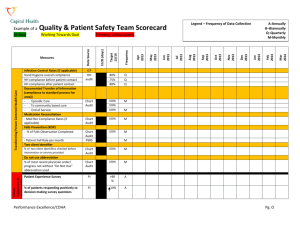
Quality & Patient Safety Scorecard Example
advertisement

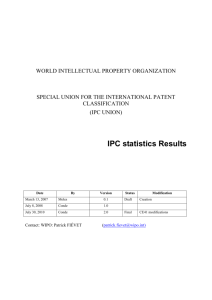
Transforming Person Centered Health Care Infection Control Rates MRSA # carriers on unit MRSA # of transmissions per month New cases of c. diff on unit per month - VRE # carriers on unit -VRE # of transmissions per month - Surgical infection rates (if applicable) Hand Hygiene (HH)– overall compliance - HH compliance before pt contact - HH compliance after pt contact Documented TOA or TOI (compliance) - TOA shift to Shift - TOA Unit to Unit (includes episodic care) Pressure Ulcer Prevention (ROP) - Braden Scale (on admission) Compliance Rates - Pressure Ulcer Prevalence Rates Medication Reconciliation - Med Rec Compliance Rates - Unintentional Discrepancies (if applicable) - Undocumented Intentional (if applicable) - Success Index (if applicable) Falls Prevention (ROP) - % of Falls Assessment Completed - Patient Fall Rate per month - % of falls causing injury VTE Prophylaxis Ordered ( PPO ) Wait time (if applicable) Version 2 updated May 2013 IPC IPC IPC IPC IPC IPC IPC IPC IPC IPC CA CA CA 0 M M M M M M Q Q Q 100 100 M M 0 0 100 CA M M CA CA CA CA 100 0 0 M M M M CA CA CA CA PI 100 M M M Q Q Mar 2014 Jan 2014 Dec 2013 Nov 2013 Oct 2013 Sep 2013 Aug 2013 Jul 2013 Jun 2013 May 2013 Apr 2013 Frequency Target 13/14 Measures A-Annually B–Biannually Q–Quarterly M-Monthly Trending Unfavourably Baseline Working Towards Goal Data Source At Goal Legend – Frequency of Data Collection Feb 2014 Example of a Quality & Patient Safety Team Scorecard Innovating Health & Learning Transformational Leadership Citizen Engagement & Accountability HSM/ PSRS HSM Y/N Absenteeism (illness) FTEs HSM Q # Inter-professional learning opportunities # (%) staff completed required annual patient safety education # (%) staff completed required annual hand hygiene education # (%) staff completed required annual O&HS education Version 2 updated May 2013 90% 90% ↑10 % A A A Q PI ↑20 % A PI ↑20 % A LMS A HSM Q HSM A LMS A LMS A Mar 2014 Feb 2014 Jan 2014 Dec 2013 Nov 2013 Oct 2013 Sep 2013 Aug 2013 Jul 2013 Jun 2013 May 2013 Apr 2013 Frequency Target 13/14 Patient Experience Survey - Inpatient - Ambulatory -% of patients responding positively to decision making survey questions Patient/Family/Client Complaints/Compliments Patient, Family or Client Engagement % of employees and physicians responding positively to leadership survey questions % of staff, management and physicians responding positively to accountability survey questions # (%) staff completing front line leadership program PI HSM HSM PI Baseline Data Source Measures Sustainability Readmission Rate % of patients discharge by 1100 AM ALC days Case Mix Group – Typical (# days) CMG# CMG # CMG # PI PI PI ALOS/ELOS/TARGET PI PI PI Mar 2014 Feb 2014 Jan 2014 Dec 2013 Nov 2013 Oct 2013 Sep 2013 Aug 2013 Jul 2013 Jun 2013 May 2013 Apr 2013 Frequency Target 13/14 Baseline Data Source Measures Q Q Q Q Q Q Guidelines for Scorecard The scorecard is to be used in conjunction with action template. The purpose of the scorecard is to: o align operational related team goals with Capital Health’s 2013 milestones and 2016 strategic goals o track trends for improvement in your care/service area o track and trend compliance to best practice, patient safety and accreditation Required Organizational Practices (ROPs) o track and trend adverse events prevalence and or incidence of ie falls, pressure ulcers, medication reconciliations; infection control measures; etc. The scorecard is to be populated monthly, quarterly or annually depending on the indicator and availability of data. The co-leads or those delegated by the co-lead are accountable for populating the scorecard. The scorecard should be regularly discussed at the Q& PS team members. Actions need to be taken to investigated and address concerning trends in indicators. To be used as evidence for development of a quality improvement action plan and quality initiatives. Instructions for Scorecard 1. Prior to use, please review Capital Health’s 2013 milestones, 2016 Strategic goals, patient safety indicators, Accreditation ROPs , Patient Experience surveys, Employee and Physician Surveys and your program goals 2. Consider areas and opportunities of interest for quality improvement Version 2 updated May 2013 3. 4. 5. 6. Referring to the Data Navigation Guide for details of where and how to obtain data Populate the Scorecard on a monthly, quarterly or annual basis depending of the frequency of data collection for each indicator Track trends Implement strategies for improvement based on evidence using the Action Template Data Source Legend IPC- Infection & Prevention Control CA- Chart Audit PI- Performance Indicators PSRS- Patient Safety Reporting system HSM- Health Services Manager LMS- Learning Management System Version 2 updated May 2013