Chest Assessment and Auscultation
advertisement

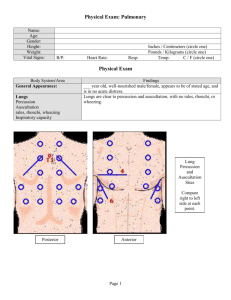
Clearing up the confusion about crackles, percussion, rhonchi in the bronchi and other lung assessment curiosities Dr Michal Boyd Nurse Practitioner/Sr Lecturer School of Nursing and Freemasons’ Dept. of Geriatric Medicine The University of Auckland Waitemata DHB 1 Use a systematic method Investigate - previous history, medications, labs & imaging Then Observe Palpate (feel) Percuss (tap) Auscultate (listen) Paint the clinical picture and make sure everything fits together! 2 Skin: During your assessment you notice that a patient's skin colour is pallid (pale). What might this indicate and why? If hypoxic (low in oxygen) the skin will appear pale as hypoxia causes vasoconstriction. Skin: Cyanosis Pneumothorax COPD Clubbing Lung cancer is the most common cause of clubbing. Clubbing often occurs in heart and lung diseases that reduce the amount of oxygen in the blood, such as: Heart defects that are present at birth (congenital) Chronic lung infections that occur in people with bronchiectasis, cystic fibrosis, or lung abscess Infection of the lining of the heart chambers and heart valves (infectious endocarditis), which can be caused by bacteria, fungi, or other infectious substances Lung disorders in which the deep lung tissues become swollen and then scarred (interstitial lung disease) Cardiac and Respiratory Assessment Anterior Thorax Posterior Thorax Anterior and Posterior Lung Lobes 9 Bronchial Segments Anterior View Lateral View Percussion & Auscultation Percussion and Auscultation Lung Auscultation and Percussion 14 What would percussion sound like? CHF What would percussion sound like? Emphysema Abnormal Respiratory Sounds Crackles (Rales) Rhonchi Medium Fine Late Inspiratory A coarse rattling sound somewhat like snoring, usually caused by secretion in a bronchial tube Wheeze Stridor Lung Consolidation Pneumonia Pleural Rub Question? A person is anxious and clammy with an obvious increase in work of breathing. Before reaching for the stethoscope you can hear this? What could cause this breath sound? swelling, a foreign body, or a tumour What would you do next? Documentation What does the person look like? SOB at rest, with exertion? Tripod Position? Has there been a significant change and if so, how long ago? Vitals – Respiration rate, Heart rate, temperature, blood pressure, Shortness of Breath Auscultation – what is heard, where is it heard and does it clear with cough? Lung Sounds Clear or abnormal? Is there a cough and is it productive – and if so how much and what does it look like? Pulse Oxymetry – above 90% How far can they walk Are they short of breath at rest? Crackles? Recent changes? Where is it heard on the chest? Inspiratory, Expiratory or both? Percussion Dull or hyperresonant? Auscultation distant, absent or normal? Where? Percussion – dullness? Where? A patient has fallen and fractured their ribs. A person has a sudden onset of shortness of breath with associated right-sided chest pain. The patient is clammy, hypotensive, and tachycardic. What could be the cause and what would you expect to hear on auscultation and percussion? Condition? pneumothorax Auscultation findings? Would be decreased/absent breath sounds in the right side of the chest with increased work of breathing. Percussion findings? Hyper-resonant Thoracic Expansion In Conclusion: Whenever I feel blue, I start breathing again. L. Frank Baum (Author of Wizard of Oz)