ACP Meeting - American College of Physicians
advertisement

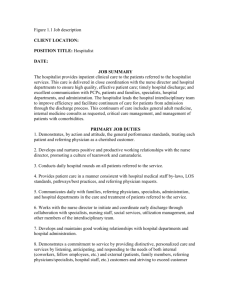
11/17/2013 Hospitalist Roles ACP Meeting Christopher Gamble, MD, FACP Associate Medical Director Hospitalist Program IU Health Ball Memorial Hospital Leader of the Medical Team Multi-disciplinary Rounds Documenting, Rounding, Communicating, Facilitating, Consulting Co-Management Education Medical Student Resident November 15, 2013 Leader of the Medical Team Quality Improvement Core Measures Mortality, LOS, Pt Satisfaction Readmissions Management Transitions of Care Pre-operative Evaluation Transition Clinic LTAC SNF Hospitalist Co-Management "We always cover the ears of the patient whenever we need to ask the nurse how to do something." Definition - shared responsibility, authority and accountability for the care of a hospitalized patient across clinical specialties “While there are opportunities for hospitalists to add real value as co-managers of surgical patients (e.g. in optimizing the medical care of patients with significant co-morbidities such as heart failure and diabetes, and reducing post operative complications such as venous thromboembolism), the general definition of comanagement is vague and varies markedly from one hospital to another.” SHM – A White Paper on a Guide to Hospitalist/Orthopedic Surgery Co Management *ACP Cartoon Sept 2009 Co-Management Medicine • Cardiology • Oncology • Hospice/Palliative Care • Endocrinology • Nephrology • Neurology Surgical • Orthopedics • General Surgery • Urology • ENT Co-Management The Classic Question for Physicians??? 1 11/17/2013 Co-Management The Classic Question for Physicians??? Co-Management Who is admitting and who is consulting? What the surgeon says: “I need your help managing the medical issues” Co-Management What the hospitalist hears: “I need you to do the discharge summary” Benefits of Co-Management Increased prescribing of evidence-based treatments Reduced time to surgery Fewer transfers to an ICU for acute medical deterioration Lower post-operative complications Increased likelihood of discharge to home Reduced length of stay Improved nurse and surgeon satisfaction Lower readmission rates Arch Intern Med. 2010 February 22; 170(4): 363–368. Comanagement of hospitalized surgical patients by medicine physicians in the United States Gulshan Sharma, MD, MPH,1,2 Yong-Fang Kuo, PhD,1,2 Jean Freeman, PhD,1,2 Dong D. Zhang, PhD,1,2 and James S. Goodwin, MD1,2 Comanagement of geriatric patients with hip fractures: a retrospective, controlled, cohort study. Implementation of a comanagement protocol for care of geriatric patients with hip fracture: Admission to a geriatric primary care service Standardized perioperative assessment regimens Expeditious surgical treatment Continued primary geriatric care postoperatively Results: Reductions in lengths of stay, ICU admissions, and hospital costs per patient Geriatr Orthop Surg Rehabil. 2013 Mar;4(1):10-5. doi: 10.1177/2151458513495238. Comanagement of geriatric patients with hip fractures: a retrospective, controlled, cohort study.Della Rocca GJ, Moylan KC, Crist BD, Volgas DA, Stannard JP, Mehr DR.Department of Orthopaedic Surgery, University of Missouri, Columbia, MO, USA. 2 11/17/2013 Medical and surgical comgmt after elective hip and knee arthroplasty: a randomized, controlled trial Issues with Co-Management Inconsistent definition from hospital to hospital Increases demand for hospitalists and with it a critical and potentially destabilizing hospitalist manpower shortage INTERVENTIONS: A comgmt Hospitalist-Orthopedic Team compared with standard postoperative care by orthopedic surgeons with medical consultation. RESULTS: Facilitates surgeon/specialist disengagement Hospitalist career dissatisfaction and burnout Unclear delineation of responsibilities places patient at risk for conflicting/contradictory orders J Hosp Med. 2008 Sep;3(5):398-402. doi: 10.1002/jhm.361.Just because you can, doesn't mean that you should: A call for the rational application of hospitalist comanagement. Siegal EM.University of Wisconsin School of Medicine and Public Health, Madison, WI, USA. CONCLUSIONS: The comanagement medical Hospitalist-Orthopedic Team model reduced minor postoperative complication rates with no statistically significant difference in length of stay or cost. The nurses and surgeons strongly preferred the comanagement hospitalist model. Additional research on the clinical and economic impact of the hospitalist model in other surgical populations is warranted. Ann Intern Med. 2004 Jul 6;141(1):28-38. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Huddleston JM, Long KH, Naessens JM, Vanness D, Larson D, Trousdale R, Plevak M, Cabanela M, Ilstrup D, Wachter RM; Hospitalist-Orthopedic Team Trial Investigators. Mayo Clinic College of Medicine, Rochester, Minnesota 55905, USA. huddleston.jeanne@mayo.edu Opportunity missed: medical consultation, resource use, and quality of care of patients undergoing major surgery. Co-Management METHODS: Observational cohort of patients undergoing surgery at a university-based hospital. The outcomes included costs, hospital los, use of preventive therapies (such as perioperative beta-blockers) and clinical outcomes. RESULTS: Consulted patients were of a similar age, sex, and race, but more frequently had an American Society of Anesthesiologists score of 4 or higher (34.2% vs 13.0%; P < .001), diabetes mellitus (29.1% vs 16.1%; P < .001), vascular disease (35.0% vs 10.6%; P < .01), or chronic renal failure (23.9% vs 5.6%; P < .001). Patients were just as likely to: Have a serum glucose level of less than 200 mg/dL (<11.1 mmol/L) Receive perioperative beta-blockers Receive venous thromboembolism prophylaxis. Consulted patients had a longer adjusted length of stay (12.98% longer; 95% confidence interval, 1.61%-25.61%) and higher adjusted costs (24.36% higher; 95% confidence interval, 13.54%-36.34%). More patients in the hospitalist group were discharged from the hospital with no complications (61.6% vs. 49.8%; difference, 11.8 percentage points [95% CI, 2.8 to 20.7 percentage points]) Fewer minor complications were observed among hospitalist patients (30.2% vs. 44.3%; difference, -14.1 percentage points [CI, -22.7 to -5.3 percentage points]) Observed length of stay was not statistically different between treatment groups. However, when adjusted for discharge delays, mean length of stay for patients in the hospitalist model of care was shorter (5.1 days vs. 5.6 days; difference, -0.5 day [CI, -0.8 to -0.1 day]). Total costs did not differ between groups. Orthopedic surgeons and nurses preferred the hospitalist model. The question isn’t if Hospitalists should or should not provide surgical comanagement but with how, with what patients, and with what goals? CONCLUSIONS: Patients who had a consultation from a generalist did not receive different quality of care, but had costs and length of stay similar to nonconsulted patients. Perioperative internal medicine consultation produces inconsistent effects on efficiency and quality of care in surgical patients. Modifying the consultative model may represent an opportunity to improve care. Auerbach AD,Rasic, MA,Sehgal N,Ide B,Stone B,Maselli J. Opportunity missed: medical consultation, resource use, and quality of care of patients undergoing major surgery. Arch Intern Med. 2007; 167(21): 2338–2344. Hospitalist Co-Management Building Co-Management What is administration’s expectations? One service at a time Ortho’s different from Gen Surg which is different than Urology Define the population of patients that will benefit ASA Guidelines Low, moderate, high risk SHM – A White Paper on a Guide to Hospitalist/Orthopedic Surgery Co Management 3 11/17/2013 ASA Classification Hospitalist Co-Management Minimal evidence to support co-mgmt of uncomplicated surgical patients Moderate risk patients Mixed evidence on improving LOS and functional status High Risk Most convincing evidence that hospitalists improve outcomes, decrease complications Examples: Decompensated Heart Failure Acute COPD exacerbations Acute MI Acute CVA DKA Active Arrhythmias http://my.clevelandclinic.org/services/Anesthesia/hic_ASA_Physical_Classification_System.aspx Building Co-Management Put it in writing and stick to the script Miscommunication between providers increases risk to patient Define who manages what Common Questions that need addressed: Who manages: DVT prophylaxis? Pain? Activity? Wound care? Post op complications? Building Co-Management Conflict resolution Who does the nurse call for Fever? Hypotension? Low UOP? Medication Reconciliation – Admission and Discharge Discharge Summary Will there be a process for resolving issues or conflicts regarding the design or operation of the co-management program? Who will be responsible for providing authority when conflicts are unable to be resolved? Educate Hospitalists and Surgeons Nursing Staff Secretaries Administration References Marcantonio ER, Flacker JM, Wright RJ, Resnick NM. Reducing delirium after hip fracture: a randomized trial. J Am Geriatr Soc. 2001 May;49(5):516–22. Fisher AA, Davis MW, Rubenach SE, Sivakumaran S, Smith PN, Budge MM. Outcomes for older patients with hip fractures: the impact of orthopedic and geriatric medicine cocare. J Orthop Trauma. 2006 March;20(3):172–8. Phy MP, Vanness DJ, Melton LJ, III, et al. Effects of a hospitalist model on elderly patients with hip fracture. Arch Intern Med. 2005 April 11;165(7):796–801. Zuckerman JD, Sakales SR, Fabian DR, Frankel VH. Hip fractures in geriatric patients. Results of an interdisciplinary hospital care program. Clin Orthop Relat Res. 1992 January;(274):213–25. Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004 July 6;141(1):28–38. Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of a comanaged Geriatric Fracture Center on shortterm hip fracture outcomes. Arch Intern Med. 2009 October 12;169(18):1712–7 Zuckerman JD, Sakales SR, Fabian DR, Frankel VH. Hip fractures in geriatric patients. Results of an interdisciplinary hospital care program. Clin Orthop Relat Res. 1992 January;(274):213–25. Arch Intern Med. 2010 February 22; 170(4): 363–368. doi: 10.1001/archinternmed.2009.553 Comanagement of hospitalized surgical patients by medicine physicians in the United States Gulshan Sharma, MD, MPH,1,2 YongFang Kuo, PhD,1,2 Jean Freeman, PhD,1,2 Dong D. Zhang, PhD,1,2 and James S. Goodwin, MD 4 11/17/2013 References Anaesth Intensive Care. 2013 Sep;41(5):569-72. Medical co-management of high risk surgical patients. Story DA, Jones DA. SHM White Paper on Hospitalist Co-Mgmt Geriatr Orthop Surg Rehabil. 2013 Mar;4(1):10-5. doi: 10.1177/2151458513495238. Comanagement of geriatric patients with hip fractures: a retrospective, controlled, cohort study.Della Rocca GJ, Moylan KC, Crist BD, Volgas DA, Stannard JP, Mehr DR.Department of Orthopaedic Surgery, University of Missouri, Columbia, MO, USA. J Hosp Med. 2012 Oct;7(8):649-54. doi: 10.1002/jhm.1951. Epub 2012 Jul 12.Evolving practice of hospital medicine and its impact on hospital throughput and efficiencies. Chadaga SR, Maher MP, Maller N, Mancini D, Mascolo M, Sharma S, Anderson ML, Chu ES. Division of Hospital Medicine, Department of Medicine, Denver Health Medical Center, Denver, Colorado 80204-4507, USA. Arch Intern Med. 2010 Dec 13;170(22):2004-10. doi: 10.1001/archinternmed.2010.432. Comanagement of surgical patients between neurosurgeons and hospitalists. Auerbach AD, Wachter RM, Cheng HQ, Maselli J, McDermott M, Vittinghoff E, Berger MS. Division of Hospital Medicine, Department of Medicine, University of California, San Francisco, CA 94143-0131, USA. Ann Intern Med. 2004 Jul 6;141(1):28-38. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Huddleston JM, Long KH, Naessens JM, Vanness D, Larson D, Trousdale R, Plevak M, Cabanela M, Ilstrup D, Wachter RM; Hospitalist-Orthopedic Team Trial Investigators. Mayo Clinic College of Medicine, Rochester, Minnesota 55905, USA. 5