Creative Solutions: A Case Study of Improving Health Care
advertisement

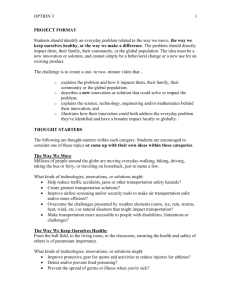
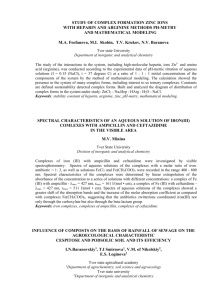
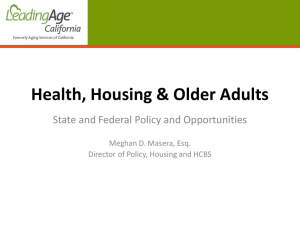
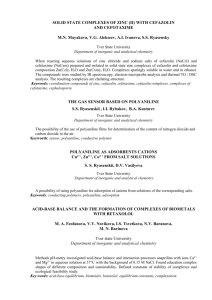
Creative Solutions: A Case Study of Improving Health Care in the Russian Federation M. Rashad Massoud, MD, MPH, FACP Director, USAID Applying Science to Strengthen and Improve Systems Project Senior Vice President and Quality and Performance Institute, University Research Co. LLC. Amanda Ottosson, MSc Healthcare Improvement Fellow, USAID Applying Science to Strengthen and Improve Systems Project Quality and Performance Institute, University Research Co. LLC. This work was done under the Quality Assurance Project implemented by University Research Co. LLC., funded by the United States Agency for International Development (USAID). INTRODUCTION This activity was born as a result of a shared vision to introduce modern improvement methods in order to improve quality of care and promote evidence based practices held by the US and Russian leadership of the Health Committee of the US-Russia Joint Commission for Economic and Technological Cooperation. The Russian Ministry of Health identified the Central Public Health Research Institute (CPHRI) in Moscow and Tula and Tver Departments of Health as the Russian implementation counterparts for the activity. The priorities for improvement were identified as maternal and child health (MCH), specifically in pregnancy-induced hypertension (PIH) and neonatal respiratory distress syndrome (NRDS) as well as primary care, specifically hypertension. In 1998, facilities representing the different levels and types of health care settings were initially chosen to participate in the improvement demonstration phase. The smallest number of facilities, which represented different levels of care were chosen. Five facilities were chosen for hypertension, three for pregnancy-induced hypertension, and five for neonatal respiratory distress syndrome. Results in the demonstration phase showed significant improvements in the care provided to patients, such as a reduction in early neonatal mortality for Tver Oblast 1 from 10.3 per 1,000 to 4.8 per 1,000; significant cost savings due to waste reduction, such as 87% reduction in the cost of care for pregnancy-induced hypertension, as well as behavioral changes amongst the team members at the leadership, team and individual levels. This case study outlines the methods and results of an effort to scale up efforts in improving health care in the Russian federation with limited funding through creative solutions. CASE PRESENTATION In 2000, based on the success of the demonstration phase, the project proposed to continue working for an additional two years, focusing on scale-up. The scale-up would include taking the PIH projects from the initial three facilities to 37, five initial facilities working on NRDS to 42 facilities and the hypertension work from five primary care facilities to 442 facilities. However the project was faced with some challenges. Unfortunately the project was not able to secure additional funding for scale up. This required the entire scale up plan to be reconsidered. The leadership of this effort had difficult decisions to make during this critical planning phase and came up with a creative solution to continuing the scale up efforts. The USAID Quality Assurance Project (QAP) in conjunction with the Health Departments of Tula and Tver Oblasts worked together to identify which areas of work could be covered by each group. The Health Departments covered all in-country costs of the learning sessions, food and travel. They decided they would use their own facilities to host learning sessions. Learning sessions were held in hospitals and other government owned facilities. This showed a new level of commitment and ownership, which proved to be extremely useful to achieving the results. The QAP team covered all costs for technical assistance. 1 Administrative region. MANAGEMENT AND OUTCOME The health authorities of both Tula and Tver Oblasts were committed to playing the leadership role in the scale up. It was agreed, that in order to enhance the chances of success in the scale up, it had to be led from within the health authority, with QAP helping them in the background. The demonstration phase had evolved champions in improvement and in the clinical topic areas. These are staff of the health authority facilities of Tula and Tver who had played important roles in the demonstration phase, and who became skilled in improvement and, or the clinical topic of the improvement. In the scale up they were selected to lead several teams each. To equip them in doing so, they were given training in adult training techniques, team facilitation and coaching as well as improvement methods and the clinical topic areas. During scale up, the facilities in each oblast were grouped into clusters which were called interregional centers. These were virtual centers but represented a grouping which was led by two champions from the original facilities, one in improvement and another in the topic, and who worked together on the improvement. These groupings were re-organized three times in the course of the work, a part of iteratively adjusting and improving the design of the scale up phase. The scale-up was organized as a series of steps, with specific activities happening at each of them and clear roles and responsibilities for the teams and the champions. It was decided that the teams will report on progress to the monthly meeting of the health authority. The champions were mentored throughout the scale up. Notably, the scale up required less site visits from the USA than the demonstration phase. The teams received their facilitation and mentorship primarily from the Tula and Tver champions and from the Chief of the Methodological Center for Quality at the CPHRI in Moscow. Discussion Although there was a lack of funding to scale-up, the work did not suffer. The methods used were essentially those for the demonstration phase combined with ideas from the Diffusion of Innovationsi, specifically the idea of “homophily”, which Everett M. Rogers describes as the interaction of people with similar backgrounds learning from one another. If there had been more funding available in the scale up, this scale up approach would not have been applied and perhaps country ownership and commitment would not have been at the same level. Due to the ownership exhibited by the Russian Federation the improvement efforts that originated in Tula and Tver Oblasts have continued and expanded further. Surprisingly, the results were better in the scale up phase, which are believed to have occurred for two reasons. First, QAP and the Russian Federation learned from the critical demonstration phase. They then applied that learning to the facilities included in the scale up phase and adapted as necessary. A second reason for success was the utilization of champions from the demonstration phase to pass on their learnings and techniques during learning sessions. This provided understanding and motivation through the scale up, leading to outstanding and most importantly sustainable results. The results can be seen below in the two graphs, which show percent of neonates with respiratory distress (RD) who died during the first week of life in the demonstration phase and scale up phase, respectively, in Tver Oblast. 35.0 29.2 30.0 25.0 20.0 20.0 18.2 18.2 16.0 10.0 16.7 15.6 12.5 15.0 14.8 14.3 12.5 9.5 10.7 13.3 5.0 4.3 0.0 10.0 5.7 7.4 4.5 3.6 4.5 5.1 3.3 3.1 3.4 2.8 0.0 9.1 8.9 6.9 6.3 4.0 5.6 Infant Mortality, Neonatal Mortality, Early Neonatal Mortality all Tver Oblast during the Scale up Phase, 1998-2003 Early Neonatal Mortality Neonatal Mortality Infant Mortality 25 DEATHS PER 1,000 Percentage of neonates with RD who died in first week of life Percent of neonates with RD who died in the first week of life during the Demonstration Phase. Five hospitals, Tver Oblast. 20 19.5 17.6 17 16.4 15 14.80 13.4 10 10.3 13.9 11.1 9.6 7.9 8.8 7.40 6.5 5 8.90 5 6.00 4.80 0 1998 1999 2000 2001 2002 2003 7.7 5.4 Questions 1. If funding is a constraint during a scale-up project, discuss the creative solutions that can be taken to continue spreading improvement efforts. (600 words i Everett M. Rogers. Diffusion of Innovations 5th Edition. Free Press 2003.