Samir Mohamed Zahed Abd-Allah_pemberton acetabuloplasty
advertisement

Pemberton Acetabuloplasty for Residual
Developmental Acetabular Dysplasia
Sameer Zahed MD, Alhusseiny Moustafa MD,
Abd-albary Gouda MD,
Banha Faculty of Medicine, Banha University, Egypt
Abstract
The objective of this work is to study the effect of Pemberton lateral
acetabular osteotomy on acetabular development. The osteotomy was
done for fifty- nine hips in 48 (11 bilateral and 37 unilateral)
patients. The average age at the time of surgery was 1.9 years. The
osteotomy was preceded by closed reduction in 18 hips, open
reduction with varus derotation femoral osteotomy in 32 hips, and no
treatment in 9 hips. The radiologic outcome according to the criteria
of Severin was the corner stone in assessment of the results. At the
final follow up period (average 4 years) for all the cases (59), there
were: 46 hips with Severin class I (excellent), 10 hips with Severin
class II (good), and 3 hips with Severin class III (fair). The final
follow up values of acetabular index and centre edge angle were
nearly the same for the normal and the operated abnormal hips in
the unilateral cases. There was limited range of motion in one case
but did not affect the daily activities. Our conclusion is that
1
Pemberton acetabuloplsty can positively affect the growth and
maturation of the acetabulum with residual developmental dysplasia.
Introduction
Patients who have developmental hip dislocation have laxity of the joint
capsule associated with acetabular dysplasia, subluxation, or dislocation
of the hip, and, on occasion, an angular or rotational deformity of the
proximal aspect of the femur. The major goal of treatment is to restore the
hip to an anatomical configuration that is near to normal as possible {1}.
However, the various methods by which this goal is accomplished have
been subject to considerable controversy. There is disagreement as to
whether the proximal aspect of the femur or the acetabulum should be
selected as the site for correction
{2}.
Many authors
{3, 4, 5, 6}
have
proposed that osteotomy of the pelvis represents a more direct approach
to acetabular dysplasia. Conversely, there are several proponents of
proximal femoral osteotomy {7, 8, 9, 10}. They believe that alteration of the
neck shaft angle at the proximal aspect of the femur can lead to correction
of the acetabular deficiencies.
Osteotomy of the innominate bone, an operation devised by Salter
{10},
is
useful only when any subluxation or dislocation has been reduced or can
be reduced by open reduction at the time of osteotomy in a child 18
months to 6 years of age. The entire acetabulum together with the pubis
2
and ischium is rotated as a unit, the symphesis pubis acting as a hinge.
The osteotomy is held open antrolaterally by a wedge of bone, and thus
the roof of the acetabulum is shifted more anteriorly and laterally.
The term acetabuloplasty designates operations that redirect the
inclination of the acetabular roof by an osteotomy of the ilium superior to
the acetabulum followed by levering of the roof inferiorly. Pemberton
{5)
devised an acetabuloplasty that he called pericapsular osteotomy of the
ilium in which an osteotomy is made through the full thickness of the
ilium, using the triradiate cartilage as the hinge about which the
acetabular roof is rotated anteriorly and laterally. Pemberton osteotomy is
useful only (as in Salter osteotomy) when any subluxation or dislocation
has been reduced or can be reduced by open reduction at the time of the
operation in children at least 18 months old
{11}.
Historically {12}, the first
authors to osteotomies the lateral side were Albee (1915), Jones (1920) in
USA. Lance (1925) introduced the technique in Paris to be followed by
other European surgeons. Some of them osteotomised deeper toward the
triradiate cartilage (Wiberg 1953; Mittelmeier1964; Dega 1965).
Pemberton lateral acetabuloplasty did not gain the same popularity as
Salter innominate osteotomy. Also, there are no much reports
investigating the effect of this osteotomy on the acetabular development.
Objectives; this study aim to present the authors experience after 59
lateral acetabloplasty osteotomies of Pemberton type, for correction of
3
residual acetabular dysplasia in patients of congenital hip dislocation. The
aim is to study the effect of Pemberton osteotomy on the acetabular
growth and hip development.
Patients and Methods
During the period between February 1997 and July 2002, 59 lateral
acetabuloplsty osteotomy had been performed for 48 patients with
developmental hip dysplasia as a treatment for residual acetabular
dysplasia. Forty three surgeries (35 patients) were done in Saudi German
Hospital, Jedda and sixteen surgeries (13 patients) were done at Banha
University Hospital. The age of the patients included in this study ranged
from one to three years, (average 1.9 years). Operative therapy is
generally not indicated in patients who are less than one year old, since
non operative methods are usually successful.
There were 11 bilateral hip dislocations, 22 right and 15 left. There were
34 girls and 14 boys. Previous open reduction and derotation femoral
osteotomy was done in 32 hips, closed reduction and hip spica was used
before in 18 hips, and no interventions previous to the osteotomy in 9
hips. The indications for the osteotomy in this study were residual
acetabular dysplasia or progressive subluxation of the femoral head, as
documented by serial pelvic radiographs. The prerequisites for the
osteotomy (inclusion criteria) were : (1) Concentric reduction of the
femoral head in the acetabulum as demonstrated by antroposterior
4
radiographs with the hip abducted flexed and internally rotated; (2) Age
one year or more; (3) No major deformities of the femoral head or the
acetabulum; (4) Satisfactory hip range of motion. The duration of follow
up ranged from 3 to 8 years (Average 4 years). The patients were
evaluated clinically and radiologically every three months in the first two
years after surgery and then yearly later on. The patients were assessed
clinically regarding the range of motion of the hip joint, limping and pain.
The hip joints were radiographed to assess the acetabular index, quality of
reduction and the occurrence of avascular necrosis of the femoral head.
Clinical assessment, on the final evaluation, was scored according to
McKay
{13}
criteria as follows: Excellent; painless, stable hip with no
limping and negative Trendelenburg sign. The hip internal rotation is
more than 15 degrees and otherwise normal range of motion. Good;
painless stable hip with slight limp, decreased motion and negative
Trendelenburg sign. Fair; minimal pain with positive Trendelenburg sign
and moderate stiffness of the hip joint. Poor; significant pain and
limping.
Radiologic classification of Severin
{14}
was adopted to assess the final
radiologic results (Table 1). This anatomical classification is currently
considered the best method for radiographic assessment of congenitally
dislocated hip. It incorporates the evaluation of the centre edge angle,
concentricity, and congruity of the hip joint.
5
Femoral head necrosis; The presence or absence of femoral head
necrosis was determined with the use of criteria of Kalamaci and
MacEwin {4}, (Table 2).
Operative Technique
- Under general anaesthesia with the patient supine on a radiolucent table,
the hip joint is exposed through bikini incision.
- The lateral side of the iliac bone is completely exposed down to the joint
capsule and posteriorly to the sciatic notch. Next, two flat retractors are
inserted subperiosteally into the sciatic notch, one along the medial
surface of the ilium to protect the important structures over iliacus
muscle, and one along the lateral surface to keep the anterior third of the
ilium exposed both medially and laterally.
- The acetabular roof is transected 6- 8 mm above the lateral acetabular
margin using a flat 1- 2 cm osteotome driven forward and medially, under
image intensifier control, towards the posterior rim of the triradiate
cartilage. Anteriorly, the osteotome passes above or through the anterior
inferior iliac spine and must be withdrawn and placed more posteriorly
where the pelvic wing is thicker. On the medial side, the cut should
terminate a short distance above the triradiate cartilage, without entering
it; thus placing the hinge parallel to the posterior triradiate cartilage.
6
- Before levering the acetabular roof downwards to attain a normal angle,
the osteotomy must be completed posteriorly by driving the osteotome in
ilioischial rim of the triradiate cartilage just anterior to the sciatic notch.
An osteotome of 2 cm width is ideal for this manoeuvre since it applies
even pressure over the whole acetabular roof
- The acetabular roof is kept in its corrected position by a bone wedge
placed in the posterior side of the osteotomy. The graft might be fixed by
one or 2 K wires.
- Capsuloraphy is done to augment the soft tissue over the reduced head.
- Bilateral hip spica is applied for 10- 12 weeks.
Results
No patient had discomfort or pain with activity at the time of the most
recent follow-up examination. The motion in three hips was limited to 90
degrees of flexion and 20 degrees of inward rotation. This clinical
limitation did not affect the activities of daily living. The range of motion
of the remaining 56 hips was normal. A residual positive Trendelenburg
gait of the fatigue type was found in one hip while the other 58 hips had a
normal gait.
The degree of acetabular coverage achieved by the growth and
development of the abnormal (treated hips) was compared with that of the
normal (untreated hip) with the use of the previously described Severin
7
radiographic criteria. Thirty seven patients had a unilateral Pemberton
osteotomy (right; 22 and left; 15). Radiographs were made for both the
abnormal (treated) and the normal (untreated) hips throughout the entire
duration of follow-up averaging 4 years (3- 8 years). Thus, it was possible
to assess the effect of the lateral acetabuloplasty osteotomy of Pemberton
on acetabular growth and development of the abnormal hips (Table 3).
The preoperative acetabular index in the 37 normal hips averaged 19
degrees, compared with 33 degrees in the abnormal hips. At the most
recent follow-up examination, the acetabular index average was
12degrees in the normal hips with an open triradiate cartilage, and it had
improved to an average of 11 degrees in the abnormal hips.
Preoperatively, the average centre-edge angle of Wiberg {15} was 27
degrees in normal hips and 3 degrees in abnormal hips. In contrast, the
centre-edge angle averaged 35 degrees for both the normal and the
abnormal hips at the most recent follow-up examination (Table 3).
Acetabular angle of Sharp {16}, which was measured in patients who had
a closed triradiate cartilage at the most recent follow-up visit, averaged 42
degrees in normal hips and 40 degrees in abnormal hips (Table 3).
At the most recent overall follow-up examination of the 59 operated hips:
forty-two hips were rated as class (Ia) (normally developed hip)
according to Severin criteria {14} (Table 4) (Figure 1). Six hips were
rated as class (IIa), with some deformity as a result of abnormal osseous
8
development (Figure 2), while the centre-edge angle of Wiberg was
within the normal range. Eight hips had a marginal centre-edge angle that
caused four to be classified as (Ib) (Figure 3) and another four as (IIb).
Only three hips were rated as class III (a dysplastic hip with no
demonstrable evidence of instability). This was considered to be a
marginal result. Thus, 56 out of 59 of the treated hips were rated as class I
or II (excellent or good) at the most recent follow-up examination; only
three hips were rated as class III (fair).
Complications: Preoperatively, ten hips had evidence of avascular
necrosis of the femoral head (Kalamaci and MacEwin {4}, grade 1). The
necrosis was in the fragmentation phase at the time of the osteotomy. All
had had a previous closed or open reduction. At the most recent followup examination, only two of those ten patients had a Severin rating of
class I. One had a rating of class (IIa); four, class (IIb); and three, class
III. Avascular necrosis of the femoral head did not develop in any patient
after the Pemberton acetabuloplasty osteotomy. No patient had necrosis
of the acetabulum. We identified no radiographic evidence of
chondrolysis, premature arrest of the triradiate cartilage, or iatrogenic
femoral head-acetabular incongruity as a result of the osteotomy. There
were no postoperative infections.
9
Discussion
It has been agreed that correction of acetabular deficiency should be the
primary goal in the treatment of residual acetabular dysplasia in patients
who have congenital dislocation of the hip. We have observed, along with
others {3, 4, 5, and 6}, that this is achieved most directly by pelvic osteotomy.
In order to explore the validity of this concept, we reviewed the results of
Pemberton pericapsular osteotomy in fifty-nine hips in forty-eight
patients who had acetabular dysplasia. The osteotomy was done by first
two of us in Benha University Hospital, Egypt and Saudi German
Hospital, Jeddah, Saudi Arabia over a period of 7 years. Both surgeons
followed the same technique prescribed before.
Eyre- Brook et al.
{17},
reviewed the results of Pemberton osteotomy in
thirty-seven patients, but only the centre-edge angle was measured; the
acetabular index and the angle of Sharp were not recorded. Five of their
thirty-seven patients had closed triradiate cartilage at the time of the
osteotomy, and eleven of the patients had a femoral osteotomy at the time
of, or shortly after, the acetabular osteotomy. In addition, in eleven of
their patients, the acetabuloplasty had been done after previous acetabular
or femoral procedures. This multiplicity of variables made it difficult to
reach conclusions regarding the real influence of the Pemberton
osteotomy on acetabular development. We attempted to eliminate all of
10
these variables. Patients who had a previous procedure other than an open
or closed reduction were excluded.
The radiographic appearance of the hip joint has been recognized as the
best prognostic factor for longevity of the hip joint in patients who have
congenital dislocation of the hip
{18}.
In the present study, acetabular
development was documented by qualitative and quantitative criteria as
well as by the criteria of Severin
{14}.
With the use of these parameters,
comparison of the normal and dysplastic hips permitted an assessment of
the growth and maturation of the hip that had been treated with a
Pemberton osteotomy compared with the normal, untreated hip. The
centre-edge angle of Wiberg
{15}
is considered to have some value in the
prediction of the function of the hip joint in adulthood. According to
Wiberg, this measurement reflects either the adequacy of acetabular
development or any subluxation of the femoral head, or both. The clearly
established improvement in the centre-edge angle at the time of follow-up
in the hips that were treated with Pemberton osteotomy demonstrates that
the osteotomy consistently improved coverage of the femoral head.
Over many years, Severin
{14}
criteria have been used for analysis of the
end-results of various treatment modalities for congenital dislocation of
the hip. Ward {19} and his associates reported poor levels of interobserver
and intraobserver reliability when the system was used. Despite this, we
found that Severin criteria are the most realistic available system to use in
11
this study. Severin primarily restricted his classification to patients who
were six years old or more only because too few of his patients were
younger than the age of six for him to make a statistically valid statement
about the usefulness of his system in this age group. Severin, however,
found that the centre-edge angles in normal children who were younger
than the age of six years corresponded to the same values as those found
in children who were six to thirteen years old. To test the hypothesis that
the classification of Severin could be used in patients who were younger
than the age of six, we classified the normal hips in our series with his
system. We found that the classification could be reliably extended to
younger patients, who had the same distribution of marginal values as
would be expected with the use of the values that Severin gave for
patients who were six to thirteen years old.
In our study, at the follow-up examination, fifty-one of the operatively
treated hips were rated as either class I (forty-four hips) or class II (seven
hips), with the radiographic results rated as excellent or good,
respectively. These results are evidence of the effectiveness of the
Pemberton osteotomy on acetabular development.
Pre-existing necrosis of the femoral head (10 hips) infection makes the
prognosis for hips treated with a pericapsular osteotomy much less
predictable. The necrosis that was seen in the present study was identical
to that which occurs in patients in whom avascular changes in the capital
12
femoral epiphysis develop after a closed reduction with excessive
abduction force, and while the patient is wearing a spica cast or a Pavlik
harness, for treatment of congenital dislocation of the hip
{20, 21, 22, 23}.
As
children, these patients rarely have pain, and very few have a limited
range of motion. Similarly, the prognosis, in terms of normal
development of the femoral head, after a Pemberton osteotomy is not as
good as in children who have no necrosis of the femoral head.
Seven of the ten hips that had good (four) or fair (three) radiographic
results in the present series had had necrosis of the femoral head before
the osteotomy. Only two of the ten hips in which necrosis of the femoral
head had been identified preoperatively had a rating of class (Ia) at the
latest follow-up examination. Arthrograms of the hip were not used in
this series, as we think that the concentricity of reduction of the hip can
be interpreted accurately by careful study of radiographs made with the
hip in abduction and internal rotation.
In conclusion, we think that Pemberton osteotomy is a safe, effective
procedure for correction of residual acetabular dysplasia in patients who
have congenital dislocation of the hip.
References
1- Tavaro J: Modified Pemberton acetabuloplasty for the treatment of
congenital hip dysplasia. J Pediatr Orthop. 24 (5):501- 7, 2004
13
2- Milickovice Z: Acetabular development after operative treatment of
residual acetabular dysplasia: a comparative study between different
age groups. J Bone and Joint Surg 85-A(2):278-86, 2003
3- Hall J E: Pelvic osteotomy in the early treatment of CDH. Advances
Orthop Surg, 10: 3, 1986.
4- Kalamchi Ali; and MacEwen G: Avascular necrosis following
treatment of congenital dislocation of the hip. J. Bone and Joint
Surg, 62-A: 876-888, Sept. 1980.
5- Pemberton P: Pericapsular osteotomy of the ilium for treatment of
congenital subluxation and dislocation of the hip. J. Bone and Joint
Surg, 47-A: 65-86, 1965.
6- Salter R: Innominate osteotomy in the treatment of congenital
dislocation and subluxation of the hip. J. Bone and Joint Surg, 43-B
(3): 518-539, 1961.
7- Harris N; Lloyd-Roberts G; and Gallien R: Acetabular development
in congenital dislocation of the hip. With special reference to the
indications for acetabuloplasty and pelvic or femoral realignment
osteotomy. J. Bone and Joint Surg., 57-B (1): 46-52, 1975.
8- Kasser J; Bowen J; and MacEwen, G: Varus derotation osteotomy
in the treatment of persistent dysplasia in congenital dislocation of
the hip. J. Bone and Joint Surg, 67-A: 195-202, Feb. 1985.
14
9- Lloyd-Roberts G: The role of femoral osteotomy in treatment of
congenital dislocation of the hip. In congenital dislocation of hip, p
427-435. Edited by Tachdjian M O. New York, Churchill
Livingstone, 1982.
10- Somerville E: A long-term follow-up of congenital dislocation of the
hip. J. Bone and Joint Surg, 60-B (1): 25-30, 1978.
11- Ponseti, I: Growth and development of the acetabulum in the normal
child. J. Bone and Joint Surg., 60-A: 575-585, July 1978.
12- Cherney D; and Westin G: Acetabular development in congenitally
dislocated hips as a function of age at the time of reduction. Orthop.
Trans., 6: 377-378, 1982.
13- McKay D: A comparison of the innominate and the pericapsular
osteotomy in the treatment of congenital dislocation of the hip. Clin
Orthop, 98: 124-132, 1984.
14- Severin Erik: Congenital dislocation of the hip. Development of the
joint after closed reduction. J Bone and Joint Surg, 32-A: 507-518,
1950.
15- Wiberg Gunnar: Studies on dysplastic acetabula and congenital
subluxation of the hip joint. With special reference to the
complications
of
osteoarthritis.
Acta
Chir.
Scandinavica,
Supplementum 58, 1939.
15
16- Sharp I: Acetabular dysplasia. The acetabular angle. J. Bone and
Joint Surg., 43-B (2): 268-272, 1961.
17- Eyre-Brook A; Jones D ; and Harris F: Pemberton's
acetabuloplasty for congenital dislocation or subluxation of the hip. J
Bone and Joint Surg, 60-B(1): 18-24, 1978.
18- Smith W; Badgley C; Orwig J; and Harper J: Correlation of post
reduction
roentgenograms
and
thirty-one-year
follow-up
in
congenital dislocation of the hip. J. Bone and Joint Surg, 50-A:
1081-1098, Sept. 1968.
19- Ward W, Voght M, Grudziak J, et al: Severin classification system
for evaluation of the results of operative treatment of congenital
dislocation of the hip. J Bone and Joint Surg 1997; 79–A:656- 63
20- CoopermanD; Wallensten R; and Stulberg S: Post-reduction
vascular necrosis in congenital dislocation of the hip. Long-term
follow-up study of twenty-five patients. J. Bone and Joint Surg, 62A: 247-258, March 1980.
21- Gage J ; and Winter R : Avascular necrosis of the capital femoral
epiphysis as a complication of closed reduction of congenital hip
dislocation. A critical review of twenty years' experience at Gillette
Children's Hospital. J. Bone and Joint Surg., 54-A: 373-388, 1972.
16
22- Thomas C; Gage J; and Ogden J: Treatment concepts for proximal
femoral ischemic necrosis complicating congenital hip disease. J.
Bone and Joint Surg, 64-A: 817-828, July 1982.
23- Tonnis D (editor): Congenital Hip Dislocation—Avascular Necrosis,
translated by Gottfried Stiasny. New York Thieme- tratton, 1982.
17
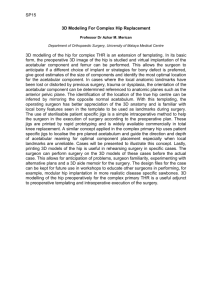
Figure (1): (A) Open reduction and Pemberton osteotomy were done for
non touched neglected left DDH for this male patient at the age of 25
months. (B&C) Antro-posterior and lateral follow up radiographs at the
age of 7 years with excellent outcome (grade Ia Severin).
Figure (2): (A), Male patient with left DDH. (B), varus derotation
osteotomy (complicated by avascular necrosis, grade I) was done at age
25 months followed 5 months later by Pemberton osteotomy. (C), follow
up at 38 months age. (D), the final follow up at age of 4 years and 5
months showed centre edge angle >19 deg. with mild deformity of the
femoral neck (Severin grade IIa, good).
Figure (3): (A) 13 month old female with neglected left DDH. (B)
Pemberton acetabuloplasty was done at age of 19 month following healed
varus derotation osteotomy. (C) Final follow up at age of 6 years.
Acetabular index was restored, centre edge angle 15 deg.- 19 deg.
denoting grade Ib Severin (excellent).
18
Table (1): Severin {14} classification system for hip dysplasia.
Table (2): Kalamaci and MacEwin classification system {4}.
Table (3): Average radiographic measurements (in degrees) for the
normal (untreated hips) and abnormal (treated hips) in 37 unilateral
cases.
Table (4): Radiologic outcome at the last follow up
19
Figure (1):
(1- A)
(1- B)
(1- C)
20
Figure (2):
(2- A)
(2- C)
(2- B)
(2- D)
21
Figure (3):
(3- A)
(3- B)
(3- C)
22
Table (1):
Class & Grad
Centre edge angle (degrees)
Radiographic Appearance
Ia, Excellent
> 19 deg. (6-13 yrs old)
Normal
> 25 deg. (14 yrs or more)
Ib
15-19 deg. (6-13 yrs old)
20- 25 deg. (14 yrs or more)
IIa, IIb Good
III, Fair
Same as class I
<15 deg. (6-13 yrs old)
Normal
Moderate deformity of femoral head,
femoral neck, or acetabulum
Dysplasia without subluxation
< 20 deg. (14 yrs or more)
IVa, Poor
IVb
V, Failure
VI, Failure
0 deg. or more
< 0 deg.
Moderate subluxation
Severe subluxation
Negative
Femoral head articulates with
pseudoacetabulum in superior part of
original acetabulum
Negative
Redislocation
Table (2):
1- Delay in the appearance of ossific nucleus or mottling of the cartilage
model with little effect on the neck, minimal loss of height of the
ossific nucleus, occasional coxa magna.
2- Changes in the ossific nucleus plus lateral physeal damage.
3- Changes in the ossific nucleus plus central physeal damage
4- Total damage to the head and physis.
23
Table (3):
Acetabular Index
Hip
Preop. Follow up
Centre edge angle
Preop. Follow-up
Angle of Sharp
Follow up
Normal
19
12
27
35
42
Abnormal
33
11
3
35
40
Table (4):
Grade
Ia
Excellent
No of patients
42
Ib
4
IIa Good
6
IIb
4
III Fair
3
IV, V, VI; poor to failure
0
24