytic enzymes: 1) fast-twitch, glycolytic (FG); 2) fast-twitch, oxidative, glycolytic (FOG); and 3) slow-twitch, oxidative (SO). Over a seven-year period, Burke conducted a series of important experiments on cat motor units that resulted in the formulation of another classification system.12 Triceps surae muscle motoneurons in the ventral horn of L7 and SI spinal cord segments were impaled with micropipette electrodes. To physiologically characterize and identify motoneurons, synaptic potentials were recorded in response to natural or electrical stimulation of specific input systems. Concurrently, the mechanical properties of the identified motor unit were studied by passing a depolarizing current through the electrode to cause contraction of the muscle unit. These contractions were recorded by a force transducer attached to the muscle's tendon and could then be characterized. Using the glycogen depletion method, Burke examined the histochemical profiles of physiologically identified motor units.12 This technique permits histochemical identification of the activated muscle unit by depleting its supply of glycogen through prolonged PHYSICAL THERAPY TABLE Muscle Fiber Classification Systems Brooke/Kaiser Peter et al 22 Burke12 23 Nomenclature Basis for Classification Classification System Histochemistry Myofibrillar ATPase (pre-incubations pH 10.3, 4.6, 4.3) Histochemistry Oxidative enzymes Glycolytic enzymes Myofibrillar ATPase Physiology Contraction characteristics of whole muscle Biochemistry (whole muscle) Physiology Contraction characteristics of motor units identified by glycogen depletion stimulation of the motoneuron. The glycogen-depleted muscle fibers (activated fibers) are then analyzed for their histochemical profiles. Data on motoneuronal properties were correlated with individual muscle unit contractile and histochemical characteristics. Burke divided the motor unit population into four categories: 1) fast-twkch, fast-fatigable (FF); 2) fast-twitch, intermediate fatigue-resistant (FI); 3) fasttwitch, fatigue-resistant (FR); and 4) slow-twitch, fatigue-resistant (S). Brooke and Kaiser developed a classification scheme that has become the standard method for classifying human muscle fibers.23 Their system is based on the pH lability of the myosin adenosinetriphosphatase (ATPase) enzyme. It was observed by Engel that type I fibers exhibit light staining after an alkaline preincubation, whereas type II fibers stain darker at the same alkaline pH level.6 Brooke and Kaiser demonstrated that with manipulation of the pH level of the preincubation medium, the following type II subclasses can be shown: IIA, IIB, and IIC. Type IIA fibers do not stain at a pH level of 4.6, whereas a pH level of 4.3 is required to inhibit the staining of the type IIA and IIB fibers. In general, the only fiber that stains intensely at an alkaline and an acid pH level is the type IIC fiber (Figure ). Because all the classification systems use different criteria for assigning names to muscle units and motor units, there is no clear-cut equivalence of units described by the different systems. Creating an equivalence table of all the fiber types would at present have questionable validity, and this is especially true for the subclasses of the type II fibers. However, to make generalizations and to avoid confusion in understanding the literature, a description of the relationships between the classifications is useful. The following is a generally accepted way of correlating the nomenclature and a brief description of the biological properties of each muscle fiber type (Table): Volume 62 / Number 12, December 1982 I MA IIB SO FOG s FR IIC FG Fl FF 1) Type I (SO, S) fibers have large amounts of oxidative enzymes and small amounts of glycolytic enzymes. These fibers primarily use aerobic metabolism, are associated with extensive capillary density, have a high number of mitochondria, and have wide Z bands.24, 25 These muscle units generate a relatively small amount of tension, have a slow contraction speed, and are resistant to fatigue. 2) Type IIB (FG, FF) fibers are well-supplied with glycolytic enzymes and are poorly endowed with oxidative enzymes, which indicates a high capacity for anaerobic metabolism. These fibers are associated with relatively sparse capillary density, have few mitochondria, and have narrow Z bands.25, 26 These muscle units generate a large amount of tension in a short time, but they fatigue rapidly. 3) Type IIA (FOG, FR) fibers possess intermediate amounts of oxidative and glycolytic enzymes, which indicates the use of both anaerobic and aerobic metabolism. These fibers have cytological properties that fall between the type I and type IIB fibers.26 These muscle units have relatively fast contraction speeds and intermediate tension-generating capacity and are resistant to fatigue. Two of the classification schemes—Burke's, based on a cat muscle and Brooke and Kaiser's, based on human muscle—include a third subclass of type II fiber. Burke describes a fast-twitch unit with intermediate fatigue resistance (FI). The Brooke and Kaiser classification includes a type IIC fiber. Regardless of the classification scheme used, these fibers usually make up a small percentage of the total fiber populations. Very little is known about the FI or type IIC fibers, and it is not clear whether they are the same. In an attempt to describe the general characteristics of muscle units, we have, by necessity, made some assumptions. These descriptions are based on observations of untrained human and animal muscle. As will be discussed later in this review, some of the metabolic properties of muscle can be modified with 1775 altered patterns of use. Some authors prefer to use the myosin ATPase approach of classification because it is least affected by training-induced changes. Saltin et al discussed at length some of the difficulties that occur when classification of fibers is based on metabolic enzymes.26 MUSCLE FIBER TYPE PREDOMINANCE The distribution of motor units in humans is very different from that in animals. In animal muscle there are many muscles that have a predominance of either fast- or slow-twitch units and this is true for any member of that species; for example, in all rats, the soleus muscle is slow. In humans this does not appear to be the case. The proportion of fibers of any given type varies greatly between individuals (one person may have a greater percentage of slow-twitch units in their vastus lateralis muscle than another person has).21 However, when muscles of many people are examined and the fiber proportions are averaged, the ratio of fast- to slow-twitch fibers is usually 50:50.21 Humans, therefore, tend to have almost equal numbers of the two major fiber types in most muscles. When the muscles of an individual are compared, variability between muscles is observed; the fiber proportions in the vastus lateralis muscle, for example, may be very different from the proportions in the rectus femoris muscle of the same subject.21 Muscle fiber type predominance is said to exist when the percentage (number of fibers) of a given muscle unit type is extremely large within a specific muscle or when compared with another muscle.7 Existing evidence suggests that muscle fiber type predominance is genetically determined.27 When predominance of one fiber type has been demonstrated in a muscle, for convenience the whole muscle has been referred to as "fast" or "slow." Clinical Significance Muscle fiber type predominance has become an issue in sports medicine. Athletes often have a high proportion of a fiber type that allows them to excel in their particular sport.26-35 Marathon runners, for example, have a high proportion of slow-twitch muscle units.26 However, there is general agreement that other factors, such as motivation, coordination, and learning may be equally important for athletic success.28, 35 Whether training can induce a change in fiber type predominance is still unresolved. Theoretically, muscle dysfunction may give rise to joint dysfunction, which may make fiber type predominance important clinically. For example, an individual who has a low proportion of slow-twitch muscle units might be susceptible to joint injury when performing tasks that require endurance. The muscle 1776 may fatigue and be unable to protect the joint from excessive loading. On the other hand, an individual with a low proportion of fast-twitch units might have a decreased capacity to produce a fast rise in tension in response to sudden loads. This failure to develop tension rapidly might lead to excessive joint loading, causing joint destruction. Although the above hypotheses are speculative at present, they are based on concepts derived from experimental data. Radin, in his work done with others, demonstrated that the most destructive forces applied to cartilage are impulse loads.36 These loads require cartilage to absorb shock at a rate beyond its capability. Radin has postulated that impulse loading may be a major cause of osteoarthritis (or osteoarthrosis as he prefers to call it because of its noninflammatory origin). He also concluded that it is the shockabsorbing quality of muscle action that prevents cartilage destruction by impulse loading. The eccentric contraction, which Hill described as doing negative work,37 appears to be the mechanism that is used to save cartilage from the effects of impulse loading. In view of the suggested role of muscle in sparing cartilage, we believe that muscle must be capable of welltimed and appropriately modulated contractions. According to the model proposed by Radin, without the appropriate amount and rate of tension development, joint destruction would be almost assured. Sirca and Susec-Michieli examined the muscle fibers of subjects with osteoarthritis.38 Those authors do not discuss the possibility that their finding a loss of type II fibers is a potential cause rather than a result of the disease. We must emphasize the word "potential" because the notion that inappropriate fiber predominance might lead to osteoarthrosis is highly speculative. However, it is a intriguing thought and points out the importance of considering how inadequate muscle performance could contribute to a mechanical disruption of joints. Research is needed before a definitive link can be shown between patterns of muscle fiber predominance and joint dysfunction. However, others have also suggested inappropriate muscle action may be a cause of joint pain.39-42 Until research determines whether a link does exist, we advise clinicians to consider the possible contribution of muscle to joint dysfunction. MUTABILITY PARADIGMS Although many experimental paradigms have been used to alter the properties of muscle fibers, these experimental approaches can be grouped into four major categories. One paradigm places muscle fibers in a state of reduced activity or disuse.43, 44 The assumption is made that the muscle fibers are then experiencing a decreased metabolic demand. Immobilization, tenotomy, and the elimination of descendPHYSICAL THERAPY ing influences on lower motoneurons are examples of procedures used to eliminate or reduce activity in the motor units.45, 46 The second experimental model is one in which there is increased use of the muscle fibers.4'46 In this case, there is an increase in the metabolic demand placed on the muscle fibers. Electrical stimulation, exercise, and compensatory hypertrophy produced by denervating one muscle of a synergistic group are methods used to produce increased use of a muscle.4, 10, 46 The third paradigm involves the use of drugs such as anabolic and catabolic steroids.47"49 The fourth experimental model is based on the manipulation of the muscle fiber's metabolism, for example, through the use of malnutrition paradigms.50, 51 All the experimental paradigms provide information that can be used for clinical practice. The relevance of studies examining the effects of use and disuse is apparent. Less obvious is the need to understand the effects of drugs, such as corticosteroids, which are commonly used for a variety of diseases.7, 52 Knowing that the steroid-treated patient has a selective type II atrophy means that exercises should be performed that hypertrophy that fiber. Similarly, by understanding metabolic studies, therapists can be better prepared to treat the type II fiber area loss of the cachectic cancer patient or of the malnourished patient (eg, a patient with Crohn's disease).7 This review will focus only on the changes in fibers seen with varied patterns of disuse and increased use that provide the basis for understanding all mutability studies. Metabolic factors, drugs (including alcohol), and the effects of aging are discussed elsewhere in this issue. REDUCED ACTIVITY AND DISUSE PARADIGMS The most obvious changes that clinicians observe resulting from disuse is loss of muscle mass. Classically, we have referred to this as atrophy, a nonspecific term that describes the muscle as if it were a homogeneous entity. Experimentation on humans and animals has demonstrated that disuse atrophy is a complex phenomenon whose effects vary with fiber types and with different muscles. Experiments using immobilization of limbs provide a nonsurgical disuse model that is analagous to what is seen in orthopedic patients who have been immobilized in casts. By understanding the results of these experiments, we can be better equipped to manage patients with atrophy brought about by cast immobilization. Cast Immobilization Cast immobilization of normal animal muscle results in preferential atrophy of slow-twitch fibers. Volume 62 / Number 12, December 1982 These fibers decrease in size and lose some of their capacity for oxidative metabolism.44 Cast immobilization results in a decreased rate of protein synthesis in all muscle fibers, with type I fibers showing the greatest decrease.44,53 A physiological change also takes place in the type Ifibers:they increase their rate of tension development after having been immobilized.44, 54 The change in the contraction speed of immobilized slow-twitch muscle fibers is unique. There is no other known stimulus likely to occur in normal animal muscle that leads to a change in contraction time.1 In addition to the changes that take place within the slow-twitch fibers, there is evidence that in the soleus muscle (a predominantly slowtwitch muscle) of the rat and the guinea pig a loss in the number of slow-twitch fibers occurs.55, 56 This loss could explain the overall increase in contraction times for those muscles. However, there is currently a controversy over whether slow-twitch fibers preferentially degenerate, or whether the loss in number of slow-twitch fibers is a result of some being converted to fast-twitch fibers.44 Although fiber-specific changes after immobilization have been repeatedly examined in animal muscle, only a few studies have been done with humans. And as might be expected, the results from human studies present a less cohesive picture than the one presented in animal studies. Sargeant et al studied seven patients whose lower extremities had been in casts for an average of 131 days (range, 53-213).57 All patients had unilateral fractures. Needle biopsy specimens were obtained bilaterally from the lateral part of the quadriceps femoris muscle. Fiber type distribution and area were calculated for 50 to 100 fibers. When the muscle that had been in the cast was compared with the muscle of the uninvolved lower extremity, it was found that 1. There was no change in the numbers of type I and type II fibers. 2. Type I fibers showed a greater atrophy (loss of area) than the type II fibers in six of the seven patients. The average type I loss was 46 percent, and the average type II loss was 37 percent. 3. Overall, there was a 42 percent decrease in mean fiber area. These results support the following conclusions: there was no fiber type conversion (eg, type I fibers did not become type II), and there appears to have been no selective degeneration (eg, loss of a specific fiber type). In addition, this study extended to humans the finding of preferential type I fiber atrophy as found with cast immobilization. Although cast immobilization allows for the investigation of muscle changes in humans, there is a major problem associated with this method when the uninvolved limb is used as a control for the comparison of 1777 fiber area and frequency: use of this limb is likely to increase during the period of cast immobilization. Therefore, in this study it was possible that while one limb was undergoing disuse, the other limb may have been changing because of increased use. This increased use, as might occur with crutch walking, could have led to compensatory hypertrophy (increase in cross-sectional area) of the type II fibers. It should be remembered that subjects in this study were immobilized in the casts for long periods of time (53-213 days). Recently Haggmark et al reported on the effects of casts applied to another population sample: eight men and one woman from 25 to 40 years of age who underwent surgical reconstruction of the anterior cruciate ligament (a modified Jones procedure).58 At the time of surgery, biopsy specimens were taken from the vastus lateralis muscles of both the involved and uninvolved legs. The legs were then immobilized for five weeks. During the time of cast immobilization all subjects performed isometric excercises of the involved extremity. These consisted of contractions lasting three to six seconds, followed by rest periods of six seconds. Initially, patients had difficulty doing these exercises because of pain; however, Haggmark et al reported that after a couple of days subjects were able to "retrieve" their muscle function. The subjects progressed to the point of doing the excercises for one hour. Also, during the time they were in the cast, subjects were allowed to use the limb for ambulation within pain tolerances. After removal of the casts another biopsy was taken. Also, preoperative and postoperative measurements of thigh circumference were compared, and a decrease in circumference was evident. Histochemical analysis showed that there was a loss of area only in the type I fibers when preoperative and postoperative values were compared. Biochemical analysis of single fibers demonstrated a loss of succinic dehydrogenase (SDH, an oxidative enzyme) activity in the type I fibers. There were no changes in the area or in the metabolic activity of the type II fibers of the operated limb or in either fibers of the uninvolved limb. The type I fiber atrophy, which involved both fiber size and loss of metabolic capacity, occurred despite the use of isometric exercises. Although it is impossible to say whether the exercises lessened the degree of atrophy, the results demonstrate that isometrics did not prevent atrophy in these patients. The type I atrophy demonstrated by Haggmark et al with patients who had undergone knee surgery is in contrast to the mixed atrophy demonstrated by Sargeant et al with patients with fractures. Several explanations may be offered for the apparent discrepancy. One factor may have been methodological. As was noted previously, Sargeant et al used the uninvolved limb as a control for comparison values. 1778 Haggmark et al used the preoperative values as a control, and therefore the results could not have been affected by changes in the uninvolved limb that might have occurred with altered patterns of use. Also, Haggmark et al's subjects were in casts for a much shorter period of time but probably had more pain than Sargeant et al's. Gydikov suggested that pain has a greater inhibitory effect on the motoneurons of the type I fibers than on the motoneurons of the type II fibers.59 The type I atrophy Haggmark observed may have been caused by pain rather than immobilization. There remains a controversy over the type of atrophy seen in patients after cast immobilization. Muscle pathologists have observed type II atrophy after cast immobilization, unless the patient was in severe pain (personal communication from M.H. Brooke, July 1982). This observation may strengthen the argument that Haggmark et al's findings were related to the effects of pain rather than of the cast. However, the observation cannot explain the mixed atrophy reported by Sargeant et al. At the present time, clinicians might want to assume that a mixed atrophy exists in cast-immobilized patients and plan their exercises accordingly. Rehabilitation of the cast-immobilized patient apparently must include exercises that improve endurance as well as strength. The need for exercises that combine strength and endurance training is reinforced by the results of a series of experiments that combined training with cast immobilization in human volunteers.60, 61 MacDougall et al examined muscle metabolite concentrations in nine men who had trained and had been immobilized in a cast.60 Biopsy samples from the long head of the triceps brachii muscle were taken from subjects who had their forearms immobilized in casts for five weeks. Subjects were divided into two groups. One group trained before cast immobilization and the other after. A biopsy was taken from each subject at the initiation of the study, after the casts were removed, and after training. Metabolites measured were adenosine triphosphate (ATP), adenosine diphosphate (ADP), creatine (C), creatine phosphate (CP), and glycogen. Immobilization significantly reduced CP concentrations by 25 percent and glycogen concentrations by 40 percent. Muscle homogenates were used for biochemical analysis, and as a result, fibers could not be identified where the metabolites were lost. Of clinical interest was the interaction between training and immobilization; subjects who had trained before immobilization showed a greater loss of metabolites; however, the group that trained after immobilization demonstrated a greater increase in metabolite concentrations as a result of training. MacDougall et al's findings suggest that cast immobilization may in some ways be more deleterious to the well-trained athlete than to the sedentary inPHYSICAL THERAPY dividual. For the athlete, immobilization possibly results in greater disuse and therefore leads to even greater relative loss of muscle metabolic properties. Conversely, the increased training effect seen in subjects who exercised after immobilization indicates that for these subjects, exercise represented even greater relative use. The results reported by MacDougall et al suggest that on a relative basis, deconditioned subjects may respond better to postimmobilization rehabilitation programs than do well-trained athletes. It would appear that athletes need special consideration following immobilization in order to attain their previous high level of performance. Although the most obvious treatment would be to exercise with very high loads, this strategy would not deal with the loss of endurance capacity found in immobilized human muscle. However, it should be noted that both of the metabolites found by MacDougall et al to be diminished, CP and glycogen, are associated with the production of ATP during the early phases of forceful muscle contractions. Concentrations of these metabolites are known to increase as a result of high-power exercise.60 In a follow-up study, MacDougall and associates used the same experimental design of taking biopsies before and after sequential immobilization and training of the triceps brachii muscle.61 In this follow-up study, histochemical staining was used to type fibers and to examine the changes in fiber area and frequency. The group that trained before immobilization consisted of four men, and the group that exercised after cast removal consisted of three men. Subjects were in casts for five weeks. Immobilization led to a decrease in the areas of both major fiber types: type I fibers decreased 25 percent and type II fibers decreased 33 percent. This decrease in type II fiber area did not appear to be dependent on when the subject had trained. Fiber area was similarly reduced in the group that trained before immobilization and in the group that was to begin exercise after immobilization. This finding indicates that cast immobilization, relative to fiber area, causes similar atrophy in trained and untrained muscle. The results of this experiment on the triceps brachii muscle are different from the results Sargeant et al and Haggmark et al reported on the quadriceps femoris muscle. They found a preferential type I fiber atrophy, similar to that found in animal studies. Although MacDougall and associates reported a mixed atrophy, the type II fibers actually showed a greater loss in area.61 Further research will be required to determine whether the apparent discrepancy between these studies is due to inherent differences in the muscles, duration of immobilization, presence of pain, or experimental methods. A critical observation also may be made relative to what appear to be inconsistencies in the two studies Volume 62 / Number 12, December 1982 of MacDougall. In the first experiment, decrease in metabolic substrate was dependent on prior training. In the second study, decrease in cross-sectional area of the type II fibers was not dependent on prior training. Cast immobilization had a more deleterious effect on metabolite concentrations in trained muscle than in untrained muscle, whereas it had the same effect on the cross-sectional area of trained and untrained muscle. These findings illustrate the complex nature of atrophy and the need to define and to understand the term in clinical practice. Subjects with trained muscle seem to be more susceptible to one effect of cast immobilization, specifically loss of ATP precursors; they are not more susceptible to the loss of fiber area. Therefore, clinical evaluation of the cast-immobilized patient should include assessment of prior training and activity levels. Joint Dysfunction and Tendon Rupture Cast immobilization is one situation in which muscle use is significantly reduced. Other clinical conditions in which inactivity leads to significant changes involve joint dysfunction and tendon ruptures. Edstrom described preferential atrophy of type I fibers in the vastus medialis muscle of patients with long-standing anterior cruciate ligament injuries.62 Biopsy specimens were taken from 10 subjects (9 of whom were athletes) at the time of arthrotomy. He reported that of the 4 subjects with the most pronounced signs of atrophy, 3 exhibited the greatest degree of joint dysfunction and appeared to have the most disability. The changes that take place in the muscle of patients with osteoarthritis of the hip have been described by Sirca and Susec-Michieli.38 In younger patients with osteoarthritis (37-64 years of age), they reported a decrease in the percentage of type II fibers in the gluteus medius, gluteus maximus, and tensor fasciae latae muscles. In older patients with osteoarthritis (65-78 years) a decreased percentage of type II fiber was found only in the gluteus medius and the tensor fasciae latae muscles. In the older group, the percentages in the gluteus maximus muscle did not differ from age-matched autopsy controls. In the younger group, there was a decreased fiber diameter for both type I and type II fibers in the gluteus medius and the tensor fasciae latae muscles. The diameter of type II fibers decreased in the gluteus maximus muscle, whereas the diameter of the type I fibers was similar to that of the controls. The pattern of atrophy in the gluteus maximus muscle clearly differs between the two age groups, but the significance of this finding has yet to be investigated. The findings of Sirca and Susec-Michieli cannot be explained on the basis of aging because each of their groups was compared with age-matched autopsy con1779 trols. It is clear, however, that the mixed pattern of muscle atrophy in patients with osteoarthritis differs from that seen in patients with cast immobilization and ligamentous injuries of the knee. It has not been determined whether this difference is caused by some factor associated with the disease process, such as loss of motion or pain, or is representatve of a unique activity pattern, or is caused by some other factor. Following rupture of the bicipital tendon, Jozsa et al found that there was a reduction in the area of type I fibers and a decrease in the percentage of type I fibers in the long head of the biceps brachii muscle.63 The area of the type II fibers remained the same. Comparisons of nine subjects were based on biopsy samples from the uninvolved arm. Because the time from tendon rupture to biopsy and repair varied from one day to six months, it was difficult to assess the rate of atrophy in these patients. However, it appeared that fiber area changed similarly in all patients, whereas fiber number appeared to depend on length of time since tendon rupture. INCREASED ACTIVITY AND USE PARADIGMS Disuse has been shown to cause changes in almost all muscle characteristics. Similarly, increased use of muscle also leads to a wide variety of changes. The most obvious method for increasing use is the lifting of heavy loads for a relatively low number of repetitions (strength training). This exercise usually results in an increased muscle mass and is probably the only paradigm for increased use that produces muscle hypertrophy.64 This paradigm may be contrasted to situations where the muscle works against a light load for a relatively large number of repetitions. This latter form of exercise has been called endurance training and results primarily in altered metabolic characteristics within muscle fibers.65 Although, clinically, endurance training has been considered only from the standpoint of load and repetitions, there is another critical variable that affects the type of changes muscle undergoes. This variable is intensity, relative to maximal oxygen uptake of the individual.66 When high-intensity exercise is performed for a period of time, the changes that take place in the muscle are different from those seen with traditional strength and endurance exercises.26, 67-69 Muscle responds to use in a wide variety of ways that are dependent on the exact nature of the training stimulus. To fully understand the effects of clinical procedures, a conceptual framework that relates all possible stimuli and responses must be developed. Low Loads and High Repetitions To investigate the response of muscle to low load and high repetitions (increased frequency of use), 1780 Salmons and Henriksson4 developed just such a conceptual framework based on the transformation of type II to type I fibers. They have suggested that when an increased metabolic demand is placed on muscle through endurance training or chronic electrical stimulation there is a "hierarchy of stability" of muscle properties that can be demonstrated by systematically changing that functional demand. The early changes seen with chronic electrical stimulation of muscle are similar to those seen with endurance exercises.4 Apparently, each mutable property of muscle has a different threshold of use that must be reached before change can occur.70 The thresholds for these various properties, such as metabolism and contraction speed, fall along a continuum. There is a consistent sequence of changes that occur in muscle that is directly related to the type and duration of use. Salmons and Henriksson reviewed a series of experiments with chronic electrical stimulation that demonstrated fiber transformation from fast twitch to slow twitch.4 The documentation of the sequential changes that occurred during these fiber transformations has given us a framework for explaining the variety of results of experiments examining the effects of increased muscle use. Electrical Stimulation Fiber transformation from type II to type I has been accomplished in animals primarily through the use of indwelling electrodes that delivered 10 Hz pulses continuously to motor nerves for six weeks or more.4 Contractions obtained in this way were palpable but not very forceful. By sacrificing animals at intervals during this stimulation period, the changes that occurred could be recorded. It was discovered that at various stages of stimulation, the different muscle properties were changing. For example, after one week, changes in capillary density could be seen, and after two weeks, changes in rate of tension development could be observed. The following is a compilation of some of these changes from a variety of experiments:4 Within one week: Increased capillary density was observed as was an increased resistance to fatigue. Cytological changes (eg, decreased T system) associated with type I fibers were found. Within two weeks: Oxidative capacity increased along with mitochondrial volume. Glycolytic enzymes were reduced. Cytological changes (eg, increased Z disk thickness) consistent with type I fiber transformation were found. There was also a loss of sarcoplasmic reticular proteins and decreased activity of calcium uptake. At this point, the muscle also took on the isometric contraction characteristics of the type I fiber with increased time-to-peak tension and increased time-to-half relaxation. PHYSICAL THERAPY Within three weeks: Myosin ATPase activity was reduced. Three to eight weeks: Changes occurred in contractile and regulatory proteins consistent with fiber transformation. Eight weeks: The maximum velocity of shortening under isotonic conditions was significantly reduced. These experiments examined whole muscle, and it was noted that after fiber transformation the whole muscle may actually become even slower than normal slow muscle. This may have happened because after stimulation the muscle was completely slow-twitch, whereas normal slow muscle, such as the soleus muscle, usually contains some fast-twitch fibers.4 Experiments in which electrical stimulation was discontinued showed that reversal of fiber transformation (return to fast twitch) takes place with the sequence of events reversed. During the process of transformation of type II to type I, there was no change in the number of fibers in the muscle. However, the area of the fibers decreased. In this review we have reported that electrical stimulation results in fiber transformation. Several alternate hypotheses to explain these results have been made. A complete listing of those and a discussion of why they may not be valid are presented by Salmons and Henriksson.4 The electrical stimulation used in the studies described above was essentially low frequency and chronic (continuous). To determine whether the critical factor was frequency or stimulus duration, Sreter et al examined the effects of 60 Hz stimulation (for five weeks) on the fast extensor tibialis anterior muscle of the rabbit.71 The results were similar to those found with 10 Hz stimulation. Because the 60 Hz stimulation resembled the discharge frequency of fast motor units, the results suggest that the amount of activity a muscle engages in, rather than the discharge pattern, may be the critical stimulus for fiber transformation. Sreter et al, however, found one difference when the higher frequency pattern was imposed on muscle. Normally, muscle undergoing fiber transformation from 10 Hz stimulation loses between 30 and 50 percent of its mass compared with the nonstimulated leg. With 60 Hz stimulation, no change in mass was found. This may imply that the muscle fiber type is dependent on the degree of overall activity, whereas muscle mass may be related to the pattern of use. It should be noted that attempts to convert denervated slow muscle to fast muscle72'73 have not provided clear-cut results that can be used to understand stimulus variables needed for this type of fiber transformation. One study examined the effects of electrical stimulation on human muscle fibers. In an attempt to reduce "refractory" knee flexion contractures, Munsat et al stimulated the femoral nerve with implanted Volume 62 / Number 12, December 1982 electrodes in five patients.74 When phasic stimulation (33 Hz every four hours for one hour; 5 seconds on, 25 seconds off) was performed on four patients with fixed contractures of the knee, isometric contractions resulted. In the fifth patient, a surgical release of the rectus femoris muscle allowed the stimulation to produce a more isotonic contraction of the muscle because the muscle could shorten. In the four patients with isometric contractions, the number of type I fibers increased and both type I and type II fibers increased in size. In the patient with a tenotomized muscle, the number and size of type I fibers decreased. The results of Munsat et al's study are intriguing and suggest that electrical stimulation variables and the type of muscle contraction (ie, isometric or isotonic) must both be considered determinants of fiber transformation. However, their findings must be applied cautiously in view of the following limitations of the study: 1) the isotonic condition in this study also involved tenotomy, and as a result there was no "true" isotonic contraction (there was no resistance); 2) the results are based on four subjects in one group and one in another; 3) these patients may not have had normal muscle at the beginning of the study as a result of their longstanding contractures, because these quadricep femoris muscles had undergone contracture-induced immobilization in a lengthened position (knee flexion). The electrical stimulation experiments detail how and when muscle changes. To apply this information to the clinical setting, it is necessary to review some of the experiments that deal with endurance training. Endurance Training In animals, repeated experimentation has shown that with endurance training, such as long distance running, the primary effects involve alteration of the fibers' metabolic capacity.65 There is an increase in the respiratory capacity of muscle (eg, increased mitochondrial volume); a rise in the ability to generate ATP via oxidative phosphorylation by metabolizing fats, carbohydrates, and ketones; an increase in myoglobin content; and increased capillary density. Therefore, the changes that take place with endurance training are similar to those that occur during the early phases of chronic electrical stimulation. The only difference in effect between endurance training and chronic electrical stimulation is that endurance training apparently cannot significantly change muscle contraction characteristics.4 With chronic electrical stimulation, muscle is in constant use, whereas during even the most rigorous endurance programs, muscle is only intermittently active. Contractile characteristics, such as speed of contraction, have been 1781 shown to be among the last properties of muscle to endurance capacity of the high-tension developing transform during electrical stimulation. Although en- type II fibers. This finding has implications for rehabilitation. durance training is a potent stimulus for muscular changes, it appears that it cannot be carried out for Patients who will be required to function at relatively long enough periods of time to lead to changes in low work loads, with relatively low tension developmuscle contraction characteristics or to alter the re- ment, can be trained at low intensities. However, if a lated properties of myosin ATPase. Chronic electrical patient needs to function for prolonged periods of stimulation brings about total change in muscle char- time at high work loads, with possibly high levels of acteristics because it is a stimulus that leads to the tension required, they must undergo high-intensity highest level in the hierarchy of change; endurance endurance training. The extension of the findings on endurance training to patients is at present our hytraining does not reach that level.4, 70 Human muscle appears to respond to endurance pothesis and has not yet been proven valid by clinical training in much the same way as animal muscle, that research. is, with increases in oxidative capacity.26, 31, 65, 75-77 Conversion of the various subtypes of type II fibers However, this increase in oxidative capacity occurs in has been shown by Andersen and Henriksson.68 With different muscle cells, depending on the intensity of submaximal exercise (30 minutes, four days a week the exercises relative to maximal oxygen uptake for eight weeks at 81% Vo 2 max ), type IIB fibers were (Vo2max). Gollnick et al found that when subjects converted into type IIA fibers. Because the type IIA exercised intensely (from 75-90% Vo 2 max ) one hour fibers have a greater oxidative capacity, this result a day, four days a week for five months, histochemical may have been expected. A more controversial findstaining showed an increase in oxidative capacity in ing was reported by Jansson et al, who contend that both type I and type II fibers of the vastus lateralis with appropriate training there can be interconversion muscle.75 of type IIC and type I fibers.69 Jansson et al reported that some type I fibers Henriksson and Reitman used biochemical analysis to examine the training effect when intensity was convert to type IIC fibers during "anaerobic training" varied.67 This method is a more sensitive means of (running at 90-100% Vo 2 max two or three times a assessing enzyme changes than the histochemical week for a total of 44 miles). They also reported that method used by Gollnick et al. Henriksson and Reit- with "aerobic training" (running at 70-80% Vo2 max man showed that when subjects exercised at about 80 for a total of 68.2 miles a week) conversion in the percent Vo 2 max for 27 minutes a day, three days a opposite direction took place: type IIC fibers became week for eight weeks, there was a significant increase type I fibers. This report is the only one in the in SDH activity of the type I fibers of the vastus literature to make the suggestion that training can lateralis muscle. Another group of subjects trained at convert type II fibers to type I fibers. Fiber conversion about 92 percent Vo 2 max for three days a week with through training is a controversial suggestion, and five work periods separated by two minutes of rest. one must take into account that the level of training These subjects, who exercised at an intensity that for Jansson et al's anaerobic paradigm was extraorapproached their maximum capacity, showed an in- dinarily intense. Most endurance training appears crease in SDH activity in only the type II fibers. With incapable of producing the threshold needed to convery high intensity endurance training, only the oxi- vert type II fibers to type I fibers. dative capacity of the type II fibers increased. With Another endurance study suggested that the type low intensity exercise, oxidative capacity increased IIC fiber is really an intermediate form between the only in the type I fibers. In both the high and low type I and type II and that the IIC is a fast, endurant intensity groups, there was no change in phospho- fiber.25 Ingjer used an interval training approach: the fructokinase activity. The stability of this glycolytic subjects ran 45 minutes three days a week, one day at enzyme indicates that in neither group was there an 50 to 90 percent Vo 2 max and the other two days increased capacity for anaerobic metabolism. intermittently at 100 percent Vo 2 max for 24 weeks.25 Increased oxidative capacity is the result of endur- (Not surprisingly, only seven of the original 15 subance training and occurs in the type I fiber when the jects completed the study.) After training, there was intensity of work is low and in the type II fiber when an increase in the percentage of type IIA fibers and the intensity is high. Therefore, endurance training is a decrease in the percentage of type IIB fibers, sugnot a single form of exercise and certainly does not gesting a conversion between the two types. Ingjer lead to similar changes in all muscle. Response to proposed that this took place via a type IIAB fiber 78 endurance training is dependent on the level of work that was previously described by Gronnererod et al. and effort during the training. Low-level endurance These IIAB fibers, which are not included in most training will increase the oxidative capacity and, classification schemes, have a size, capillary supply, therefore, endurance of the low-tension developing and mitochondrial content intermediate between type type I fibers. High-intensity work will increase the IIA and type IIB fibers. Another finding of Ingjer's 1782 PHYSICAL THERAPY was that the type IIC fiber, which is relatively uncommon, increased in number from 0.4 percent to 2.29 percent after training. Because this type IIC fiber resembled the type I fiber cytologically and enzymatically, Ingjer argued that the IIC may be derived from the type I fiber. In every circumstance, endurance training improves the oxidative capacity of muscle. When intensity is low, this improvement is restricted to the type I fiber. When intensity is high, the improvement occurs in the type II fiber and probably is accompanied by conversion of the type IIB fiber into a type IIA fiber. The possibility exists that type IIC fibers may be converted under extreme training conditions into type I fibers. Because the only evidence for conversion through training comes from a paradigm with high intensity, the hierarchical model of Salmons and Henriksson may be applicable.4 This model states that changes take place along a continuum and that as stimulus intensity and duration increase, the changes that take place in a muscle increase. Total fiber conversion may be possible only under the most extreme circumstances. It must be emphasized, however, that this hierarchical model was based on animal experimentation. If the same type of process with similar time courses is shown to exist in humans, then exercise programs may be developed that could vary specific muscle properties by working up to the desired level in a hierarchy. Muscle Use and Development Muscle mutability demonstrated through electrical stimulation and endurance experiments has provoked some questions about how muscle development may be affected by patterns of muscle use. According to Salmons and Henriksson, there is in the fetus a unique form of myosin, the most abundant muscle protein, whereas the other muscle proteins are biochemically similar to those seen in adult fast-twitch muscle.4 At birth, or shortly thereafter, type I fibers appear. The number of type I fibers at birth varies greatly between species and is apparently dependent on how mature the organism is at the time of birth. According to Salmons and Henriksson, development of type I fibers proceeds postnatally in a fashion that is "reminiscent of the changes evoked in adult fast twitch muscle by chronic low frequency stimulation, suggesting that the emergence of slow-fiber properties in the course of ontogenetic development could be contingent on the establishment of definitive patterns of motor activity in the maturing nervous system."4(p101) This would suggest that developmental approaches to patient care that have focused primarily on the nervous system79 may have been promoting normal ontogenetic development of the highly mutable maturing muscle. This hypothesis, which would Volume 62 / Number 12, December 1982 offer new scientific foundations for some physical therapy treatment strategies, needs to be investigated further. The possibility that developmental intervention may be a stimulus for normal development in the periphery, namely in the muscle, is a provocative concept. Strength Training All of the preceding discussion relating to increased use is based on two conditions: either the intensity relative to V0 2 max was varied, or the subjects worked against low loads for many repetitions. Both of these conditions relate to the concept of endurance. The next important type of use paradigm deals with maximal efforts, something traditionally referred to as "strength training." Generalization of the results of strength training studies is difficult because the term strength, as applied to exercise, has no single meaning. Strength is usually operationally defined in each study. What makes interpretation of strength training literature even more difficult is the use of what therapists might consider nonspecific forms of exercise. For example, one group examined changes in the fiber composition of the vastus lateralis muscle after subjects exercised by doing squats,34'64 an exercise that involves not only the knee extensor muscles but much of the hip musculature. Further confusion has been created by studies in which strength training consisted of multiple exercises that may or may not have been accomplishing the same goal.60, 80 Despite the multiple sources of confusion that seem to dominate the strength training literature, the following general observations can be made: 1) type II fiber area increases in response to heavy resistance training61; 2) type II fiber area appears to correlate with the maximal isometric strength81-84; 3) there is no definitive picture as to the changes that take place in the fiber's metabolic capacity1, 60, 85; and 4) myofibrillar proteins increase, resulting in enlarged or hypertrophic muscle fibers.1, 9, 10 Beyond these generalizations, it is difficult to discuss strength training because of the problems listed above. The readers are urged to examine the following references for a view of some of the strength training literature: MacDougall et al,60, 61, 80 Thorstensson,64 Nordemar et al,81 Grimby et al,82 Costill et al,85 Komi et al,86 and Thorstensson et al.87 The effects of strength training described above are generally agreed upon. However, there is an additional effect that has been infrequently observed and is highly controversial—fiber splitting. Advocates of fiber splitting as an effect of strength training believe that when a muscle cell hypertrophies, it reaches a maximum size and, therefore, further hypertrophy is impossible. They suggest that additional strength 1783 gains can only be made through the addition of fibers, which occurs when existing fibers (cells) divide and split. Gonyea and associates in different studies have been the primary advocates of thefibersplitting effect and have reported seeing the phenomenon in exercised cat muscle.88-90 Those who believe in fiber splitting remain a minority in the field of muscle biology. Experiments demonstrating fiber splitting have yet to be replicated. One of the major reasons why fiber splitting has not been conclusively demonstrated in response to training is the possibility that fiber splitting is not really biological but rather an artifact of the way muscle is prepared for morphological analysis. The studies that have reported fiber splitting in response to training have been done in animals. Fiber splitting is also known to occur in human muscle but has always been associated with a dystrophic process or some other disease.91 One group reported the effects of strength training programs on postoperative orthopedic patients. Grimby et al used three different kinds of training programs on 30 patients who had surgery for tears of the anterior cruciate or medial collateral ligaments, or both.82 Subjects were athletes with a mean age of 26 years (range of 16-46 years) who had been operated on approximately 14 months before the beginning of this study. All the subjects received postoperative physical therapy consisting of quadriceps femoris and hamstring muscle training once a week for two to three months, and the therapy was supplemented by a home program. At the time they began the training study, all had returned to athletic competition and could fully extend and flex their knees to at least 100 degrees without pain. Two of the three training groups performed what might be considered strength training exercises. One group trained isokinetically, extending the knee 10 times from a position of 100 degrees of flexion at a speed of 42°/sec. Three sets of 10 contractions were performed with a oneminute rest between contractions. This was done three days a week for six weeks. The second group used a quadriceps table where a weight was set so as to exert maximum resistance at 60 degrees from full extension. Subjects then exercised using the maximum weight that they could lift 10 times. This was repeated three times with a one-minute rest between bouts. This group also trained three days a week for six weeks. Both groups warmed up for five minutes on a bicycle ergometer before the training exercises. The isometric strength of the operated limb was approximately 80 to 90 percent of that of the nonoperated side before training. Both groups increased their strength when measured isometrically or isokinetically at speeds of 30 and 42°/sec, and the isokinetic group also improved at 120°/sec. However, it is interesting to note that when the increase in force values were examined, the isokinetic group improved 1784 more isometrically than did the other group but showed equal improvement isokinetically. Muscle biopsies taken before and after training showed no significant change in fiber areas despite the observed changes in the various strength measures. There was also no significant change in the concentrations of CP, ATP, lactate dehydrogenase, and myokinase. The results of this study demonstrate that in well-trained individuals, strength training may lead to increases in performance measures, such as force and torque, without changes being observed in the area or the metabolic profiles of muscle fibers. Methodological suggestions. The contrast is sharp between the systematic approach to endurance training and the multiple methods of examining strength training. Investigators examining the effects of endurance training almost always use a bicycle ergometer and examine effort or intensity in terms of V02 max. By using a common method and by sharing a commonly defined variable, studies may be related to each other and findings generalized. As was noted earlier, strength lacks a single definition and must be operationally defined. Perhaps systematization of future studies will be aided if the term "strength" is replaced by the term "power" which can be readily defined (Power=Work/time). Because this term is defined in classical physics, it can be measured and reliably used by others. Just as endurance studies report the level of effort in terms of V02 max, so might future studies on maximal efforts report their procedures in terms of the percentage of maximal power production a muscle may achieve. For power to be used as a replacement for strength in clinical settings, therapists will need to modify some of their methods of measurement. This modification appears to be both feasible and useful.92, 93 SUMMARY We have selectively examined the literature on muscle mutability in response to altered patterns of use. The body of literature is vast and is increasing everyday as new reports are published. We believe it is essential for physical therapists to meet the challenge of keeping current with this literature and of extrapolating clinically useful information. Throughout this article, we have attempted to review clinically relevant observations when we thought them appropriate. At times, we have engaged in conjecture, some of which undoubtedly will be refuted. Many points have been made in very general terms because the clinical application is unknown. For example, it was argued that under certain circumstances intensity or repetitions should be increased to cause a desired effect. However, knowing that physiologists increased the aerobic capacity of type II fibers in athletes by training them at greater than 90 PHYSICAL THERAPY percent of their Vo 2 max does not tell us what training level would be required for a sedentary middle-aged person or an elderly patient. The challenge that now faces physical therapists is to use the literature on muscle mutability to generate meaningful clinical hypotheses and to test them. These hypotheses could give rise to new treatment strategies that could be examined for efficacy through clinical investigations. Only through the testing of ideas on patients in a clinical setting can we define in clinical terms the types of procedures that will lead to desired changes in muscle. The research effort that will be needed before we can optimally apply the concepts of muscle biology to patient care may seem immense. However, we believe that the benefits of such an effort will make the cost worthwhile. The potential value of using muscle biology for patient care was first described by Engel, one of the pioneers in the field. He wrote: To learn the mechanism of type II fiber atrophy would be of general impor- tance—many patients with cancer and other chronic diseases appear to be more incapacitated by the generalized weakness of type II fiber atrophy than by any other aspect of their disease. If a method of reversing or preventing type II fiber atrophy could be found, many such patients could be greatly benefited even if their basic disease remained untreated.7(p113) The evidence reported in this review supports our contention that muscle is among the most mutable tissues in all of biology. It is also apparent that this mutability can have beneficial as well as negative effects on human functioning. Muscle appears to be dynamically changing from moment to moment in response to the patterns of use imposed upon it. It is likely that our success or failure with our patients will frequently depend on our ability to understand and use this dynamic capacity. REFERENCES 1. Edgerton VR: Mammalian muscle fiber types and their adaptability. American Zoology 18:113-125, 1978 2. Desmedt JE: Motor Unit Types, Recruitment and Plasticity in Health and Disease. Basel, Switzerland, S Karger AG, 1981 3. Pette D (ed): Plasticity of Muscle. Berlin, West Germany, Walter de Gruyter & Co, 1980 4. Salmons S, Henriksson J: The adaptive response of skeletal muscle to increased use. Muscle Nerve 4:94-105, 1981 5. Brooke MH: A Clinician's View of Neuromuscular Disease. Baltimore, MD, The Williams & Wilkins Co, 1977 6. Engel WK: The essentiality of histo and cytochemical studies of skeletal muscle in the investigation of neuromuscular disease. Neurology (NY) 12:778-784, 1962 7. Engel WK: Selective and nonselective susceptibility of muscle fiber types. Arch Neurol 22:97-117, 1970 8. Larsson L: Morphological and functional characteristics of the aging skeletal muscle in man. Acta Physiol Scand [Suppl] 457:1-36, 1978 9. Edgerton RV: Neuromuscular adaptation to power and endurance work. Can J Appl Sport Sci 1:49-58, 1976 10. Goldberg AL, Etlinger JD, Goldspink DF, et al: Mechanism of work-induced hypertrophy of skeletal muscle. Med Sci Sports Exerc 7:185-198, 1975 11. Sherrington CS: Ferrier Lecture: Some functional problems attaching to convergence. Proc R Soc Lond [Biol] 105:332-362, 1929 12. Burke RE: Motor Units in mammalian muscle. In Summer AJ (ed): The Physiology of Peripheral Nerve Disease. Philadelphia, PA, WB Saunders Co, 1980, p 133 13. Burke RE, Levine DN, Saleman M, et al: Motor units in cat soleus muscle: Physiological histochemical and morphological characteristics. J Physiol (Lond) 238:503-514, 1974 14. Burke RE, Levine DN, Tsairis P, et al: Physiological types and histochemical profiles in motor units of the cat gastrocnemius. J Physiol (Lond) 234:723-748, 1973 15. Burke RE, Levine DN, Zajac FE, et al: Mammalian motor units: Physiological-histochemical correlation in three types in cat gastrocnemius. Science 174:709-712, 1971 16. Burke RE, Tsairis P: The correlation of physiological properties with histochemical characteristics in single muscle units. Ann NY Acad Sci 228:145-159, 1974 Volume 62 / Number 12, December 1982 17. Kugelberg E, Edstrom L: Differential histochemical effects of muscle contractions on phosphorylase and glycogen in various types of fibers: Relation to fatigue. J Neurol Neurosurg Psychiatry 31:415-423, 1968 18. Kugelberg E: The motor unit: Morphology and function. In Desmedt JE (ed): Motor Unit Types Recruitment and Plasticity in Health and Disease. Basel, Switzerland, S Karger AG, 1981, p1 19. Nemeth P, Pette D: The limited correlation of myosin-based and metabolism-based classification of skeletal muscle fibers. J Histochem Cytochem 29:89-90, 1981 20. Nemeth P, Pette D, Vrobova G: Comparison of enzyme activities among single muscle fibers within defined motor units. J Physiol (Lond) 311:489-495, 1981 21. Johnson MA, Polgor J, Weightman D, et al: Data on the distribution of fibre types in thirty-six human muscles: An autopsy study. J Neurol Sci 18:111 -129, 1973 22. Peter JB, Barnard RJ, Edgerton VR, et al: Metabolic profiles of three fiber types of skeletal muscle in guinea pigs and rabbits. Biochemistry 11:2627-2633, 1972 23. Brooke MH, Kaiser KK: Muscle fiber types: How many and what kind? Arch Neurol 23:369-379, 1970 24. Buchtal F, Schmalbruch H: Motor unit of mammalian muscle. Physiol Rev 60:90-142, 1980 25. Ingjer F: Effects of endurance training on muscle fibre ATPase activity, capillary supply and mitochondrial content in man. J Physiol (Lond) 294:419-432, 1979 26. Saltin B, Henriksson J, Nygaard E, et al: Fiber types and metabolic potentials of skeletal muscles in sedentary man and endurance runners. Ann NY Acad Sci 301:3-29, 1977 27. Komi PV, Vitasalo JHT, Havu M, et al: Skeletal muscle fibres and muscle enzyme activities in monozygous and dizygous twins of both sexes. Acta Physiol Scand 100:385-392,1977 28. Gollnick PD, Hermansen L, Saltin B: The muscle biopsy: Still a research tool. The Physician and Sports Medicine 8:49-55, 1980 29. Goldspink G: Design of muscle for locomotion and the maintenance of posture. Trends in Neuroscience 4:218-221, 1981 1785 30. Costill DL, Daniels J, Evans W, et al: Skeletal muscle enzymes and fiber composition in male and female track athletes. J Appl Physiol 40:149-154, 1976 31. Costill DL, Fink WJ, Pollock NL: Muscle fiber composition and enzyme activities of elite distance runners. Med Sci Sports Exerc 11:12-15, 1979 32. Coyle EF, Bell S, Costill DL, et al: Skeletal fiber characteristics of world class shot-putters. The Research Quarterly 49:278-284, 1978 33. Green HJ, Thomson JA, Daub WD, et al: Fiber composition, fiber size and enzyme activities in vastus lateralis of elite athletes involved in high intensity exercise. Eur J Applied Physiol 41:109-117, 1979 34. Thorstensson A, Larsson L, Tesch P, et al: Muscle strength and fiber composition in athletes and sedentary men. Med Sci Sports Exerc 9:26-30, 1977 35. Karlsson J, Sjodin B, Tesch P, et al: The significance of muscle fibre composition to human performance capacity. Scand J Rehabil Med 56:62-65, 1978 36. Radin EL: Aetiology of osteoarthritis. Clin Rheum Dis 3:509-522, 1976 37. Hill AV: Production and absorption of work by muscle. Science 131:897-903, 1960 38. Sirca A, Susec-Michieli M: Selective type II fibre muscular atrophy in patients with osteoarthritis of the hip. J Neurol Sci 301:3-29, 1977 39. Janda V, Schmid HJA: Muscles as a pathogenic factor in back pain. In Buswell J, Gibson M (eds): International Federation of Orthopedic Manipulative Therapists: Proceedings of 4th Conference. New Zealand, Christchurch, 1980, p 1 40. Janda V: Muscle, central nervous motor regulation and back problems. In Korr IM (ed): The Neurobiologic Mechanisms in Manipulative Therapy. New York, NY, Plenum Publishing Corp, 1978, p 2 7 41. White AA III, Gordon SL: Synopsis: Workshop on idiopathic low-back pain. Spine 7:141-149, 1982 42. Jokl P: Muscles and low back pain. In White AA III, Gordon SL (eds): Symposium on Idiopathic Low Back Pain. St. Louis, MO, The CV Mosby Co, 1982, p 456 43. Guba F, Marechal G, Takacs O (eds): Mechanisms of Muscle Adaptation to Functional Requirements. Advances in Physiological Science, vol 24. New York, NY, Pergamon Press Inc. 1981 44. Booth FW, Seider MJ, Hugman GR: Effects of disuse by limb immobilization on different muscle fiber types. In Pette D (ed): Plasticity of Muscle. Berlin, West Germany, Walter de Gruyter & Co, 1980, p 373 45. Edgerton VR, Cremer S: Motor unit plasticity and possible mechanisms. In Desmedt JE (ed): Motor Unit Types, Recruitment and Plasticity in Health and Disease. Basel, Switzerland, S Karger AG, 1981, p 220 46. Vrbova G: Influence of activity on some characteristics of slow and fast muscles. In Hutton RS, Miller Dl (eds): Exercise and Sports Sciences. Philadelphia, PA, Franklin Institute Press, 1979, vol 7, p 181 47. Sakai Y, Kobayashi K, Iwata N: Effects of an anabolic steroid and vitamin B complex upon myopathy induced by corticosteroids. Eur J Pharmacol 52:353-359, 1978 48. Goldberg AL, Goodman HM: Relationship between cortisone and muscle work in determining muscle size. J Physiol (Lond) 200:667-675, 1969 49. Gardiner PF, Edgerton VR: Contractile responses of rat fasttwitch and slow-twitch muscles to glucocorticoid treatment. Muscle Nerve 2:274-281, 1979 50. Goldspink G, Ward PS: Changes in rodent muscle fibre types during postnatal growth, undernutrition and exercise. J Physiol (Lond) 296:453-469, 1979 51. Li JB, Goldberg AL: Effects of food deprivation on protein synthesis and degradation in rat skeletal muscles. Am J Physiol 231:441-448, 1976 52. Brooke MH, Kaplan H: Muscle pathology in rheumatoid arthritis, polymyalgia rheumatica and polymyositis. Arch Pathol Lab Med 94:101-117, 1972 53. Booth FW, Seider MJ: Early change in skeletal muscle protein synthesis after limb immobilization of rats. J Appl Physiol 47:974-977, 1979 1786 54. Fischbach GD, Robbins N: Changes in contractile properties of diseased soleus muscles. J Physiol (Lond) 201:305-320, 1969 55. Booth FW, Kelson JR: Effect of hind-limb immobilization on contractile and histochemical properties of skeletal muscle. Pflugers Arch 342:231-238, 1973 56. Maier A, Crockett JL, Simpson DR, et al: Properties of immobilized guinea pig hindlimb muscles. Am J Physiol 231:1520-1526, 1976 57. Sargeant AJ, Davies CTM, Edwards RHT, et al: Functional and structural changes after disuse of human muscle. Clinical Science and Molecular Medicine 52:337-342, 1977 58. Haggmark T, Jansson E, Erikson E: Fiber type, area metabolic potential of the thigh muscle in man after knee surgery and immobilization. International Journal of Sports Medicine 2:12-17, 1981 59. Gydikov A: Pattern of discharge of different types of alpha motor neurons and motor units during voluntary and reflex activities under normal physiological conditions. In Komi PV (ed): Biomechanics. Baltimore, MD, University Park Press, 1976, vol 5A, pp 45-65 60. MacDougall JD, Ward GR, Sale DG, et al: Biochemical adaptation of human skeletal muscle to heavy resistance training and immobilization. J Appl Physiol 43:700-703, 1977 61. MacDougall JD, Elder GCB, Sale DG, et al: Effect of strength training and immobilization on human muscle fibres. Eur J Appl Physiol 43:25-34, 1980 62. Edstrom L: Selective atrophy of red muscle fibres in the quadriceps in long-standing knee-joint dysfunction: Injuries to the anterior cruciate ligament. J Neurol Sci 11:551-558, 1970 63. Jozsa L, Balint JB, Demel S: Histochemical and ultrastructural study of human muscles after spontaneous rupture of the tendon. Acta Histochem (Jena) 63:61-73, 1978 64. Thorstensson A: Muscle strength, fibre types and enzyme activities in man. Acta Physiol Scand [Suppl] 443:1-45, 1976 65. Holloszy JO, Booth FW: Biochemical adaptations to endurance exercise in muscle. Annu Rev Physiol 38:273-291, 1976 66. Vihko V, Salminen A, Rantamaki J: Oxidative and lysosomal capacity in skeletal muscle of mice after endurance training of different intensities. Acta Physiol Scand 104:74-81,1978 67. Henriksson J, Reitman JS: Quantitative measures of enzyme activities in type I and type II muscle fibres of man after training. Acta Physiol Scand 97:392-397, 1976 68. Andersen P, Henriksson J: Training induced changes in the subgroups of human type II skeletal muscle fibres. Acta Physiol Scand 99:123-125, 1977 69. Jansson E, Sjodin B, Tesch P: Changes in muscle fibre type distribution in man after physical training: A sign of fibre type transformation? Acta Physiol Scand 104:235-237, 1978 70. Salmons S: The response of skeletal muscle to different patterns of use: Some new developments and concepts. In Pette D (ed): Plasticity of Muscle. Berlin, West Germany, Walter de Gruyter & Co, 1980, p 387 71. Sreter FA, Pinter K, Jolesz F, et al: Fast to slow transformation of fast muscles in response to long-term phasic stimulation. Exp Neurol 75:95-102, 1982 72. Jolesz F, Sreter FA, Mabuchi K, et al: Effect of various forms of hypo- and in-activity on slow muscle. In Guba F, Marechal G, Takas O (eds): Mechanism of Muscle Adaptation to Functional Requirements. Advances in Physiological Sciences, vol 24. New York, NY, Pergamon Press Inc. 1981, p 57 73. Lomo T, Westgaard RH, Engbretsen L: Different stimulation patterns affect contractile properties of denervated rat soleus muscles. In Pette D (ed): Plasticity of Muscle. Berlin, West Germany, Walter de Gruyter & Co, 1980, p 297 74. Munsat TL, McNeal D, Waters R: Effects of nerve stimulation on human muscle. Arch Neurol 33:608-617, 1976 75. Gollnick PD, Armstrong RB, Saltin B, et al: Effect of training on enzyme and fiber composition of human skeletal muscle. J Appl Physiol 34:107-111, 1973 76. Bergh V, Thorstensson A, Sjodin B, et al: Maximum oxygen uptake and muscle fiber types in trained and untrained humans. Med Sci Sports Exerc 10:151-154, 1978 PHYSICAL THERAPY 77. Suominen H, Heikkinen E, Lieson H, et al: Effect of 8 weeks' endurance training on skeletal muscle metabolism in 56-70year-old sedentary men. Eur J Applied Physiol 37:173-180, 1977 78. Gronnererod O, Dahl HA, Vaage O: Easy typing of human muscle fibers in sequentially preincubated myofibrillar ATPase section. Proceedings of the International Union of Physiological Science 13:285, 1977 79. Semans S: The Bobath concept in treatment of neurological disorders. Am J Phys Med 46:732-785, 1967 80. MacDougall JD, Sale DG, Moroz J, et al: Mitochondrial volume density in human skeletal muscle following heavy resistance training. Med Sci Sports Exerc 11:164-166, 1979 81. Nordemar R, Berg U, Ekblom B, et al: Changes in muscle fibre size and physical performance in patients with rheumatoid arthritis after 7 months physical training. Scand J Rheumatol 5:233-238, 1976 82. Grimby G, Gustafsson E, Peterson L, et al: Quadriceps function and training after knee ligament surgery. Med Sci Sports Exerc 12:70-75, 1980 83. Ringqvist M: Fibre size of human masseter muscle in relation to bite force. J Neurol Sci 19:297-305 84. Ringqvist I: Muscle strength in myasthenia gravis: Effect of exhaustion and anticholinesterase related to muscle fibre size. Acta Neurol Scand 47:619, 1971 Volume 62 / Number 12, December 1982 85. Costill DL, Coyle EF, Fink WF, et al: Adaptations in skeletal muscle following strength training. J Appl Physiol 46:96-97, 1979 86. Komi PV, Viitasalo JT, Rauramaa R, et al: Effect of isometric strength training on mechanical, electrical and metabolic aspects of muscle function. Eur J Applied Physiol 40:45-55, 1978 87. Thorstensson A, Hulten B, Von Dobeln W, et al: Effect of strength training on enzyme activities and fibre characteristics in human skeletal muscle. Acta Physiol Scand 96:392-398, 1976 88. Gonyea WJ, Erikson GC: Experimental model for study of exercise induced skeletal muscle hypertrophy. J Appl Physiol 40:630-633, 1976 89. Gonyea WJ, Bonde-Petersen F: Alterations in muscle contractile properties and fiber composition after weight-lifting exercise in cats. Exp Neurol 59:75-84, 1978 90. Gonyea WJ, Bonde-Petersen F: Electromyographic analysis of two wrist flexor muscles studied during weight lifting exercise in cats. Biomechanics 6A:207-212, 1978 91. Dubowitz V, Brooke MH: Muscle Biopsy: A Modern Approach. Philadelphia, PA, WB Saunders Co, 1973, pp 87-89 92. Rothstein JM, Delitto A, Sinacore D, et al: Electromyographic, peak torque, and power relationships during isokinetic movement. Phys Ther, to be published 93. Rothstein JM, Delitto A, Sinacore DR, et al: Muscle function in rheumatic disease patients treated with corticosteroids. Muscle Nerve, to be published 1787