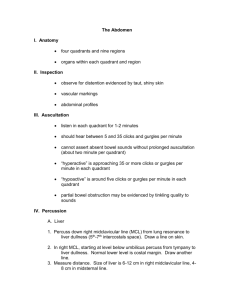
Percussion
advertisement

Percussion Dr. Laszlo Jakab Technique the pleximeter finger hyperextension of the middle finger of the left hand its DIP joint press firmly avoid contact by other part of the hand → → decrease of vibrations the plexor finger right middle finger→ partially flexed tip of the plexor finger strikes the pleximeter finger Technique transmission of vibrations → through the bones of DIP joint → to the underlying chest wall movement of the wrist thick chest wall → heavier percussion strike 2x in 1 location percussion → audible sounds ← motion of the chest wall Technique underlying tissues air-filled fluid-filled solid penetration → 5-7cm into the chest deep-seated lesions → undetected Medical percussion sounds NORMAL PERCUSSION SOUNDS Resonance: heard over lung tissue Tympany: heard over most portions of the abdominal cavity Dullness: heard over solid organs (eg, liver) and muscles ABNORMAL PERCUSSION SOUNDS Lung: dullness, which may be produced by pneumonia, tumor, infarction, or fluid collection; hyperresonance or even tympany, which may result from confluent air collection, as seen in pneumothorax or emphysema Abdomen: dullness, which may be produced by intra-abdominal tumors or masses; shifting dullness may indicate presence of ascites Heart: an expanded area of dullness may indicate cardiomegaly or pericardial effusion The Posterior Chest Percussion → compare one side with other symmetrical areas sitting position undress to the waist apex → base omit the scapular areas ← thick musculosceletal structures normal lung percussion → resonance → → intensity: loud, pitch: low, duration: long emphysema (lungs are hyperinflated) percussion → →diffuse hyperresonance → intensity: very loud, pitch: lower, duration: longer The Posterior Chest Abnormal dullness fluid in the pleural space = pleural effusion hemothorax (blood), empyema (pus) solid tissue in the lung → lobar pneumonia alveoli filled with fluid, RBC, WBC Unilateral hyperresonance large air-filled bulla in the lung or large amount of air in the pleural space The Posterior Chest Identification of the level of diaphagmatic dullnes percussion: apex → base resonance→ dullness = diaphragm abnormally high level→ diaphragmatic paralysis Diaphragmatic excursion distance between levels of dullness on full exspiration on full inspiration 5-6 cm Summary Normal case: percussion note → resonant tactile fremitus → normal Lobar pneumonia (bacterial infection, alveoli filled) percussion note → dull over the airless area tactile fremitus → increased Pleural effusion (fluid accumulates and separates the ai-filled lung from the chest wall and blocks the transmission of the sound) percussion note → dull over the fluid tactile fremitus → decreased The Posterior Chest Ptx air in the pleural space → blocks the transmission of the sounds percussion note → hyperresonant or tympanic over the pleural air tactile fremitus → decreased or absent over the pleural air The Anterior Chest supine position compare both sides dullness behind the right breast → right middle lobe pneumonia identification of the upper border of liver dullness The Heart supine position estimation of cardiac size percussion: lung resonance → cardiac dullness percuss for the right, left and upper border left border → LV right border → RA The Abdomen relaxed patient supine position full exposure warm hands stand on patient´s right side The Abdomen Orientation 4 quadrants percussion tympany predominates → gastric air bubble, gas in the GI tract dullnes → each side solid structures (liver, spleen) suprapubic area → distended bladder, enlarged uterus Traube's space Anatomical boundaries are: 1. Right : Lateral margin of left lobe of liver. 2. Left : Spleen. 3. Superior : Resonance of lung. 4. Inferior : Costal margin. Contents 1. Fundus of stomach (Hence percussion of Traubes area normally gives Tympanitic resonance). 2. Costo-phrenic recess of left pleura devoid of lungs. Causes of obliteration of Traubes space: 1. Full stomach. 2. Left sided Pleural effusion. 3.Splenomegaly. 4. Enlargment ofleft lobe of liver due to any etiology. 5. Dextrocardia. 6. Proloiferative growth in fundus of stomach. The Liver liver dullness vertical span = height in cm in the right midclavicular line lung resonance → upper border of liver dullness tympany → lower border of liver dullness increased span → enlarged liver =hepatomegaly decreased span → small liver liver dullness disappears → free air present below the diaphragm → sign of perforation The Spleen posterior to the midaxillary line splenic dullness → oval area surroundings pulmonary resonance abdominal tympany enlarged spleen = splenomegaly → large dull area Ascites protuberant abdomen ascites fluid → sinks with the gravity percussion → dullness outward → central tympanic area shifting dullnes patient turns onto one side → dullness shifts fluid wave impulse transmitted through the fluid