Patient Care Worksheet: Nursing Assessment & Planning
advertisement

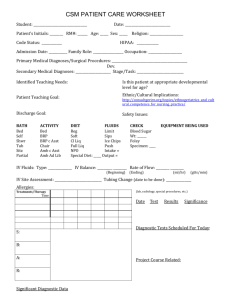
32 CSM PATIENT CARE WORKSHEET Student Date Patient Initials Rm # Admission Date Family type Primary Diagnoses/ Surgical Procedure Code Status Age Occupation Secondary Medical Diagnosis Religion HIPAA Is this patient at the appropriate developmental level for age? Dev. Stage/Task Identified teaching needs of patient/caregiver: Patient/ Caregiver Teaching Goal: (Based on teaching needs) Ethnic/Cultural Implications: Safety Issues: (Based on developmental level): BATH Bed Self Shower Tub Partial Assist ACTIVITY Bed BRP BRP c Asst Chair Amb c Asst Amb ad Lib Discharge Plan: DIET FLUIDS Reg Soft/Pureed Cl Liq Full Liq NPO Special diet: Limit Blood sugar: Sips Wt: Ice Chips Foley: Push Specimen: Intake for my Output for my shift: shift: Total Care Restraints IV Fluids: type NG/Gastrostomy Fluids: Type Allergy Treatments/ Therapy Diagnostic Test Sched for today CHECK/LIST Flow rate Flow rate/Bolus/ H2O Feed Amount Time Normal Vitals for age Temp: BP: Pulse: Resp: O2 saturation Pain level Other EQUIPMENT BEING USED Site Assessment Residual Special VS parameters for Patient Temp: BP Pulse Resp O2 saturation ASSESSMENTS/OBSERVATIONS Day 1 Day 2 ASSESSMENT CRITERIA INTEG: color, temp, moisture, turgor, integrity, scars, incisions, lesions (measure) NEURO: A&O x 4, PERRLA, DTR'S, symmetry, facial expressions, EOMs x 6, fine/gross motor fxn, MAE, grips, sensation, speech, strength, Babinski *RESP: rate, rhythm, depth, effort, breath sounds, cough, O2 sat., symmetry of chest, m. membranes color *CV: pulses, capillary refill, edema, CSM, cyanosis, murmur T= T= R= R= B/P= Apical P= Radial P= B/P= Apical P= Radial P= *GU: urine amount & characteristics, bladder distention, ext. genitalia condition, circumcised GI: intake %, appetite, BM, bowel sounds, distention, masses *MS: ROM, spine, MAE, Strength, paralysis, ambulation status EENT: vision, glasses, ENT discharge, hearing, hearing aid, dentures, nares, lymphadenopathy EMOT/PSYCH: affect, mood, cooperation, family support systems PAIN: location, intensity, characteristics, pharmacological and nonpharmacological interventions & effectiveness *Include any accessory equipment used on patient (monitor, 02, foley, NG or gastrostomy tube) TIME MANAGEMENT PLAN Primary Patient Goal: TIME PLAN Met/Not Met ANALYSIS OF DAY How did it go/What could I change? PATIENT CARE PLAN DATA Subjective & Objective NURSING DIAGNOSIS PATIENT GOAL OUTCOME CRITERIA NURSING INTERVENTIONS RATIONALE WITH REFERENCES EVALUATION