Do you have direct access to colonoscopy or flexi
advertisement

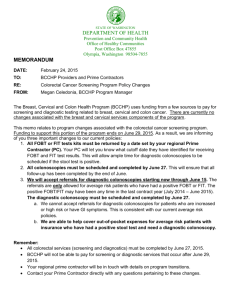
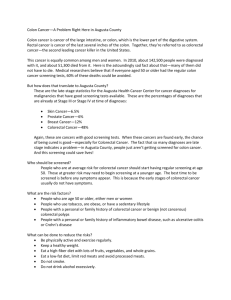
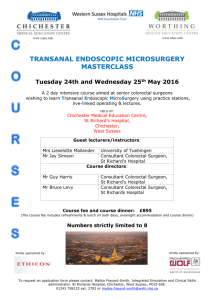
SW Colorectal Diagnostic Pathway Questionnaire Do you have direct access to colonoscopy or flexi-sigmoidoscopy? If you do what are the criteria? Answered: 13 Skipped: 1 Answer From Dropdown Colonoscopy Flexi-sigmoidos copy 0% 10% Yes 20% 30% 40% 50% 60% 70% 80% 90% 100% No Answer From Dropdown Yes Colonoscopy Flexi-sigmoidoscopy No 23.08% 3 76.92% 10 13 30.77% 4 69.23% 9 13 # If you do what are the criteria 1 No – but are staring work to introduce a straight-to-test colonoscopy pathway for colorectal cancer 2 week wait referrals in 2015 2 Not to colonoscopy. At present looking at direct access. All pts go through 2WW clinic consultant appt. Designated 2WW clinic weekly 3 Plan for Cons is triage 2WW referrals then book direct to colonoscopy, CT colonoscopy 4 No - All 2WW are seen in clinic 1st and referred from clinic Gastroenterology straight to test but vetted 5 See attached sheet 6 Can change model but not at present 7 Starting 22nd Jan GPs will be able to book colonoscopy directly through ICE open net 8 OPA 9 Yes Direct to both Colonoscopy - Anaemia Flexi § - rectal bleeding 10 2WW - vetted / seen by consultant first in clinic Non 2WW Gastroenterology referrals straight to test - Both vetted 11 No Precious resource. Risk GP direct to test around activity / capacity Spent long time looking at triage to get it right. Booking system a challenge. Could in theory offer flexi if booking system allowed it 1 / 17 Total SW Colorectal Diagnostic Pathway Questionnaire Do you use nurse telephone preassessment? Answered: 13 Skipped: 1 Yes No 0% 10% 20% 30% 40% Answer Choices 50% 60% 70% 80% 90% 100% Responses Yes 30.77% 4 No 69.23% 9 Total 13 # Additional Comments 1 No – but may be part of the new pathway 2 Pre - Op endoscopy only. Bowel prep at OPD or posted 3 Yes for colonoscopy 4 No - Formal assessment in OPD by endoscopy nurse / staff Yes for non 2WW referrals 5 Endoscopy pre-assessment triage is built into the ICE open net 6 Although partly for 10% of colorectal referrals will be implementing fully nurse led assessment 7 Yes by endoscopy staff 2 / 17 SW Colorectal Diagnostic Pathway Questionnaire Do you have blood test results available prior to colonoscopy or flexisigmoidoscopy? Answered: 13 Skipped: 1 Yes No Other 0% 10% 20% 30% 40% Answer Choices 50% 60% 70% 80% 90% 100% Responses Yes 69.23% 9 No 15.38% 2 Other 15.38% 2 Total 13 # Comments 1 Only if indicated following assessment in clinic 2 Yes as pt has been through 2WW clinic 3 No delays - bloods done at OPA or P/A if needed CT colons - bloods not needed Colonoscopy - need renal function within 3/12 for contrast used in CT colon 4 Not routinely patients individualised 5 Sometimes Yes if for colonoscopy - On form (GP fills out half the time) 6 If GP has performed prior to OPA. Gone away from direct to test. All puts seen by Snr Reg at 2WW appt then 1wk to colonoscopy or plain CT 7 Available on ICE 8 Yes OPA 9 Yes for pts referred i.e. anaemia 10 Not routinely 11 via TAC 3 / 17 SW Colorectal Diagnostic Pathway Questionnaire What problems do you experience? E.g. Complications etc? Answered: 4 Skipped: 10 Do not attend Perforation Not suitable for... Poor bowel prep 0% 10% 20% 30% 40% 50% 60% 70% 80% Answer Choices 90% 100% Responses Do not attend 75.00% 3 Perforation 50.00% 2 Not suitable for investigation when on couch 25.00% 1 Poor bowel prep 100.00% 4 Total Respondents: 4 # Other (please specify) and add any further information 1 I cannot give precise figures – I am sure our endoscopy unit can. 2 Low problems experienced as patients already been seen in clinic 3 Perforation due to underlying co-morbidities DNA Bowel prep not taken 4 radiology travelling cross-side Admin error re prep IP Cancellations - Bed capacity 5 Inappropriate referrals DNA 5-10% FS conversions to BE / CT / Colon (c 30%) 6 Gone away from direct to test. All puts seen by Snr Reg at 2WW appt then 1wk to colonoscopy or plain CT. Bowel prep is full seen at 2WW apt so low problems 7 We have a robust nurse and booking office contact with patient. Texting patient introduced to advise further 8 Admin burden. Check with endoscopy. 9 Awaiting accuracy of referral at present -? Whether they are having appropriate test 10 Equity of service across all colorectal puts not just 2WW 11 Admin error - wrong prep or investigation 12 very low due to nurse pre-assessment 4 / 17 SW Colorectal Diagnostic Pathway Questionnaire What would you like to be doing that you are not currently doing? Answered: 13 Skipped: 1 # Responses 1 Straight-to-test colonoscopy (and CT colonography) for colorectal cancer two-week wait referrals in a safe and efficient process. 2 Implement new colorectal diagnostic pathway plan but this was blocked by Trust Board 3 STT 4 Straight to test Tele at 2WW OPA for st to test pts Roll out new pathway for all referrals 5 Booking / Identifying dedicated radiology tests 6 Straight to colon / CT colon Straight to colonoscopy for more cases i.e. Change in bowel habit Telephone preassessment for colonography 7 More direct to test for suitable patients Flexi- Sigmoidoscopy PR bleeding 45 upwards Cant afford unecessary colonoscopy 8 New pathway as discussed today 9 Reduce mean time to treatment Have reduced pathway by reducing time to 1st test by reducing 2WW apt down to 10days. Reflected through system. 10 Investigating all pts with an appropriate CIBH with a colonoscopy 11 Offering equity of service across all patients 12 Pressure time wise on investigations - Appropriateness 13 All referrals using same pathway 5 / 17 SW Colorectal Diagnostic Pathway Questionnaire If you would like to make a change does your local environment support this? Answered: 11 Skipped: 3 Yes No Other 0% 10% 20% 30% 40% Answer Choices 50% 60% 70% 80% 90% 100% Responses Yes 81.82% 9 No 9.09% 1 Other 9.09% 1 Total 11 # Further information 1 Yes – we are starting our first meeting between colorectal cancer services, endoscopy services and management team in January 2015. Our local CCGs are also encouraging this process. 2 Yes 3 CT colonoscopy - Capacity due to implode 12/12 need is develop peripheral hospitals with facilities to expand services i.e. NAH 4 Limited financial resources 5 Underway at present 6 Needs full colorectal team to discuss 6 / 17 SW Colorectal Diagnostic Pathway Questionnaire Do 2005 NICE 2 week wait referral guidelines for urgent referral need revising? - Have you already changed your referral guidelines? Answered: 10 Skipped: 4 Yes Do 2005 NICE 2 week wait referral guidelines for urgent referral need revising? Have you already changed your referral guidelines? No 80.00% 8 20.00% 2 10 33.33% 3 66.67% 6 9 # Comments 1 They are likely to be incorporated into the review of colorectal cancer management by NICE in June 2015. 2 Renewed last year 3 Local templates used but need revising 4 Yes need revising but not currently updated 5 Not yet - reviewing current NICE (2014) recommendations 6 Reviewing the early release of NICE 2015 we are in line with this 7 Guidelines need to be adhered to by primary care 8 Further follow up / info on GPs who persistently do not meet criteria 9 Needs revising 10 years + on 7 / 17 Total SW Colorectal Diagnostic Pathway Questionnaire Should we standardise direct access criteria? Answered: 13 Skipped: 1 Yes No Other 0% 10% 20% 30% 40% Answer Choices 50% 60% 70% 80% 90% 100% Responses Yes 61.54% 8 No 15.38% 2 Other 23.08% 3 Total 13 # Further Info 1 Difficult to answer – different patient populations, different capacity/demand pressures, different provision of services by CCGs or Trusts would make standardisation. That is why we see a variation in modality of primary tests for sympotomatic presentation of potential colorectal cancer (barium enema, colonoscopy, CT colonography) across the UK. 2 National Standards 3 We will present our 6th month outcome at the SSG 4 Standardis criteria 5 Professional responsibility, patient fit for test. Follow up and mapping of results etc 6 Direct access for GPs to flex + TAC 8 / 17 SW Colorectal Diagnostic Pathway Questionnaire Should we standardise the use of nurse telephone pre-assessment? Answered: 11 Skipped: 3 Yes No Other 0% 10% 20% 30% 40% Answer Choices 50% 60% 70% 80% 90% 100% Responses Yes 54.55% 6 No 9.09% 1 Other 36.36% 4 Total 11 # Further info 1 This is difficult – with most Trusts under severe financial strain – I do not believe any Trust is keen on recruitment at present. More specialist nurses trained in appropriate nurse telephone pre-assessment would be a positive move – but who will pay. 2 N/A 3 This service is currently not available 4 Yes + local guidelines 5 As discussed today 6 Might be a good idea 7 Standardised new process 8 Need to ask endoscopy 9 This is standardised 9 / 17 SW Colorectal Diagnostic Pathway Questionnaire Could direct access to CT colonography be introduced? If Yes what would be the criteria Answered: 11 Skipped: 3 Yes No 0% 10% 20% 30% 40% Answer Choices 50% 60% 70% 80% 90% 100% Responses Yes 54.55% 6 No 45.45% 5 Total 11 # Criteria / Further Info 1 Those patients unsuitable for colonoscopy but able to manage CT colonography. 2 Capacity issues Failed colonoscopy Someone unfit for colonoscopy 3 Not at present 4 Yes but needs robust criteria / Consultant advice and guidance first. National Guidance 5 No - Limited resources mean the wait is currently too long. The resource has a potential to be swamped 6 Colon criteria - Unfit or technically not suitable for colon 7 Full bowel prep no difference. However biggest block in pathway is radiology service / resources 8 CT have 1 free appt per day (so can get in on same day (same prep) if failed / needed 9 We already use this - CIBH 10 No not without risk. Booking criteria important needs standardising including clinical context and "feel" for patient 11 Need consultant input (following up) Still need histology 12 GP risk not enough understanding. Specialist guidance don't do this often enough. 10 / 17 SW Colorectal Diagnostic Pathway Questionnaire What would be the wait time? Answered: 7 Skipped: 7 0 - 7 days 7 - 14 days 14 - 21 days 21 - 28 days 28 days + 0% 10% 20% 30% 40% Answer Choices 50% 60% 70% 80% 90% 100% Responses 0 - 7 days 14.29% 1 7 - 14 days 71.43% 5 14 - 21 days 14.29% 1 21 - 28 days 0.00% 0 28 days + 0.00% 0 Total 7 # Further info 1 Hopefully within 7 days of request. 2 2WW = 2/52 Urgent = 4/52 Routine = 6/52 As currently in place 3 2/52 4 Barren time practically waiting for service. Ideally need to see the right people at the right time. Difficult in current climate 5 10 days 6 2/52 11 / 17 SW Colorectal Diagnostic Pathway Questionnaire What information would be needed to make Advice & Guidance work? Answered: 11 Skipped: 3 # Responses 1 How can Advice and Guidance work? I assume you mean GP talking to colorectal surgeon. I am not sure how my colleague’s job plans could be changed to provide time in our contracts to support this. 2 Education 3 Regular interactivity / meetings between hospital clinicians and GPs 4 GP care enquiries regarding pts not currently in pathway or known to specialty Good coms on local services 5 Timings of wait for test Expectations re results What happens next Expectations of test / team 6 Rota for surgeons to provide this 7 Why waste time on advice and guidance when could go straight to test. Email system would work well with GP asking questions as would telephone. Who answers / consultants need to sleep / Could work as a regional service 8 N/A 9 Communication between hospital clinicians and GPs. GPs adhering to criteria 10 Critical - Needs time spent on the question 11 At present consultants spending 5hrs per week making this work. GP written comms 12 / 17 SW Colorectal Diagnostic Pathway Questionnaire Is written Advice & Guidance sufficient or would telephone advice be a useful and practical addition? Answered: 8 Skipped: 6 Yes No 87.50% 7 12.50% 1 8 100.00% 7 0.00% 0 7 Written Advice and Guidance sufficient Telephone Advice and Guidance useful Total # Comments 1 We can certainly do some work around written guidance, but my experience of talking with GPs over colorectal cancer management, is that a GP makes about 4 colorectal cancer 2 week wait referrals a year (a part time GP less). Will they remember how to find the guidance when they need it? Most GPs I have met seem to want the secondary care provider ‘sort it all out’. 2 Both 3 Telephone advice may be helpful in borderline / doubtful cases 4 Both 5 Currently being updated 6 Yes - both 7 Could work well regionally 8 N/A 9 For system to work GPs need to refer appropriatley 10 Telephone guidance may reduce the need for attendance / referral 11 New process timely OPA with nurse 12 As above 13 Needs to be tariffed into plan to make this effective otherwise challenge to making this work 13 / 17 SW Colorectal Diagnostic Pathway Questionnaire Would we be comfortable with patients who meet the NICE 2week wait criteria being seen in a more than 2 weeks? Answered: 11 Skipped: 3 Yes No Other 0% 10% 20% 30% 40% Answer Choices 50% 60% 70% 80% 90% 100% Responses Yes 45.45% 5 No 36.36% 4 Other 18.18% 2 Total 11 # Other (please specify) 1 Origin of colorectal cancer referral does not influence short-term patient out-come. Colorectal Disease 2008; 10: 58-62. The association between referral source and outcome in patients with colorectal cancer. The Surgeon 2012; 11: 141-146. 2 Patient expectations and support. 2 weeks is a long time to wait as a patient when referred from GP to hospital 3 No - Impact in achieving 62 day target in current pathway Also need to consider pt experience in delaying start of pathway following referral 4 If an appropriate scoring system was in place 5 No to avoid advanced cancers being delayed in treatment 6 With local agreement only 7 Practically difficult. How do we manage pt expectation. 8 N/A 9 2 weeks is a political timetable not based on any evidence so yes 10 Ensure all patients seen within 2weeks 11 Some pts are seen after 2wks if apps are changed - On whole the later the patient seen the later the treatment starts 12 2 wks to pre-assessment clinic then max another two weeks for all. All scoped less than 4wks 14 / 17 SW Colorectal Diagnostic Pathway Questionnaire If Yes, what would a reasonable timescale be in days? Answered: 2 Skipped: 12 14 - 21 21 - 28 28 - 35 35 - 42 42 - 49 49 - 56 56 - 63 63 + 0% 10% 20% 30% 40% Answer Choices 50% 60% 70% 80% 90% 100% Responses 14 - 21 100.00% 2 21 - 28 100.00% 2 28 - 35 0.00% 0 35 - 42 0.00% 0 42 - 49 0.00% 0 49 - 56 0.00% 0 56 - 63 0.00% 0 63 + 0.00% 0 Total Respondents: 2 # Comment 1 Too political an issue to comment. 2 1 week 3 Would need to book and implement referral template to triage all referrals akin to 2WW referrals Max 14 days should be aiming for 7 4 Depends on patient / symptoms 5 2weeks 6 N/A 15 / 17 SW Colorectal Diagnostic Pathway Questionnaire 7 The total wait rather than time to first appointment is more important- definitely< 3/12 8 Ensure all patients seen within 2weeks 9 Need full colorectal team input (following up) 16 I 17 SW Colorectal Diagnostic Pathway Questionnaire Would it be possible to set a revised timescale that meant the total wait for those diagnosed with cancer is reduced (by evening out waiting times and refining the pathway)? Answered: 11 Skipped: 3 Yes No Other 0% 10% 20% 30% 40% 50% Answer Choices 60% 70% 80% 90% 100% Responses Yes 81.82% 9 No 0.00% 0 Other 18.18% 2 Total 11 # Comments 1 Certainly straight to test might reduce the pathway time and thus treatment times for symptomatic patients diagnosed with colorectal cancer. 2 In ideal but pathways can be very complex at times 3 Increased diagnostics and staging is causing delays in treatment More pts having PET / CT / EBUS etc to make decisions on treatment plans Not just about kit but resources to support whole process - reporting times 4 Yes see the Seva score system 5 Possibly with the use of evening clinics and resources until 9pm 6 Not sure 7 Max 5 weeks from seeing GP. No real reason why those meeting 2WW criteria don't go straight to test. Of total Pts 25% Direct to test(bleeding right age group) 25% - (10%) Don't need to be in 2WW 50% is left maybe a third direct to test rest seeing more experienced dr / clinician 8 N/A 9 Would be dependent on individual units 10 If current proposals work pts seen in clinic within 2-3 days Current wait times endoscopy and imaging within 2 week window If multiple biopsy 15days 11 With diagnostics currently, difficult to see being able to reduce target times 12 Yes - See Harriet Watson TAC Model one model one pathway 17 / 17