QUIZ PAGE JUNE 2012 - Repositório do Hospital Prof. Doutor
advertisement

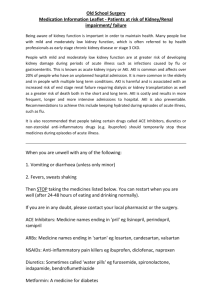
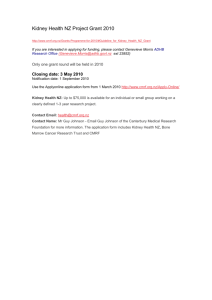
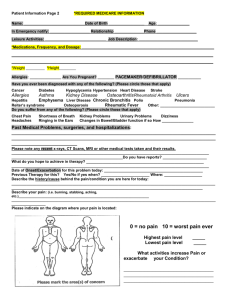
QUIZ PAGE JUNE 2012 Kidney Failure in an HIV-Positive Patient CLINICAL PRESENTATION A 71-year-old man was admitted with a recent decrease in kidney function. In March 2008, HIV (human immunodeficiency virus)-1 was diagnosed and cART (combination antiretroviral therapy) was started with atazanavir, tenofovir, emtricitabine, and ritonavir. Eight months later, he developed acute kidney injury (AKI) as his serum creatinine level increased from 1.0 mg/dL (88.4 mol/L; estimated glomerular filtration rate [eGFR], 79 mL/min/1.73 m2 [1.32 mL/s/ 1.73 m2] calculated using the 4-variable MDRD [Modification of Diet in Renal Disease] Study equation) to 4.3 mg/dL (380 mol/L; eGFR, 15 mL/min/1.73 m2 [0.25 mL/s/1.73 m2]), associated with glycosuria, microhematuria, and non-nephrotic proteinuria.Antiretroviral therapy was changed to atazanavir, abacavir, lamivudine, and ritonavir, with normalization of urinalysis results and a decrease in serum creatinine level to 2.4 mg/dL (212 mol/L; eGFR, 29 mL/min/1.73 m2 [0.48 mL/s/1.73 m2]). After a second AKI episode, kidney function progressively worsened, with persistent sterile leukocyturia and crystalluria. The patient received no other medications besides antiretrovirals. Viral load remained ⬍200 copies/mL and CD4 count was ⬎200 cells/L since the initiation of cART (Fig 1). On admission, physical examination findings were unremarkable. Laboratory data were significant for serum urea level of 187 mg/dL (67 mmol/L) and serum creatinine level of 7.1 mg/dL (628 mol/L; eGFR, 8 mL/min/1.73 m2 [0.13 mL/s/1.73 m2]). Urinalysis was negative for protein, glucose, and nitrites. Urinary sediment showed 75 leukocytes per high-power field, fine needle crystals, and no red blood cells or cellular casts. Test results for hepatitis B, hepatitis C, and cryoglobulin were negative. Ultrasound showed normalsized kidneys. A kidney biopsy was performed (Figs 2 and 3). Figure 1. Changes in serum creatinine level (solid line) and viral load (dashed line) since HIV (human immunodeficiency virus) diagnosis. Conversion factor for serum creatinine in mg/dL to mol/L, ⫻88.4. Abbreviation: AKI, acute kidney injury. Figure 2. ⫻200). Hematoxylin and eosin stain (original magnification, What are the kidney manifestations of HIV? How has cART changed HIV-associated kidney diseases? How do you interpret the kidney biopsy? Am J Kidney Dis. 2012;59(6):xxvii-xxx Figure 3. Epoxy resin semithin section stained with methylene blue (original magnification, ⫻200). xxvii QUIZ PAGE What is the most likely cause of the progressive decrease in kidney function in this patient? QUIZ PAGE JUNE 2012 ANSWERS DISCUSSION f What are the kidney manifestations of HIV? Kidney disorders are frequent in HIV infection at all stages (Box 1).1,2 Patients with HIV are at increased risk of AKI, with hypoperfusion being the most frequent cause.2 The most common HIVassociated glomerular injuries are due to focal segmental glomerular sclerosis, known as HIV-associated nephropathy, or to HIV immune-complex kidney disease. However, different diseases related to common comorbid conditions can be found.1,3 Box 1. Differential Diagnosis of Kidney Disease in HIV AKI ● ● ● ● CKD ● ● QUIZ PAGE f How has cART changed HIV-associated kidney diseases? The advent of cART has changed the pattern of kidney disease in patients with HIV infection, decreasing the incidence of AKI related to infection and HIV-associated nephropathy, but increasing nephrotoxicity related to antiretroviral therapy.4 Mechanisms of that nephrotoxicity include myoglobinuria, direct tubular toxicity, acute interstitial nephritis, and crystal nephropathy.5 Intratubular kidney precipitation of medications can promote acute and chronic kidney injury, termed crystal nephropathy (Box 2).6,7 Patients with HIV are commonly exposed to drugs that may promote intratubular crystal precipitation, but the real magnitude of this nephrotoxicity may be underestimated. xxviii Common non–HIV-specific causes Opportunistic infectionsa 〫 Kidney hypoperfusion and ischemia 〫 AIN 〫 Rhabdomyolysis b 〫 Urinary tract obstruction: blood clots, fungus balls, or crystalluria HIV-specific glomerulopathiesa Drugsc ● HIV-specific glomerulopathiesa 〫 HIV-associated nephropathy 〫 HIV immune-complex kidney disease Immune complex–mediated GN IgA nephritis Mixed sclerotic/inflammatory disease Lupus-like disease 〫 Thrombotic microangiopathy Common HIV-nonspecific glomerulopathiesb 〫 HCV-related MPGN/cryoglobulinemia 〫 Postinfectious GN 〫 Amyloidosis 〫 Membranous glomerulopathy 〫 Classic FSGS 〫 Diabetic nephropathy 〫 Minimal change disease 〫 IgA nephropathy Drugsc Fluid and Electrolyte Disorders ● ● ● Disorders of osmolality Potassium disorders Acid-base disorders Antiretroviral Nephrotoxicity ● ● ● ● ● ● ● ● AKI: abacavir, atazanavir, didanosine, indinavir, ritonavir, saquinavir, tenofovir CKD: abacavir, atazanavir, indinavir, lopinavir, tenofovir AIN: abacavir, atazanavir, indinavir Fanconi syndrome: tenofovir, didanosine, abacavir Renal tubular acidosis: lamivudine, stavudine Crystalluria, lithiasis: see Box 2 Nephrogenic diabetes insipidus: didanosine, tenofovir Others Abbreviations: AIN, acute interstitial nephritis; AKI, acute kidney injury; cART, combination antiretroviral therapy; CKD, chronic kidney disease; FSGS, focal segmental glomerulosclerosis; GN, glomerulonephritis; HCV, hepatitis C virus; HIV, human immunodeficiency virus; IgA, immunoglobulin A; MPGN, membranoproliferative glomerulonephritis. a Less common cause since cART introduction. b More common cause since cART introduction. c Including antiretroviral drugs listed in Antiretroviral Nephrotoxicity. Am J Kidney Dis. 2012;59(6):xxvii-xxx Box 2. Agents Associated With Crystal Nephropathy ● Antiretrovirals 〫 Atazanavir a 〫 Indinavir ● Antivirals a 〫 Acyclovir 〫 Foscarnet ● Antibiotics 〫 Ampicillin 〫 Cephalexin 〫 Ciprofloxacin a 〫 Sulfonamides ● Other drugs 〫 Aspirin a 〫 Methotrexate 〫 Oral sodium phosphate 〫 Piridoxylate 〫 Primidone 〫 Sulfa-containing medications a 〫 Trianterene 〫 Vitamin C 〫 Xylitol Note: HIV (human immunodeficiency virus)–positive patients are frequently exposed to multiple drugs that can precipitate into crystals. a Most commonly prescribed medications associated with crystal nephropathy. f How do you interpret the kidney biopsy? Am J Kidney Dis. 2012;59(6):xxvii-xxx length (Figs 5 and 6). Negative periodic acid–Schiff and von Kossa staining excludes polysaccharides and phosphate content, respectively. Immunofluorescence microscopy is negative. f What is the most likely cause of the progressive decrease in kidney function in this patient? Our patient presented with progressive chronic kidney disease. The absence of proteinuria/hematuria and the kidney biopsy excluded glomerulopathies. Although AKI may have a multitude of causes, the patient had neither opportunistic infections nor other non–HIV-related causes. The first episode was associated with tubular toxicity and improved after tenofovir withdrawal, making this drug a likely culprit.8 Crystalluria was not appreciated as a possible cause of the second AKI episode, and the cART regimen continued; however, this could have represented acute crystal nephropathy that later progressed to chronic disease. Crystal deposition likely was caused by atazanavir, the only drug taken by the patient known to be associated with urinary crystal formation. Urinary crystals disappeared after atazanavir withdrawal. It is likely that the nephrotoxic effect, first with tenofovir and then with atazanavir, significantly contributed to chronicity. Despite atazanavir withdrawal and a course of steroid therapy, Figure 5. Urinary sediment (original magnification, ⫻200). xxix QUIZ PAGE Light microscopy shows a glomerulus with mild nonspecific ischemic collapse and pericapsular fibrosis (Fig 2). There is diffuse and mild active interstitial infiltration by mononuclear cells, associated with giant cell reaction, surrounding numerous crystals distributed in the interstitium and within distal or collecting tubules (Figs 3 and 4). Crystals appear generally clear with characteristic serrated edges and are nonbirefringent upon polarization. Electron microscopy shows crystal-shaped clefts similar in outline to the crystals seen in the urinary sediment, with aggregations of fine needle crystals ranging in size from 150270 nm in diameter and reaching several micrometers in Figure 4. Periodic acid–Schiff stain (original magnification, ⫻400). 4. Roe J, Campbell LJ, Ibrahim F, Hendry BM, Post FA. HIV care and the incidence of acute renal failure. Clin Infect Dis. 2008;47: 242-249. 5. Izzedine H, Harris M, Perazella MA. The nephrotoxic effects of HAART. Nat Rev Nephrol. 2009;5: 563-573. 6. Izzedine H, Launay-Vacher V, Deray G. Antiviral drug–induced nephrotoxicity. Am J Kidney Dis. 2005;45:804-817. 7. Perazella MA. Crystal-induced acute renal failure. Am J Med. 1999; 106:459-465. 8. Fernandez-Fernandez B, Montoya-Ferrer A, Sanz AB, et al. Tenofovir nephrotoxicity: 2011 update. AIDS Res Treat. 2011;2011:354908. Figure 6. Electron microscopy (original magnification, ⫻3,000). the patient did not recover kidney function, and long-term hemodialysis therapy was started. A timely diagnosis may have led to a better outcome. FINAL DIAGNOSIS Atazanavir crystal–induced nephropathy as a part of multifactorial end-stage renal disease. ACKNOWLEDGEMENTS QUIZ PAGE Ana Isabel Silva, Luis Inchaustegui, Bruno Rodrigues, and Pedro Fidalgo are gratefully acknowledged. xxx REFERENCES 1. Fine DM, Perazella MA, Lucas GM, Atta MG. Kidney biopsy in HIV: beyond HIV-associated nephropathy. Am J Kidney Dis. 2008;51:504-514. 2. Franceschini N, Napravnik S, Eron JJ Jr, Szczech LA, Finn WF. Incidence and etiology of acute renal failure among ambulatory HIV-infected patients. Kidney Int. 2005;67: 1526-1531. 3. Flandre P, Pugliese P, Cuzin L, et al. Risk factors of chronic kidney disease in HIV-infected patients. Clin J Am Soc Nephrol. 2011;6: 1700-1707. CASE PROVIDED AND AUTHORED BY Silvia Coelho, MD,1 Samuel Rodrigues Aparicio, MD,2 Rita Manso, MD,2 and Karina Soto, MD, PhD,1 Departments of 1Nephrology and 2Pathology, Hospital Fernando Fonseca, Lisbon, Portugal. Address correspondence to Karina Soto, MD, PhD, IC 19, Hospital Fernando Fonseca EPE, 2720276 Amadora, Lisboa, Portugal. E-mail: ksoto.nefro@gmail.com © 2012 by the National Kidney Foundation, Inc. http://dx.doi.org/10.1053/j.ajkd. 2012.03.005 SUPPORT: None. FINANCIAL DISCLOSURE: The authors declare that they have no relevant financial interests. Am J Kidney Dis. 2012;59(6):xxvii-xxx