Neuroscience 7b – Cortical Motor Function
advertisement

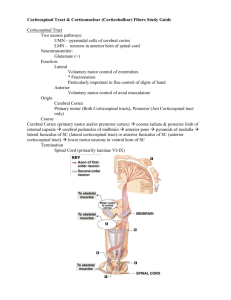
Neuroscience 7b - Cortical Motor Function Anil Chopra 1. Explain the importance of integration of sensory and motor systems in the voluntary motor control. 2. Know the organisation of the anterior and lateral corticospinal tracts from the motor cortex to a given motoneurons pool. 3. Explain the role of the pre-motor cortex and supplementary motor area in the planning of motor tasks 4. Explain how CNS damage can lead both to exaggerated motor activity (i.e. spasticity and hyper-reflexia) and at the same time depressed motor activity (i.e. weakness) 5. Explain how stroke affecting the motor cortex can produce symptoms and how plasticity in the nervous system can aid recovery. The different parts of the central nervous system are associated with different aspects of cortical motor function. Association Neocortex: uses information about where the body is in space (based on vision, audition and somatic sensations). The frontal lobe and limbic system generate the desire to move into a certain position by considering all the possibilities and then filtering them through the basal ganglia. Basal Ganglia: filter out the different options to decide the best plan of action. Motor Areas and Cerebellum: make the tactical decision. Brainstem and spinal Cord: cause the movement to be made accordingly by sending signals down the different tracts. Descending Pathways Extrapyramidal Pathways: these are indirect descending motor pathways that originate in: - red nuclei: rubro-spinal tract - reticular nuclei: reticulospinal tracts - vestibular nuclei: vestibulo-spinal tracts Corticospinal Tracts: most of the motor pathways descend in the pyramidal tracts. These are direct connections between the motoneurons in the primary motor and pre-motor corticies and those in the spinal cord. They cross over at the pyramidal decussation in the lower medulla oblongata to form the contra-lateral (lateral) corticospinal tracts. There are small number of fibres that remain uncrossed influencing muscles of the back, thorax and abdomen. Path of the Corticospinal tract: » Axons leave pyramidal cells and enter the white matter just below Layer VI. Every gyrus has this core of white matter entering and leaving the cortex » The slips of white matter form the corona radiata (radiating crown) » The corona radiata runs deeper into the hemispheres and splits the caudate and putamen nuclei in two » The axons are now called the internal capsule » At around the level of the mid brain the internal capsule coalesces to form a tight bundle – the cerebral peduncles or stalks of the cerebrum in order to exit the brain. These stalks form the floor of the brainstem and contain the descending motor fibres » After the mid brain it reaches the pons where the fibres split. Several synapse into the pontine nuclei to form corticopontine fibres. The remaining corticospinal tract gets fragmented and is no longer visible as a single tract, but as a number of smaller ones » In the medulla the corticospinal fibres come together again to form pyramids. Pyramids run the entire length of the medulla in the ventral surface » At the most caudal (bottom) part of the medulla the fibres cross the midline – decussation of the pyramids » As each individual fibre decussates it takes up position in lateral white matter of the spinal cord forming the lateral corticospinal tract. From here they dive into the ventral horn at the level of their target and synapse with α-motorneurons or interneurons » 15-20% of the corticospinal fires do not dross the decussation and so form the anterior corticospinal tract. The Internal Capsule: A major two-way highway Sensory information travels up to the cortex from the thalamus, motor information travels down from the cortex to the spinal cord It has two limbs: Anterior Limb Posterior Limb – further divided into the anterior part which contains the corticospinal pathway and the posterior part which contains sensory fibres going from the thalamus to the cortex The corticospinal tracts originate in three main areas of the cerebral cortex: Primary Motor Cortex (Brodmann’s area 4): 38% Premotor Cortex PMA and supplementary motor cortex SMA (Brodmann’s area 6): 30% Somatosensory cortex (Brodmann’s areas 1,2 & 3): 32% Corticospinal Tract Corticospinal tract has 2 parts The largest is the lateral corticospinal tract with 70-90% of the fibers It originates from primary motor cortex, premotor cortex and somatosensory cortex It crosses at the pyramidal decussation It projects to the lateral ventral horn and makes monosynaptic connections on the motoneurons of distal muscle. This enables fine independent finger movements premotor cortex Frontal lobe Parietal lobe Corticospinal Tract premotor cortex primary motor cortex primary motor cortex somatosensory cortex Anterior (ventral) corticospinal tract remains uncrossed until the spinal cord Here bilateral and polysynaptic connections are made on medial motoneurons of proximal and axial muscle These muscle are used primarily for posture It is not fully developed at birth Cortical Motor Areas Primary motor cortex: Low stimulation from the primary motor cortex is needed to produce a muscle movement. The activities relating to motor acts all converge on M1 (the primary motor cortex). NB: M1 contributes to most of the fibres in the corticospinal tract. A small population of cortical neurones in M1 controls small movements. These are movements that are specific, distal (i.e. fingers) and delicate/precise. Premotor Cortex: electrical stimuli from this area of the brain does not produce muscle movement unless the stimuli is very intense (much more so than in M1). This are of the brain prepares M1 for the motor act. It does this by facilitating multiple columns in M1. These neurones are more easily stimulated by impulses from other parts of the brain and are close to the threshold level needed to produce the movement. Lesions in the PMA do not cause paralysis but only result in the slowing of complex movements. Supplementary Motor Cortex: this area of the brain elicits complex movements involving many muscle groups (entire arm, hands and postural movements). It is not needed for simple repetitive acts that require little skill, and is particularly active when carrying out learned tasks. Ablation of this area results in inability to perform complex bimanual tasks + reduction in spontaneous motor activity. Lesions to the motor systems Upper motor neuron: all motor neurons from the cerebral cortex to the synapse in the spinal cord. Lower motor neuron: motor neurons that directly cause movement; i.e. peripheral motor neurons. Upper motor Neuron lesions Symptoms and signs: Weakness (initially) o Paresis = muscle weakness o Plegia = total loss of muscle control o Hemi = one side of the body o Para = affecting both legs o Quadra = affecting all 4 limbs. Spasticity (later) o Increased muscle tone in the affected voluntary muscles. o Hypotonia = dencreased muscle tone and weakness. Increase muscle stretch reflexes (hyperreflexia & clonus) Babinski sign: normally, when the lateral inferior surface of the of the foot is scratched from heel to little toe, the toes flex i.e. curl downwards, however, in an upper motor neuron lesion this is damages and the toes extend out and flare. Consequences of Stroke Stroke is the consequence of cerebrovascular disease that interrupts blood flow to part of the brain causing ischaemia and infarction. The diagnosis depends on establishing the time course and the symptoms: » Time course – symptoms develop over a few seconds to a few hours. Few other neurological conditions develop this quickly » Symptoms – Because stroke is of vascular origin the symptoms are often limited to the region in the brain and so functions dependant of the territory of a single vessel There are three causes of stroke: Thrombosis – ischaemic stroke Embolism – ischaemic stroke Haemorrhage – usually from a ruptured aneurysm An ischaemic stroke in the left middle cerebral artery would lead to: R-sided upper motor neuron facial weakness R-sided hemiplegia Severe speech disturbance - aphasia