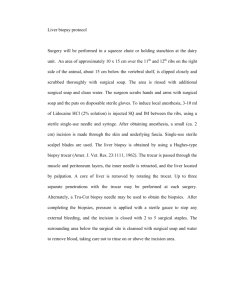
Here
advertisement

Surgical Techniques For 3rd year medical students Institute of Surgical Research University of Szeged, Medical Schoool Hungary 2005 1 1. Asepsis and antisepsis 1.1. Historical overview 19th century surgery has faced with four „classic” difficulties. Pain, infection, obsolete technology and the enigmatic pathophysiological changes of the perioperative period were the greatest obstacles. By the end of the „century of surgeons” three problems were solved, and modern clinical surgery was born. The first milestone was reached on October 16, 1846 in the Massachusetts General Hospital, when a patient of John Collins Warren (1778–1856) was successfully narcotized by ether by William T. G. Morton (1819-1868) a dentist from Boston. Within some weeks, on December 21, 1846, Robert Liston (1794–1847) applied ether narcosis in London. Hungary kept in line with the developments. Lajos Markusovszky (18151893) tested the ether narcosis in Vienna on January 25, 1847, and then he performed an operation on February 8, 1847 together with János Balassa in Budapest. Narcosis has quickly become a relatively safe and generally accepted method in surgery. Vilmos Vajna reported on the 3-years statistics of the German Surgical Society in the Hungarian Medical Weekly Journal in 1893 (the foundation of the journal (1857) and the Hungarian Medical Publishing Company (1863) was also the merit of Markusovszky); 3098 cases were anesthetized with only one death. A new era commenced; hence the duration of the operation was not delimited by pain. Initial attempts to prevent wound infection were not that successful. Surgical incisions were still followed by irritative fever, which sometimes lasted only for few days and accompanied by pus bonum et laudabile (good and commendable pus, sec. Galen) but even the most brilliant surgeons had to take into account the possibility of fatal postoperative infection. The terms „hospitalism” and „hospital gangrene” were used to denominate postoperative infections. The frequency of these infections is well-demonstrated by the incidence of the puerperal fever. The average death rate was 9.92% in the Department of Obstetrics at the Allgemeines Krankenhaus in Vienna, but in certain periods the incidence was as high as 29.3% (October 1842). In this period the average mortality rate in hospitals in Edinburgh and Glasgow averaged around 40%, and was as high as 59% in Paris. According to James Simpson (the British obstetrician who introduced chloroform narcosis) „a man laid on an operating table in one of our surgical hospitals is exposed to more chances at death than was an English soldier on the battlefield of Waterloo.” Finally Ignác Semmelweis (1818–1865) identified unequivocally that decomposing organic matter on the surgeon’s hands propagates infection leading to the spreading of puerperal fever, e.g. sepsis. On May 15, 1847, Semmelweis introduced compulsory hand wash with chlorinated lime and succeeded to reduce the mortality rate from puerperal fever from 14.5% to 1.2% in his department. Before the era of the bacteriology this was a strike of genius. Semmelweis has proved the effectiveness of the asepsis but the adverse circumstances prevented the rapid spread of his theory and this recognition did not become generally known. At the beginning of the 1860’s Louis Pasteur (1822-1895) elaborated the „germ theory”. Twenty years after Semmelweis Sir Joseph Lister (1827–1912) Scotch surgeon elaborated the method of wound disinfection. Lister sprayed carbolic acid (fenol) in the operating theater to the instruments, to the hand of the surgeon and also onto the wound to kill microorganisms, thereby laying the foundation of ”antisepsis” (1867). Robert Koch (1843–1910) reported his postulates in 1881 by which it become possible to verify that infectious diseases are caused by living microorganisms, namely bacteria: 1. “After it has been determined that the pathogenic organism is present in the animal body, 2. and after it has been shown that the organism can reproduce in the body; 3. and be transmitted from one individual to another, the most important experiment remains to be done.... 2 4. to determine the conditions necessary for growth and reproduction of the microorganism.” In a further substantial step Ernst von Bergmann (1836-1907) introduced the sublimateantisepsis (1887) and the steam-sterilization (1886), then Curt Schimmelbusch (1850-1895) the aseptic wound management. At the end of the 1880’s Lister realized that the treatment of wounds with antiseptics has a disadvantageous effect on wound healing. Furthermore it has been shown that the effect of chemicals is only superficial, they are not able to kill bacteria in deep tissues. Later Lister admitted that the aseptic method elaborated by the German school of surgeons is more advantageous than his own. Surgical gloves were invented by William S. Halsted, chief surgeon of the Johns Hopkins University (1852–1922). In 1890 Halsted requested the Goodyear Rubber Company to prepare thin rubber gloves for the head scrub nurse (his later wife), Caroline Hampton, who suffered from dermatitis caused by the disinfectants. J. Bloodgood the follower of Halsted used these gloves routinely, and the method decreased not only the incidence of dermatitis but the number of postoperative wound infections as well. Today, asepsis is a generally acknowledged principle of modern surgery. However, serious sepsis is still a life threatening systemic condition. 1.2. Asepsis and antisepsis in the surgical practice During surgery the body’s major defense against infection, the skin is broken and the inner surfaces of the body are exposed to the environment. Therefore, every attempt must be made to prevent bacteria from entering the wound (asepsis) and to eliminate them if they have already entered (antisepsis). Definition of asepsis Procedures to reduce the risk of bacterial (or other, e.g. fungal, viral) contamination. It involves the use of sterile instruments and gloved „no touch” technique. It includes all of those prophylactic methods, working processes and behavioral forms by which microorganisms (bacteria, fungi and viruses) can be kept off the patient’ organism and the surgical wound. The goal of the asepis is to prevent contamination. The asepsis can be secured by the use of sterile devices, materials and instruments and by creating an environment that is poor in microbes. Definition of antisepsis Removal of transient microorganisms from the skin and a reduction in the resident flora. It terms those techniques which are applied to eliminate contamination (bacterial, viral, fungal and others) to be present in the objects and skin by sterilization and disinfection. Living surfaces, the skin, the operating field and the surgeon’s hand can not be considered sterile. In wider sense asepsis concern an ideal state when the instruments, skin and the surgical wound is free from pathogenic germs – antisepsis includes all prophylactic procedures which are to secure surgical asepsis. Asepsis is what is primarily important. Asepsis = prevention! Definition of sterility It is a microbiologically germfree state of the materials and items. This means that they are free from every kind of pathogenic and apathogenic microorganisms including latent and resting forms, such as spores. 3 1.3. Surgical infections Possible sources of pathogens: 1. endogenous flora of the patient; 2. operating theater environment; 3. hospital personnel. 1.3.1. The main cause of postoperative wound infections is the endogenous flora Skin: Staphylococci, Streptococci Mouth: Staphylococci, Streptococci, anaerobes Nasopharynx: Staphylococci, Streptococci, Haemophilus, anaerobes Large bowel: Gram-negative rods, Enterococci, anaerobes Urinary tract: normally sterile. 1.3.2. Main pathogens of the surgical wound contaminations Staphylococcus aureus (20%), Coagulase-negative staphylococcus (14%), Enterococcus (12%), Escherichia coli (8%) Pseudomonas aeruginosa (8%), Enterobacter (7%), Proteus mirabilis, Klebsiella pneumoniae, Candida albicans, Bacteroides fragilis, other streptococci (2-3%). (Source: National Nosocomial Infections Surveillance (NNIS) System, Centers for Disease Control and Prevention (CDC), 1996) 1.3.3. Main sources of the wound contaminations Direct inoculation Patient’s residual flora or skin contamination Surgeon's hands Contaminated instruments or dressings Contaminated procedure Drains, catheters or intravenous lines Airborne contamination Skin and clothing of staff and patients 4 Air flow in operating theatre or ward Haematogenous spread Intravenous lines Sepsis at other anatomical sites (Source: Leaper DJ. Risk factors for surgical infection. J Hosp Infect 1999; 30 S127-139) 1.3.4. Surgical site infection (SSI) SSI is the most common nosocomial infection in surgical patients (approx. 40%). Serious complication with 1-3% overall incidence (but the incidence ~10% following colon surgery), and increases hospital duration 5-15 days. SSI develops within two hours after the contamination. Oxidative processes play an important role in the defense against microorganisms: reactive oxygen species (primarily the superoxide anion) represent the first line of defense against surgical pathogens. As the NADPH-oxygenase of the leukocyte is pO2–dependent (Km~60 mmHg), in case of hypoxia the chance of destroying bacteria is diminished. 1.3.5. Types of surgical wound contaminations Superficial incisional SSI. Criteria for defining an SSI as superficial: 1. Infection occurs 30 days after operation. 2. The infection involves only skin and subcutaneous tissue of incision, and 3. At least one of the following is present: - Purulent discharge from surgical site, - At least 1 of the signs and symptoms of infection (pain, tenderness, localized swelling, redness, heat), - Spontaneous dehiscence of wound or deliberate opening of wound by surgeon (unless site’s culture results are negative), - Purulent discharge from wound or drain placed in wound, - Abscess or evidence of infection on direct examination or reoperation or histopathologic or radiologic examination, - Diagnosis of infection by a surgeon or attending physician. Deep incisional SSI. Infection involves deep tissues, such as fascial and muscle layers. This also includes infection involving both superficial and deep incision sites and organ/space SSI draining through incision. Criteria: 1. Occurs within 30 days after surgery with no implant (up to one year after surgery if implant is left in place); 2. Infections involves deep soft tissues, fascia and muscle layers; 3. At least one of the following: - Purulent drainage/organism isolated from aseptically obtained culture, - Fascial dehiscence or deliberate opening of the fascia by a surgeon due to signs of inflammation, - Abscess or other evidence of infection noted below fascia during reoperation, radiologic exam or histopathology, - Surgeon declares that a deep incisional infection is present. Organ/space SSI. Infection involves any part of the anatomy in organs and spaces other than the incision, which was opened or manipulated during operation. Criteria needed to the diagnosis: 1. Occurs within 30 days after surgery or within one year if an implant is present and infection seems related to the operation 5 2. Infection involves joint/organ/space, anatomic structures opened or manipulated during the operation; 3. At least one of the following: - Purulent drainage from a drain placed into the organ/space, - Organism isolated from aseptically obtained culture from joint fluid or deep tissue, - Abscess or other evidence of infection involving joint, organ, space during re-operation, radiological exam or histopathology, - Diagnosis of organ/space SSI by surgeon. 1.3.6. Prevention of the wound contamination 1. Perioperative antimicrobial prophylaxis (preventive antibiotic treatment) should be applied in case of septic operation or in high-risk patient. 2. Blood glucose level has to be normalized. 3. Oxygen tension of the tissue has to be maintained, hyperoxygenation should be applied during the operation. 4. Body temperature has to be maintained on normal level during the operation. Narcosis deteriorate temperature regulation, the evolving surgical hypothermy + narcosis cause vasodilation, therefore the temperature further decrease. 5. Before the operation fur and hair should be removed because these harbor bacteria. 6. Thorough scrubbing before the operation is highly important. If necessary, changing the gloves and repeated scrubbing is needed. In the postoperative period hand disinfection and the use of sterile gloves is mandatory for sterile wound management. 7. Adequate surgical technique should be applied (careful handling of the tissues, control of bleeding, diathermy, applying absorbable sutures, proper suture technique, etc.). 8. It is important to know and control the risk factors. 1.3.7. Risk factors of wound contamination 1. Systemic factors Age (elderly or children), undernourishment, obesity, hypovolemia, bad perfusion, steroid therapy, immunosuppressive states. In the latter case the surgical intervention should be done exclusively in aseptic circumstances in the sterile operating room. The patient has to be isolated, and hospitalized in sterile circumstances, strictly maintaining the rules of asepsis. Wound management should be performed under „operating room circumstances”. Diseases connected to altered immune response: diabetes mellitus, cirrhoses, and uremia. 6 2. Factors related to the wound Dead or devitalized tissue left in the wound, hematoma, foreign body, including drains, sutures, dead space, improper skin scrubbing, disinfection and shaving, previously existing infection (local or distant). 3. Factors related to the operation Bad surgical technique, inadequate handling of bleeding, long-lasting surgical interventions (>2 h); intraoperative infection, non-sterile operating room personnel, instruments, improper air-exchange, hypothermy; long preoperative hospitalization. 4. Type of the operation Risk factor can be the type of the operation itself, as in certain operations the risk of wound contamination is higher than the average. Surgical wounds can be categorized according to the hazard of the wound contamination as clean, clean – infected, infected and spoiled – infected groups. Infective Risk (%) Classification Description Clean (Class I) Uninfected operative wound No acute inflammation Closed primarily Respiratory, gastrointestinal, biliary, <2 and urinary tracts not entered No break in aseptic technique Closed drainage used if necessary Cleancontaminated (Class II) Elective entry into respiratory, biliary, gastrointestinal, urinary tracts and with minimal spillage <10 No evidence of infection or major break in aseptic technique Example: appendectomy Contaminated (Class III) Nonpurulent inflammation present Gross spillage from gastrointestinal tract About 20 Penetrating traumatic wounds <4 hours Major break in aseptic technique Purulent inflammation present Preoperative perforation of viscera About 40 Penetrating traumatic wounds >4 hours Source: CDC, 1996 Dirty-infected (Class IV) 1.3.8. Postoperative wound management Decisive factor is the rigorous maintaining of the rules of asepsis. Primarily closed wound is covered with sterile covering bandage for 48 hours. Hygienic hand washes before and after the wound management is mandatory. Sterile technique must be applied in changing the covering bandage. 1.4. Sterilization Definition 7 The removal of viable microorganisms (every pathogenic and apathogenic microorganisms including the latent and resting forms such as spores), which can be achieved by different physical (heat, steam, irradiation, etc.) and chemical means and methods (ethylene oxide, etc.) or by their combined effects to kill or inactivate each living microorganism as well as of their latent and resting forms. 1. Autoclaves Autoclaves are highly effective and inexpensive tools of sterilization. Its effectiveness is based on the fact that steam temperature under pressure > 100 °C: in case of 108 kPa it means 121C (vacuum has to be created).When the steam pressure is 206 kPa, its temperature is 134C. The time needed to the sterilization is 15 min at 121 °C and 3 min at 134 °C. To be effective against viruses and spore forming bacteria the steam must be in direct contact with the materials. Effectiveness can be checked by the color-change of the indicator tape placed on the packing. Disadvantage: unsuitable for heat-sensitive objects. 2. Gas-sterilization by ethylene oxide Highly-penetrative and active against bacteria, spores and viruses. It is suitable for heatsensitive items. Disadvantage: flammable, toxic and expensive and leaves toxic residue on sterilized items and therefore instruments sterilized in this way need to be stored for prolonged period (airing) before use. 3. Sporicidal chemicals – cold sterilization Sporicidal chemicals often used as disinfectants but can also sterilize instruments if used for prolonged period. The advantage of these methods is that inexpensive and suitable for heatsensitive items. The disadvantage is that they are toxic and irritants. The most widely used liquid sporicidal chemical is 2% glutaraldehyde (Cidex). It is able to kill most bacteria and viruses within 10 minutes (spores can survive several hours). 4. Irradiation The gamma rays and accelerated electrons are excellent at sterilization. They are used for industrial purposes, for cold sterilization of disposable items (plastic syringes, needles) and materials (bandages) rather than for sterilization in hospitals. 1.5. Disinfection The reduction in number of viable organisms, the diminution of the number of propagating microorganisms by destroying or inactivating them on living or inanimate (nonliving) surfaces. Can be achieved by generally used methods with the aid of chemicals (disinfectants, glutaraldehyde, formaldehyde, quaternary detergents, etc). Some of these disinfectants are sporicidal but generally they should not be used for sterilization because most items need very long time (up to 10 hr or more) of soaking in order to render them sterile. 1. Low-temperature steam Most bacteria and viruses are killed by exposure to moist heat. Usually achieved with dry saturated steam at 73 °C applied for more than 10 minutes. Effective, reliable and suitable for instruments with a lumen or caverna. Unsuitable for heat-sensitive items. 2. Chemical disinfectants Disinfectants are suitable for heat-sensitive items as well, however less effective than heat. Destroys microorganisms by chemical or physicochemical means. Different organisms vary in their sensitivity against them: - Gram-positive bacteria are highly sensitive; - Gram-negative bacteria are relatively resistant; - Clostridial and Mycobacterial species are very resistant; - Slow viruses are highly resistant. The use of antiseptics (application, how to make the solutions, the effective concentration, the time needed for the effective disinfection of the different chemicals, etc) is regulated in 8 official guidelines (e.g. „Handout of disinfection and disinfectants” by the Hungarian National Health Center -OEK). Chemicals used include clear soluble phenolics, hypochlorites, alcohols, quaternary ammonium compounds. 1.6. Asepsis and the surgical patient Asepsis (in a wider sense) became a fully elaborated routine procedure. The rules of asepsis must be maintained in case of the patient, the operating room personnel, the operating theater, operating room devices, tools and instruments as well. Surgical asepsis needs strict precautions, working in a sterile field presupposes the understanding that violation of the technical rules may cause fatal infections. 1.6.1. Preparation of the skin before the operation Skin harbors resident flora (these bacteria cause no harm unless drawn into the body through a break in the skin, e.g. Staphylococcus epidermidis) and transient flora (acquired from a contaminated source) and this includes any type of bacteria that can live on skin. 1. Bathing It is not unequivocal that bathing lowers germ count of the skin but in case of elective operations pre-operative antiseptic showers/baths are compulsory. Special attention is given to the operative site. It should be done with antiseptic soap (chlorhexidine, quaternol) the evening prior to operation. 2. Shaving Makes surgery, suture and dressing removal easier. Must be performed immediately prior to operation, with the least cuticular/dermal injury, in this case the wound infection rate is only 1 %. The infection rate is increased to 5% or >5% if it is performed > 12 h prior to surgery (abrasions can cause colonization which can lead to wound infection). Clippers or depilatory creams reduce infection rates to < 1%. 3. Preparing the skin It is performed the day before the operation (in elective cases). Disinfectants are applied to the skin: 70% isopropyl alcohol (acts by denaturing proteins, bactericidal but short acting, effective against Gram + and Gram – organisms, fungicidal and virucidal); 0.5% chlorhexidine (quaternary ammonium compound, acts by disrupting the bacterial cell wall, bactericidal but does not kill spore forming organisms, persistent and has a long duration of action (up to 6 h), more effective against gram-positive organisms); 70% povidon–iodine (Betadine, acts by oxidation / substitution of free iodine, bactericidal and active against spore forming organisms, effective against both Gram + and Gram – organisms, rapidly inactivated by organic material such as blood, patient skin sensitivity is occasionally a problem). 1.6.2. Surgical skin preparation (prep) - It is performed after surgical hand scrub, before dressing (gowning – e.g. putting on sterile gowns). - All supplies used (towels, gauze sponges, sponge forceps and gloves) must be sterile. - Starting at the exact location where the incision will be made, begin washing (with antiseptics) moving outwards in a circular motion. Use a "no touch" technique. - Scrub outward from the incision site and discard used prep sponges and begin again with fresh ones. Do not return to an area already washed with the same sponge. 9 - Prepped/disinfected area must be large enough for the lengthening of the incision / insertion of a drain. - The skin prep is generally consists of two phases (it must be made according to the accepted and generally applied rules of the operating room). Classical: 1. removing the fat of the skin surface with petrol; 2. antiseptic paint is applied (2x) immediately (1-5 % iodine tincture). Currently: antiseptic paint (usually povidone-iodine) is applied twice (alcohol, Dodesept solution could be used in case of sensitive skin) - The preparation of the operating area is made by sterile sponges (gauze balls) mounted in a sponge holding clamp. In aseptic surgical interventions the procedure starts in the line of the planned incision, in case of septic, infected operations from the periphery toward the planned area of the operation. 1.6.3. Isolation of the operating area (draping) - After the skin preparation the disinfected operating area must be isolated from the nondisinfected skin surfaces and body areas by the application of sterile linen textile, sterile water-proof paper, or further sterile accessories/supplements. The isolation prevents contamination deriving from the patient’s skin. Draping is performed after the surgeon has donned gown and gloves. - The usefulness of the sterile self-attaching synthetic adhesives (affixed to the disinfected operating area) is questionable for the prophylaxis of postoperative wound infections, because these can help residual bacteria to come to the surface, due to the increased perspiration during the operation. - Because the deeper layers of the disinfected skin always contain residual bacteria, the skin can be touched neither by instruments nor by hands. - The isolation is generally performed by disposable sterile sheets which are attached to the patient’s skin where they cross by self-attaching surfaces. Non-disposable, permeable linen textiles are fixed to the skin with special clips. - In general surgical operations (e.g. abdominal operations) the scrub nurse and the assistant make the draping with the specially folded sheets. The first sheet isolates the patient’s leg. Then the Mayo-stand is moved to the end of the operating table. The second sheet is used to isolate the patient’s head; this sheet is fixed by a towel-clip to the guard which shields the anesthesiologist from the operative field. Then follows the placement of the two side-sheets. The isolated area is always smaller then the scrubbed area. Sheets after placed to the patient can not be moved toward the operating area, only toward the periphery, because pathogens can be transferred from the non-disinfected parts to the surgical area. Four Backhaus towel clips are fixing the sheets to the skin, the small puncture wounds heal quickly. - A special full sheet may be applied, too. It is positioned so that a hole incorporated in it lies over the operative site. Four towel clips are applied to attach the sheet to the patient’s skin. 1.7. Basic rules of asepsis in the operating theater The rules of asepsis are based on very fundamental principles. Sterile surfaces, those that are free of living microorganisms must not come into contact with non-sterile surfaces. Contamination of equipment and personnel is prevented by sterile linen or paper covering. 10 Contamination by an intermediate source such as dust and moisture is minimized by reducing or eliminating the source. 1.7.1. Positioning of the surgical patient The surgical patient can be positioned on his back (standard positioning, e.g. abdominal operation), on his side (e.g. thoracic surgery), or lying on the abdomen (e.g. varix operation). Some type of positioning must be separately mentioned. Prone position This position is used for craniotomy when the patient is laid face downward on the abdomen. Modification of the prone position (lying on the abdomen). The patient lies in prone position, with the table broken at its midsection so that the head and feet are lower than the midsection. Supine position Used for abdominal procedures and for those involving the face and neck, chest or shoulder. The head is in good alignment with the body. Vascular surgery is also performed in this supine position. Trendelenburg-position (sec. Friedrich Trendelenburg (1844-1924) German surgeon described it in 1881). Upside down (450 head down) position. Indication: depression of venous pressure (varicose vein surgery), restrains small intestine from the pelvis (gynecology, laparoscopic surgery). The goal is to allow the abdominal contents to drop in a cephalic direction (toward the head) thus giving greater exposure to the pelvic content. Physiological effects of Trendelenburg position: elevated venous reflow, raised intracranial and intraocular pressure, increased intragastric pressure → reflux of the gastric content, venous stagnation on the face and neck. Reverse (or anti–) Trendelenburg position is used for surgery of the face and neck and for procedures involving the diaphragm and upper abdominal cavity, since it allows the abdominal contents to drop in a caudal direction (toward the feet). Physiological effects: reduced venous reflow → cardiac output falls, mean arterial blood pressure decreases, improvement in the functional residual capacity (FRC) of the lung. Lateral position. Indications: thoracotomies, renal, shoulder surgery and hip operations. It can cause problems because it may change respiratory function. Lateral decubitus: the table is flexed in the centre in addition to the lateral position. Indication: nephrectomy. Problems: direct caval compression→ decreased venous return and hypotension. Lithotomy „legs up” position. Indications: gynecological and anal surgery. Potential problems: autotranfusion from the leg vessels will increase preload (the effect on CO will depend on the patient’s volume status), vital capacity is decreased, and risk of aspiration is increased: anesthesia should never be induced in this position! Kraske (jackknife or "knee-chest") position. Indication: proctology – rectal, perianal, coccygeal surgery. 1.7.3. Surgical personnel and the asepsis - Only those people whose presence is exclusively needed should stay in the operating room. - Avoid activity causing superfluous air flow (talking, laughing, sneezing, walking around). The atmosphere of the operating theater must be quiet and peaceful, movement and talking have to be kept to a minimum during surgery. Talking releases droplets of moisture laden with harmful bacteria into the air around the sterile field. 11 - Entering the operating theater is allowed only in operating room attire and shoes exclusively worn in the operating room. All the dresses have to be changed except the underwear. This complete change over should apply also for the patient who is placed in the holding area to the garments used in the operating theater. Leaving the operating area is forbidden in surgical attire. - The doors of the operating room must be closed. - Only in cap and mask covering also the hair, mouth and nose is allowed to move in the operating room out of the holding area. If the mask became wet it should be replaced. 1.7.4. Personnel attire in the operating room - Strict personal hygiene is necessary for the operating room personnel. Taking part in an operation can be possible only after surgical hand wash and scrubbing. Scrubbing person must not wear jewels. Watch and rings should be removed. Fingernails should be clean and short, nail polish is forbidden. Surgical scrubbing always has to be made according to the accepted and generally applied rules of the local operating suite. - Surgical team members in sterile attire keep well within the sterile area; the sterile area is the space that includes the patient, surgical team members, sterile equipment tables and any other draped sterile equipment. - Non-scrubbed personnel do not come close to sterile field or scrubbed sterile person, do not reach over sterile surfaces and handle only non-sterile instruments. - Scrubbed team members always face each other, never show back to each other. They face the sterile field at all times. - Airway infection or open excreting wound exclude taking part in the operation. 1.7.4.1. Scrubbing, disinfecting, gowning in general In order to minimize the risk of infection it is essential to follow the correct procedure before entering the surgical suites and operating areas. Wearing the proper scrub suit is required. Surgical attire acts as a barrier that protects patients from exposure to microorganisms that could cause postoperative infections. This barrier includes surgical gloves, caps, masks, gowns, protective eyewear, waterproof aprons, and sturdy footwear. They all must be the right size and properly worn. 1. Scrub suit It is put on in the dressing room before entering into the operating theater. Scrub suit must be changed if it becomes soiled. 2. Surgical caps The hair, mouth and respiratory tract are rich in bacteria. The cap should completely cover the hair. 3. Face mask The mask should be tied securely. It must be comfortable to wear, as it will be worn throughout the procedure. Masks should cover the nose and mouth, fitting snugly across the bridge of the nose, at the edge of the cheeks, and under the chin. Masks should be changed between cases or when they become wet (usually from breath). They should never be worn dangling around the neck. Rubbing ordinary soap on glasses and polishing them is the most satisfactory way to prevent fogging of glasses. 4. Shoes 12 If outside shoes are worn in the operating room shoe covers must be worn. These plastic overshoes (booties) should be worn over normal footwear. 5. Gowns Long-sleeved sterilized surgical gowns or disposable coveralls are worn. Remember, surgical gowns are considered sterile in front from the chest to the level of the sterile field. Sleeves are sterile from 5 cm above the elbow to the cuff. The neckline, shoulders, underarms, and back of the gown are considered to be non-sterile. Gowns should be put on after surgical scrub and before gloving. 1.7.4.2. Detailed steps of dressing 1. Scrub suit 1. Dressing: To put on: scrub suit operating room shoes/shoe cover) To remove: -bracelet -ring -wristwatch -nail-polish No one should enter the operating room wearing street cloth or clothes worn elsewhere in the hospital. All surgical personnel must wear scrub suit. The scrub suit is put on in the dressing room. Outside shoes must be changed for operating room shoes or wear shoe cover. 2. Cap and mask The cap and mask should be donned first. Positioning the mask Correct position of the mask right 13 wrong 3. The scrub preparation and surgical disinfection The surgical hand and arm scrub procedure must be performed in the scrub suite before entering the surgical suite/operating room. To maintain the asepsis hand and arm scrub is performed according to the basic rules of asepsis. 3. Scrubbing Participation in a surgical intervention requires the implementation of the complete protocol of scrubbing and disinfection. • The goal of scrubbing To reduce the number of transient and resident bacterial flora and to inhibit their activity. Scrubbing have to be made according to accepted and generally applied rules of the local surgical suite. (Green colour indicate the sterile field as a result of scrubbing) Simple scrubbing with soap is not = disinfection! Scrubbing is done according to the Ahlfeld-Fürbinger-type two phase scrub (5 min mechanical and 5 x 1 min rubbing with disinfectant hand scrub agent). A systematic approach is an efficient way to ensure proper technique. Scrubbing 1. handwash with soap Scrubbing 2. Hand- and armwash with soap Scrubbing 3. Steps of rinsing the hands Taking out the brush 14 Scrubbing 4. Do not touch the basin! cleansing the nails with brush The goal of scrubbing is to remove the outer, desquamating, oily layer of the skin which harbors many microorganisms. The basic principle of the scrub is to wash the hands and arms very thoroughly from a clean area the hand to a less clean area the arm. The scrub procedure must include all anatomical surfaces from the fingertips to approximately 2 inches above the elbow. The so-called timed-scrub should last 5 minutes and consists of the following: 1. Remove watch and rings. 2. Cut nails if necessary and clean subungual areas with a nail file. Discard the nail file in the sink 3. Turn the tap and adjust the water to a proper temperature and flow rate. Start timing! 4. Wash your hands and forearms with liquid- or foam soap thoroughly. Rub each side of each finger, between the fingers, and the back and palm of the hands with soap. After the hand is scrubbed, the arm is scrubbed. Rub the soap on each side of the forearm from the wrist to the elbow to at least 3 finger-breaths above the elbow, keeping hand higher then the arm at all times. This prevents bacteria-laden soap and water from contaminating the hand. If at any time the hand touches anything non-sterile object, the scrub must be lengthened by 1 minute for the area that has been contaminated. 5. Rinse hands and arms with water, keeping your hands above the level of your elbows, and allow water to drain off the elbows. 6. Take a sterile brush in one hand and the soap in the opposite one. 7. Make a good lather on the brush and brush your nails and finger tips only. To brush any other part of the hand is forbidden. 8. Finishing scrubbing, put the brush aside. 9. Rinse both hands and arms thorougly with tap water. Keep the hands higher than the flexed elbows to allow the water to drip off the elbows and to prevent it from running from the upper forearm down on the hands. Rinse hands and arms by passing them through the water in one direction only, from finger tips to elbow. Do not move the arm back and forth through the water, but move only in one direction, from the fingers toward the elbow. When rinsing, do not touch anything with your scrubbed hands and arms. 10. The taps should be turned off using the elbows and allow the hands and arms to drip dry for a short time (or use sterile towel to dry it.). Note: no matter what agent is used, or which scrub technique you practice, there is only one goal: infection prevention. Effective surgical scrubs are one of the most powerful strategies of infection prevention in the operating room. Glove usage gives a false sense of security against bacteria. Gloves provide an ideal environment for bacterial growth, moisture and warmth, which makes good hand-scrub techniques and aseptic gowning and gloving an important part of the total infection prevention platform. 15 11. Disinfection with alcohol-based hand- and arm-rub Disinfection 1. Steps of chemical disinfection 2. right wrong Here Bradosept is used which is an alcoholic detergent. 5 x5 ml should be used, each dose for 1 minute. - Keep your palm below the tubing of the dosing wall-apparatus so that the hand is at the same level with the eye of the photoelectric cell. Do not touch either the apparatus or the tubing. If you keep the hand properly, one dose of antiseptic will flow into your palm. - Rub in the hands and arms with the antiseptic thoroughly for 1 minute. Repeat the process 4 times more. Do not rinse your hands or dry them with sterile towel. Bradosept not simply inactivates bacteria, but it fixes skin too, i.e. a layer will be formed which prevents bacteria from coming to the surface from crypts. If at any time the hand touches anything non-sterile object, the scrub must be lengthened by 2 more 1 minute-long disinfecting steps for the hands. Recent studies have shown that using a brush to scrub hands during surgical scrub provides no greater reduction in the number of microorganisms on the hands than scrubbing with antiseptic alone. Surgical scrub may be performed using either a soft brush or sponge or the combination of these and an antiseptic alone. Avoid using a hard brush, which is not necessary and may irritate the skin. 4. Gowning - The scrubbed personnel enter the surgical suite immediately after the scrub. The hands are held above the elbows, in front of the chest. - Go to the so-called Schimmelbush container that is on a stand. Open up the cover with the foot pedal. - Pick up a sterile gown with your right hand while keeping the others with the left hand to prevent them from pulling out. The gown is folded so that the inner surface is exposed to you when you pick it up. If you are gowning yourself, grasp the gown firmly and bring it away from the container. Never touch the outer surface. - Step far enough away from non-sterile objects while dressing to allow a wide margin of safety. 16 - Hold the gown at the edges of the neck piece, out away from your body and the container and sufficiently high so that it will not touch the floor. - Holding the gown by the inside at the neckline allow it to unfold gently ensuring that the gown does not come into contact with anything non-sterile. - Gently shake folds from gown and insert both arms into the armholes, keeping your arms extended as you do so. Wait for the scrub nurse to assist you by pulling the gown up over the shoulders and tying it. - The scrub nurse grasps the inner surface of the gown at each shoulder and pulls the gown over your shoulder and the sleeves up over the wrist. The scrub nurse assists you in fastening the gown at the back. Note: do not grasp the girdle of the gown but wait until the nurse helps you. Keep your hands above the level of your waist and do not touch anything. Keep hands above the level of your waist and below nipple line at all times. Do not touch the sterile chest field with ungloved hands. Do not touch the sterile operating field or anything sterile before putting on sterile surgical gloves. Effective „sterile” area 4. Gowning Certain parts of the gown can not be considered sterile (!) a. the back and the axillaries b. lateral from the axillaries c. under the waistline d. the sleeves 10 cm distance from the shoulders over the elbow. 5. Gloving Because the skin cannot be sterilized, sterile team members should put on sterile rubber gloves if they have already been gowned. To diminish friction between the skin and the glove, sterile talcum powder is used. The gloves have been lightly coated with powder. The gloves are packed individually in container consisting of two pockets, one for each glove. If a sterile nurse is available she can glove you. 17 Gloving of the left hand 1. Glowing of the right hand 2. • from inside! from outside! The gloved hands - The sterile nurse holds the left handed glove open with her fingers beneath the cuff so that her glove does not come in contact with your skin. The palm of the glove faces to you. - Put two fingers of your right hand into the opening; pull the inner side of the glove toward yourself so that a wide opening is created. Slip your left hand into the gloves so that the glove cuff covers the sleeve cuff. - When you put on the right handed glove, place the fingers of your gloved left hand under the right glove cuff to widen the opening and thrust your right hand into the glove. - You may now adjust your gloves so that to fit comfortably on the hands. Now you are ready for taking part in an operation. If your gloves become soiled or damaged, you must change them at once. Sterile gloves are a thin barrier between sterility and contamination. Never allow bare hand to contact the gown cuff edge or the outside of glove. 6. Removing gloves Grasp the cuff of your dirty left-hand glove and pull it down so that it should hang over down from your finger in „inside out” mode, than repeat the process with the other one. Now you can take off both gloves one by one without touching the outer dirty surfaces. 18 Removing the gloves Step 1. Grasp one of the gloves near the cuff and pull it partly off. The glove will turn inside out. It is important to keep the first glove partially on your hand before removing the second glove to protect you from touching the outside surface of either glove with your bare hands. Step 2. Leaving the first glove over your fingers, grasp the second glove near the cuff and pull it partly of the way off. The glove will turn inside out. It is important to keep the second glove partially on your hand to protect you from touching the outside surface of the first glove with your bare hand. Step 3. Pull off the two gloves at the same time; be careful to touch only the inside surfaces of the gloves with your bare hands. In general, just remember, that hands must always be kept within the sterile boundary of the gown. The hands and arms are held up in front of the body with elbows slightly flexed while entering the operating room. Care should be taken not to touch anything with the hands or arms. If you are sterile, do not touch anything that is not sterile and vice versa. The back of your gown and anything below the waist is considered not sterile or contaminated. Your mask, protective eyewear, and hat are also non-sterile. 19 Effective „sterile” area Certain parts of the gown can not be considered sterile (!) a. the back and the axillaries b. lateral from the axillaries c. under the waistline d. the sleeves 10 cm distance from the shoulders over the elbow. 1.4.4. Moving in the operating room The operating room personnel have to work according to the rules of asepsis to ensure an aseptic germfree wound state. - Sterile personnel keep well within the sterile area Operating team members should move about the suite as little as possible. With excessive movement dust and air currents are swept about thus spreading bacteria. - Sterile team members face each others. They face the sterile field. The back is never turned on the sterile field. The back of the gown should be considered non-sterile. The axillary region is not sterile. -When sterile team members pass each other they pass back to back or chest to chest. - Excessive talking and laughing during surgery increases the possibility of wound contamination by bacteria from the mouth and throat. - Hands must be kept within the sterile boundary of the gown. - Sterile personnel can handle only sterile equipment. 1.4.5. The general rules of asepsis related to the operating equipment - Equipment used during a sterile procedure must be sterilized. - Sterile personnel handle only sterile equipment. 20 - If the sterility of an item or a person is questionable the item or person is considered contaminated. - Sterile tables are sterile at table height. - Gowns are sterile in front from the axillary line to the waist, and the sleeves to 3 inches under the elbow. - The edge of any container that holds sterile supplies is not sterile. - Some operative areas (nose, throat, mouth, perineal region, digestive tract etc. can not made sterile. Steps are taken to keep contamination to a minimum. 1.4.6. Further important duties to secure asepsis and to avoid wound contamination - Changing gloves: during the operation (e.g. after the opening of the bowel) gloves presumably contaminated by pathogenic microorganisms must be changed. Gloves must be replaced if the gloves become injured, and also during sustained operation, and naturally between two operation as well. In the latter case a repeated disinfecting or a new scrubbing procedure is needed as well. - Instrument change: potentially contaminated instruments must be dropped into the container (e.g. scalpel, used to incise the skin or to open a bowel) and other instruments must be replaced. - Covering the surgical wound: by sterile wound cover. - Closed circuit drainage must be applied for the drainage of the confluent fluid collected in the wound and of oozing blood. - Easily cleanable and sterilizable metal instruments or disposable instruments and suture materials, plastic canules, drains and vascular prosthesis must be used. - The aseptic and septic operations must be separated in time and space as well, but at least in time: aseptic operations (e.g. hernia operation, thyroidectomy, varix operation) must be carried out in sterile (aseptic) operating room, pathogenic, septic operations (colon, appendectomy, hemorrhoidectomy, fistula) in septic operating theatre. In case if these can not be separated spatially, aseptic operations must be done first and thereafter the septic cases. After the finishing of these surgical interventions operating theater must be cleaned up and disinfected. 1.4.7. Asepsis in the postoperative period - Patients after aseptic and septic operative interventions should be separated. If it is possible, place them in separate rooms in the hospital. - Change of bandage is done only when indicated. - Change of bandage is first done on the aseptic patient. - Changing of bandage needs sterile instruments and sterile bandages. - Before and after the change apply hand wash with antiseptics and use new sterile gloves in every case. 1.5. The surgical antisepsis It is much less effective than prophylaxis. Killing or inactivating pathogenic germs got to the wound (see later) by the application of antiseptic solutions, powders (hydrogen peroxide, povidon-jodid, boric acid etc.) locally or by antibiotic treatment. 1.6. The operating room, furniture, techniques 21 The operating rooms (operating suites) are similar in design. The pattern is always simple, in order to be easy to keep clean and decontaminate, to avoid dust to accumulate in areas that would be difficult to clean. Wall and floor surfaces are smooth and made of nonporous material. The operating room is roomy enough to allow scrubbed personnel to move around non-sterile equipment without their contamination. 1.6.1. The equipment of the operating room The standard operating table It may be manipulated in many different ways to achieve the desired position of the patient. The table top is sectioned in several places and may be reflexed or extended. The table can be flexed at one or more hinged sections, may be tilted laterally or horizontally and raised or lowered from its hydraulic base. Sections of the table such as the headboard or footboard may be removed as needed. The position and height of the table are dictated by the situation of the organ to be exposed and by the surgeon’s comfort. The ideal height of the operating table places the operative field approximately at the level of the surgeon’s elbow when his arm is at his side. Small instrument stand (Mayo stand) A special type of instrument table that is placed directly over (but not in contact) with the patient's leg. It is used to hold instruments that will be used frequently during the surgical intervention. Back table (large instrument stand) Extra supplies additional instruments used during the surgery are placed on the back table. Kick bucket Soiled (spilled) sponges and some instruments e.g. sponge holding clamp used for scrub preparation should be dropped into containers at the side of the table. Instruments needed during the operation - anesthesia equipment with gas machine and physiological monitor - monitor used to control blood parameters as blood pressure (two components), blood volume, cardiac output and to follow electrocardiogram - outlet for gases (oxygen, nitrous oxide) - outlet for suction (one for the anesthesiologist to keep the patient’s airway clear of mucous secretion, one for the surgical team to suction blood and irrigation fluids from the wound site), - AMBU-balloon (manual respirator), - endotracheal tubes, - suction catheter (to remove body fluids) - central venous catheter 22 - Ringer-lactate infusion set - ECG-pads - different venous catheters (Braunules-canules with wings) - urinary sack - Foley catheters of different size - diathermy unit (see later: electrocautery or electrosurgery) 1.8. The operating room personnel The position of the operating team at the table will vary depending upon individual circumstances, the situation of the organ. The surgeon stands on one side of the operating table. The first assistant is usually opposite the surgeon. On the other side of the table beside the first assistant, opposite the operator, stands the scrub nurse. The second assistant stands on the left or right of the operator. The position of the surgical team 2. ASSISTANT SURGEON ANESTHESIA 1. ASSISTANT SCRUB NURSE The green line marks the sterile area; the red color is the border of this field. Stepping behind this line is forbidden. 1.7.1. Duties and responsibilities of the operating room personnel Surgeon: the person who ultimately guides the flow and scope of what happens in the surgical suite. Primarily responsible for maintaining the asepsis; controls all the activities in the surgical suite during the procedure. Scrub nurse: assists in the sterile gowning and gloving of the surgeon and his/her assistant. Responsible for the maintenance of an orderly surgical field; prevents contamination of the surgical field by the strict practice of aseptic technique; must remind the surgeon and all members of the operating team if she perceives any error in maintaining the asepsis. 23 First assistant: works under the direct supervision of the surgeon and assists in such duties as hemostasis, suturing and wound dressing. The first assistant’s responsibility is to position the operating table and the light, so that the field will be properly illuminated. Second assistant: provides exposure of the operative field. He carries out the orders of the surgeon or that of the first assistant. He should restrict his activities to holding instruments and retractors as instructed by either the surgeon or the first assistant; Circulator / surgical technologist: surgical team member who does not perform a surgical hand scrub or don sterile attire, and thus does not work within the sterile field; he is responsible for the non-sterile fields. His obligation is to to carry the patient to the operating room, safely position the patient, and to keep clean the operating room. If you finished scrubbing do not - drop your hands below your waist, - touch your face or adjust your mask and glasses, - grab anything that falls off the table (but inform the circulating nurse), - reach for anything on the Mayo stand (but ask the scrub nurse for it). 1.9. The operating field before and after the isolation The operating field before the isolation of the patient Only the Mayo stand is sterile- green color marks the sterile area. 24 The operating field after the isolation of the patient The Mayo stand was moved over the patient legs. Green color marks the sterile field; the red color indicates the border of the sterile area. 1.10. Passing the instruments Instruments should be passed in positive and decisive manner. When an instrument is properly passed the surgeon will know he has it and will not have to move his eyes from the operative field. The scrub nurse and the assistants have to know what he wants by his signals. When he extends his hand the instrument should be slapped firmly into his palm, in proper position for use when he closes his hand on it. There are some widely accepted hand signals used at the operating table. These speed up the passage of instruments and eliminate much talking. Do not reach for instruments on the instrument table. Make an effort to keep the operating table neat, passing the instruments back to the scrub nurse immediately after they are used and removing soiled sponges from the field. Sponges should be dropped into the container at the side of the table. 25