2 families of cholinoceptors
advertisement

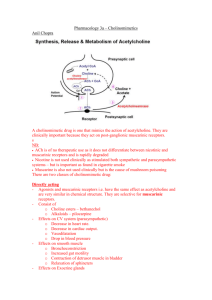
ACh serves as the synaptic transmitter at: CHOLINERGIC AND NEUROMUSCULAR PHARMACOLOGY 2 families of cholinoceptors muscarinic receptors nicotinic receptors Responses to cholinergic activation Subtypes and characteristic of muscarinic receptors Receptor subtype Other names Location Postreceptor Mechanism M1 M1a, neuronal Nerves, stomach IP3, DAG cascade M2 M2a, cardiac M2 Heart, nerves, smooth muscle cAMP, activation of K+channels M3 M2b, glandular M2 Glands, smooth muscle, endothelium IP3, DAG cascade all autonomic ganglia, SNS & PNS postganglionic parasympathetic nerve endings postganglionic SNS endings to sweat glands neuromuscular junction CNS Subtypes and characteristic of nicotinic receptors Recept or subtyp Ne M m4 ?CNS cAMP m5 ?CNS IP3, DAG cascade NN Other names Location Structural Postrec.m features echanism Muscle type, end plate receptor Skeletal Pentamer muscle (α2, β, γ, δ)2 Na+, K+ neuromuscu depolarizi lar junction ng Neuronal type, Postganglio α and β ion ganglion nic cell subunits channel receptor body, only as α 2 β dendrites 2 or α 3 β 3 1 Parasympathetic transmission Cholinergic drugs Directly acting cholinomimetics Drugs affecting the PS system Parasympathetic transmission path Drugs affecting the PS system ACh preganglionic neuron N ACh M Direct acting postganglionic neuron ganglion near target tissue Direct acting effector tissue or organ Cholinergic agonists (+) – TA: ophtalmology miosis intraocular pressure (glaucoma) Betanechol not hydrolyzed by AChE – TA: stimulation of atonic bladder postpartum/postoperational nonobstructive urinary retention – ADE: sweating, salivation, flushing, BP, nausea, abdominal pain, diarrhea, bronchospasm Muscarinic agonists (+) ACh-esterase inhibitors (+) Esters of choline Alkaloids Esters of choline Acetylcholine too unstable in plasma to be used as a drug Carbachol not hydrolyzed by AChE Cholinergic antagonists (-) Indirect acting Muscarine Pilocarpine – alkaloid, tertiary amine, not degraded by AChE – quick onset of action – TA: ophtalmology emergency and chronic lowering of intraocular pressure (IOP) in open-angle and closed-angle glaucoma – TA: xerostomia (that follows head and neck radiation TMTs or is associated with Sjorgen syndrome) Muscarinic antagonists (-) Indirect acting ACh-esterase inhibitors (+) Alkaloids Muscarinic agonists Pharmacokinetics Ach – rapidly destroyed Carbachol, bethanecol – not affected by the cholinoseterases longer duration of action Pilocarpine – well absorbed after p.o., s.c. or topical adm., access to CNS – ADE: • lipid soluble enters CNS disturbances • stimulates profuse sweating and salivaton 2 Muscarinic agonists Adverse effects SLUD, which is – – – – Salivation Lacrimation Urination Defecation Muscarinic agonists Major contraindications asthma ischaemic heart disease hyperthyroidism peptic ulcer AChE cleavage of ACh into Ch and acetate Ø of AChE ACh in synaptic space PS transmission (both M and N receptors) Types: – reversible (therapeutic) – irreversible (toxic, therapeutic) Drugs affecting the PS system Direct acting Bronchospasm Hypotension Arrhythmias AChE inhibitors Indirectly acting cholinomimetics Muscarinic agonists (+) AChE inhibitors – reversible Edrophonium Physostigmine Neostigmine Piridostygmine Muscarinic antagonists (-) Indirect acting ACh-esterase inhibitors (+) AChE inhibitors – reversible Edrophonium – ultra-short duration of action (5-10-20 min) – TA: diagnostics of myasthenia gravis (myastenic crisis vs. cholinergic crisis) Physostigmine – tertiary amine substrate for AChE – – – – – A: 2-4 h PK: CNS penetration TA: intestinal and bladder motility in atony TA: glaucoma TA: atropine overdose 3 AChE inhibitors – reversible Neostigmine – more polar than physostigmine – doesn’t enter CNS – – – – A: 2-4 hours TA: atony TA: tubocurarine antidote TA: myasthenia gravis (autoimmune disease muscular weakness) AChE inhibitors – irreversible Echothiophate, isoflurophate Nerve gases – sarin, soman, tabun Insecticides – malathion, parathion, paraoxon Pyridostigmine – longer duration (3-6 h) – TA: myasthenia gravis AChE inhibitors - irreversible Echothiopate/Isoflurophate – TA: topically – chronic TMT of open-angle glaucoma – ADE: few after topical administration AChE inhibitors in Alzheimer Disease A: brain AChE, BuChE TA: Alzheimer Disease Tacrine – withdrawn (hepatotoxicity) Donepezil Galantamine Rivastigmine!! : BuChE>AchE, no metabolism, no tolerance Irreversible AChE inhibitors Organic phosphates – irreversibly bind to AChE – toxic after systemic application (toxic military gases, insecticides) – A: generalized cholinergic stimulation, paralysis of motor function (problems with breathing), convulsions, miosis • CNS: coma, respiratory depression, seizures • Muscarinic: nausea, vomiting, diarrhea, blurring of vision, sveating, salivation • Nicotinic: mscle twiching, fasciculations, weakness, flaccid paralysis – antidote cholinoesterase regenerator pralidoxime (PAM)reactivation of AChE ineffective after aging (loss of phosphonate alkyl group) – Atropine – having an anticholinergic action – Emesis, lavage, catharsis, charcoal Therapeutic use of AChE inhibitors Use TMT of glaucoma Drugs physostigmine echothiophate isoflurophate Diagnosis of myasthenia gravis edrophonium TMT of myasthenia gravis neostigmine pyridostygmine TMT of Alzheimer’s disease donepezil rivastigmine tacrine Reversal of nondepolarizing muscle relaxants edrophonium Neostigmine pyridostygmine 4 Therapeutic uses of cholinomimetics - SUMMARY Myasthenia gravis – TMT, diagnosis Reversal of nondepolarizing muscle relaxants Xerostomia Glaucoma Alzheimer’s disease Antidote for atropine poisoning Tubocurarine anidote Bladder atony GI disorders: postoperative abdominal Muscarinic antagonists Atropine - actions Atropine – Belladonna alkaloid – competitive M antagonist – A: mydriasis, cycloplegia – A: gastric and intestinal motility, antispasmodic (pirenzepine – M1 antagonist – better at HCl production), motility of urinary bladder – A: low dose bradycardia (blockade of inhibitory prejunctional neurons), high dose tachycardia (vagal blockade at the SA&AV nodes), dilution of cutaneous vasculature (reduction in BP) – A: blockade of salivary (xerostomia), sweat ( body temperature) and lacrimal glands, inhibits secretion in the pharynx, trachea and bronchi, relaxes bronchial smooth muscles, decrease airway resistance Muscarinic antagonists Drugs affecting the PS system Direct acting Muscarinic agonists (+) Muscarinic antagonists (-) Indirect acting ACh-esterase inhibitors (+) Muscarinic antagonists Atropine – therapeutic actions ophthalmologic diagnostics mydriasis (fundus examination – more often tropicamide, homatropine), cycloplegia (refractive errors measurement) antispasmodic agent (GI tract, bladder) antidote (penetrates CNS): insecticides (irreversible AChE inhibitors), mushroom poisoning (muscarine) antisecretory agent (respiratory tract; before surgery) Bradycardia GU – TMT of cramping and urgent bladder in mild cystitis Muscarinic receptor antagonists The naturally occurring alkaloids: atropine and scopolamine Semisynthetic derivatives of these alkaloids: hyoscine butylbromide Synthetic congeneres: homatropine, tropicamide,cyclopentolate, ipratropium, tiotropium Muscarinic antagonists Atropine – adverse effects dry mouth, blurred vision, „sandy eyes”, tachycardia, constipation, attack of glaucoma (elderly) restlessness, confusion, hallucinations, delirium high doses depression, collapse of circulatory and respiratory system death 5 Effects of atropine in relation to dose (Goodman & Gilman’s) DOSE (mg) (mnemonic device) EFFECTS Slight cardiac slowing; some dryness of mouth; inhibition (therapeutic of sweating 0,5 dose) 1 Definite dryness of mouth; thirst; acceleration of heart; sometimes preceded by slowing; mild dilation of pupils 2 Rapid heart rate; palpitation; marked dryness of mouth; dilated pupils; some blurring of near vision 5 All the above symptoms marked; difficulty in speaking and swallowing; restlessness and fatigue; headache, dry, hot skin; difficulty in micturion; reduced intestinal peristalsis 10 and more Above symptoms more marked; pulse rapid and weak; iris practically obliterated, vision blurred; skin flushed, hot, dry, and scarlet; ataxia, restlessnes, and excitement; hallucinations and delirium; coma Muscarinic antagonists (semisynthetic) Hyoscine butylbromide TA: relieve bladder or intestinal spasms Muscarinic antagonists Scopolamine Atropine poisioning Mad as a hatter. Blind as a bat. Dry as a bone. Red as a beet. Hot as a pistol. Muscarinic antagonists (synthetic) Homatropine, tropicamide, cyclopentolate: mydriasis: produce mydriasis and cycloplegia Mebeverine, TA: antispasmodic Propantheline, TA: antispasmodic, urinary incontinence, peptic ulcer disease and nervous stomach Ipratropium (aerosol, dry powder, nasal spray) – quarternary derivative of atropine – TA: asthma slow onset of action • first choice β2-adrenergic agonists – TA: COPD!! – ADE: none Scopolamine – Belladonna alkaloid – PK: longer duration of action than atropine, better CNS penetration – TA : anti-motion sickness – TA : blocks short-term memory (anesthetic procedures) – AE : sedation, predictable autonomic adverse effects with increase of dose Muscarinic antagonists used in Parkinson Disease Benztropine, trihexphenidyl, biperiden – – – – – MoA: antimuscarinic agents FK : penetrate to the CNS A: tremor TA: Parkinson’s ADE: mood changes, hallucinations, xerostomia, accomodation problems, GI tract and urinary bladder motility Oxitropium (aerosol): TA :COPD Tiotropium (aerosol): TA :COPD Glycopyrrolate – TA: marked antisialogogue action (long duration, potency relative to atropine 2:1) – TA: premedicant 6 Therapeutic uses of muscarinic antagonists Ophthalmology: examination of the retina and optic disc Respiratory tract – COPD, asthma GI, biliary and genitourinary tracts - antispasmodic action CNS – motion sickness – Parkinson’s Disease Anticholinergic Drugs Ganglionic blockers 1. Antimuscarinic drugs 2. Ganglionic blocking drugs 3. Neuromuscular blocking drugs Antidote to Anticholinesterase Antidote to poisoning by mushrooms containing muscarine Preanesthetic medication Cholinergic antagonists Muscarinic antagonists OF LIMITED CLINICAL APPLICATION: GI tract – once the most widely used drugs for the management of peptic ulcer CVS – AMI in patients whom excessive vagal tone causes sinus or nodal bradycardia Ganglionic blockers Nicotinic antagonists Competitive neuromuscular blockers Ganglionic blockers Ganglionic blockers Neuromuscular blockers Nicotine – small doses ganglionic excitation • heart rate, blood pressure • peristalsis and secretions • appetite – high doses ganglionic blockade • heart rate, blood pressure • activity of GI tract and bladder • neuromuscular blockade TA: aid smoking cessation by easing nicotine craving ADE: tolerance and dependance Trimethaphan – short acting – TA: IV infusion emergency lowering of blood pressure (pulmonary edema, dissecting aortic aneurysm) when other agents cannot be used (sodium nitroprusside + β-blocker treatment of choice for aortic dissection, IV nitroglycerine acute pulmonary edema) – TA: lowering of blood pressure in surgery Cholinergic antagonists Muscarinic antagonists Ganglionic blockers Cholinergic agonists Nicotinic antagonists Competitive (nondepolarizing) neuromuscular blockers Nicotinic agonists Noncompetitive (depolarizing) neuromuscular blockers 7 Neuromuscular blockers Block the nicotinic transmission at the neuromuscular end-plate – nondepolarizing classical antagonists of N receptors – depolarizing desensitization of N receptors Use of neuromuscular blockers Surgical relaxation Control of ventilation TMT of convulsions Nondepolarizing neuromuscular blockers Adverse drug effects Cardiovascular Effects Hyperkaliemia Increased Intraocular pressure Increased intragastric pressure Muscle pain Nondepolarizing neuromuscular blockers Classification Isoquinoline derivatives – – – – – – Tubocurarine Atracurium Cisatracurium Metocurine Mivacurium Doxacurium Nondepolarizing neuromuscular blockers Tubocurarine, … (-curium, -curonium, - Steroid derivatives - Pancuronium Vecuronium (liver) Pipecuronium Rocuronium (liver) curine) – action can be overcome by ACh concentration in synaptic gap (AChE inhibitors) – sensitivity: small muscles (face, eye) > fingers > libs, neck, trunk > intercostal muscles > diaphragm – TA: IV surgery relaxation of skeletal muscles – TA: mivacurium quick recovery (short surgical procedures) – ADE: muscle weakness, myopathy – ADE: histamine release (bronchoconstriction in asthmatics), ganglionic blockade, blood pressure Depolarizing neuromuscular agents Succinylcholine – Phase I: excitation fasciculations – Phase II: flaccid paralysis (desensitization) – short duration (degradation by AChE) and quick onset of action – TA: IV endotracheal intubation prior to surgery – TA: IV electroconvulsive shock treatment – ADE: malignant hyperthermia (with halothane) – ADE: apnea (genetically related deficiency of AChE) – ADE: muscle pain and stiffness (12 to 24 h later) 8