Partner EC Provider Information & Consent Form 1011
advertisement

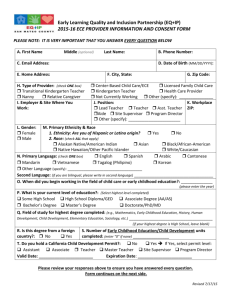
Early Childhood Quality Improvement Project (EQuIP) 2014-15 ECE PROVIDER INFORMATION AND CONSENT FORM **PLEASE NOTE: IT IS VERY IMPORTANT THAT YOU ANSWER EVERY QUESTION BELOW. PLEASE REVIEW THE QUESTIONS CAREFULLY AND ENSURE THAT YOU ANSWER ALL QUESTIONS** Today’s Date: _________________ Agency (Employer): ___________________________________________________ Site Name: ___________________________ A. First Name Classroom Name:_____________________________________________ Middle (optional) Last Name B. Date of Birth: / / D. Residential Street Address: E. City, State: G. Email Address: H. Phone Number: I. Primary Race/Ethnicity: (check ONE box) Alaska Native or American Indian Asian Pacific Islander J. Primary Language: (check ONE box) English Spanish Korean C. Gender: Male Female F. Zip Code: Black/African-American Hispanic/Latino White Multi-Racial Other (specify): _____________ Cantonese Mandarin English-Spanish Bilingual Vietnamese Tagalog (Pilipino) Other Bilingual (specify): ______________________ Other Language (specify)_______________________ K. Type of employment: (check ONE box) (If you are not currently working, check “Not currently working” and skip to Question #O) Center-Based Child Care/Preschool Licensed Family Child Care Family Support Professional Health Care Provider Not currently working Other: __________________ Workplace Name: ______________________________________________________________ Zip Code: ____________ If you are working in the field of Early Childhood Education, please answer questions L and M: L. What is your current position? Assistant Teacher Teacher Lead Teacher Supervisor Program Director/Administrator Other:__________________ M. How long have you been working in the field of Early Childhood Education (enter number of years)? ________ Years ******ANSWER ALL QUESTIONS BELOW (N - R )****** N. What is your current level of education? (Select highest level completed): Some High School High School Diploma/GED Some College Associate Degree (AA/AS) Master’s Degree Doctorate/PhD/MD Bachelor’s Degree O. Field of study for highest degree completed (e.g., Mathematics, Early Childhood Education, History, Human Development, Child Development, Elementary Education, Sociology, etc): __________________________________________________________ (if your highest degree is High School, you may leave Field of Study blank) P. Is the degree selected above from a foreign country? No Yes Q. Number of Early Childhood Education/Child Development units completed (enter “0” if none): _______________ R. If your highest level of education is High School or "Some College", enter the number of college General Education (GE) units completed here (enter “0” if none): _________ S. Do you hold a California Child Development Permit? No Yes If Yes, select your permit level: Assistant Associate Teacher Master Teacher Site Supervisor Program Director Expiration Date_______________ Please review your responses above to ensure you have answered every question. Please go to the next page to complete the form. CONSENT TO PARTICIPATE IN THE FIRST 5 SAN MATEO COUNTY EVALUATION I agree to allow the Early Childhood Quality Improvement Project (EQuIP)/San Mateo County Office of Education (SMCOE) to share information about me with First 5 San Mateo County (F5SMC) and their evaluators (including SRI International). This information will help F5SMC learn about the service providers with whom they work. I understand that: This form asks for my name, date of birth, zip code, ethnicity, language, level of education, and my history in the field of early childhood education. At some point during the program, I may be asked to complete a survey that asks me to rate my level of knowledge and skill as a service provider. I can skip any question I do not want to answer. Only a few people will be able to see my answers. Those people are not allowed to share my private information with anyone. Reports will not include my private information. There are no known risks to completing this survey. My answers might help to improve EQuIP and F5SMC activities for service providers in San Mateo County. It is very important to EQuIP and F5SMC that my information is safe, so it will be protected as required by law. If I do not complete this survey, I will still receive services from this program. My consent to share my answers will end 10 years from today. I can always change my mind and have my information erased. To do this I send a request to: EQuIP, San Mateo County Office of Education, 101 Twin Dolphin Drive, Redwood City, CA 94065. For more information, please call: 650-802-5345. I consent to take part in this evaluation. My information will only be shared with authorized individuals from EQuIP, First 5 San Mateo and their evaluators. Reports will never include my private information. Please print your name and sign and date below. ________________________________________________________________________________ Name of Individual (printed name) _________________________________________________________________________________ Signature Date Signed I do not consent to participate in this evaluation. The only people who will see my information are representatives of EQuIP/San Mateo County Office of Education. Please print your name, sign and date below. ________________________________________________________________________________ Name of Individual (printed name) _________________________________________________________________________________ Signature Date Signed Revised 9/10/2014