The Knee 21 (2014) 1018–1022
Contents lists available at ScienceDirect
The Knee
Radiodense ligament markers for radiographic evaluation of anterior
cruciate ligament reconstruction
Paul Borbas ⁎, Karl Wieser, Stefan Rahm, Sandro F. Fucentese, Peter P. Koch, Dominik C. Meyer
Balgrist University Hospital, Orthopaedic Department, Zurich, Switzerland
a r t i c l e
i n f o
Article history:
Received 5 January 2014
Received in revised form 2 May 2014
Accepted 5 July 2014
Keywords:
ACL rerupture
Graft failure
Soft tissue marker
ACL reconstruction
a b s t r a c t
Introduction: Early clinical and radiographic diagnosis of failed or loosened anterior cruciate ligament (ACL) reconstructions can be challenging. The aim of the present study is to retrospectively evaluate the use of radiologically visible markers in the ACL graft, serving as a potential diagnostic tool in ACL graft rupture and insufficiency.
Methods: Twenty patients were included in the study. ACL reconstruction was performed with use of a hamstring
autograft in hybrid fixation technique. The graft was marked with two radiodense suture knots, one at the tibial
and femoral tunnel openings. Radiographs were performed postoperatively, after 6 weeks and 12 months. Four
distances between markers and landmarks were measured in anteroposterior and three in lateral radiographic
views and the positional change between the timepoints of measurement was calculated.
Results: Measurements of the marker distances on radiographs showed an excellent interobserver reliability (κ = 0.97).
In two measured distal anteroposterior distances statistically significant changes could be detected between
6 weeks and 12 months postoperatively in one patient with MRI-documented ACL rerupture and in five patients
with ACL elongation defined as anteroposterior-translation with side-to-side difference of ≥3 mm measured
with a Rolimeter device. On lateral radiographs, marker distances were highly variable and did not correlate
with clinical ACL elongation.
Conclusion: The application of radiodense ACL graft markers is a straight-forward, non-expensive and potentially
useful diagnostic tool to identify the position of the transplant and for diagnosis of graft elongation or failure.
However, the method is sensitive to the radiological projection, which should be further studied and optimized.
© 2014 Elsevier B.V. All rights reserved.
1. Introduction
The anterior cruciate ligament (ACL) is the second most commonly
injured knee ligament and its reconstruction is among the most
frequently performed orthopaedic operations [1]. The success rate of
ACL reconstruction varies from 69% to 95%. However, clinical diagnosis
of reruptures can be difficult due to swelling, joint effusion and pain, especially in the early postoperative or posttraumatic period. Commonly,
standard anteroposterior (ap) and lateral knee radiographs are performed in patients after knee trauma and after ACL reconstruction.
However, although the proper positioning of the bone tunnels and fixation material may well be evaluated, the integrity of the ACL auto- or allograft cannot. Therefore the migration of radiodense markers that are
securely fixed within the graft material might be helpful in diagnosing
elongation or rerupture and, thus, insufficiency of the reconstructed ACL.
Several studies have addressed soft tissue markers in order to measure ACL graft lengthening or rotator cuff reconstruction failure [2–7].
⁎ Corresponding author at: Forchstrasse 340, 8008 Zurich, Switzerland. Tel.: +41 44
386 1111; fax: +41 44 386 1109.
E-mail address: paul.borbas@balgrist.ch (P. Borbas).
http://dx.doi.org/10.1016/j.knee.2014.07.003
0968-0160/© 2014 Elsevier B.V. All rights reserved.
All of these in vivo or in vitro studies used radiostereometric analysis
(RSA) to study relative motion in three dimensions. RSA is a well
established technique for monitoring migration of prostheses relative
to bone and also to detect soft tissue marker migration. However, practical use of RSA remains limited because the sophisticated radiological
systems required are not commonly available in a routine practice. To
the authors' knowledge, no prior study evaluated the use of intraligamentary ACL graft marking with standard radiographs in two planes
without RSA. We hypothesized that due to the well-defined direction of
the graft however the use of plain radiographs may be feasible with appropriate markers and measurement technique.
The aim of the present study was therefore to evaluate the use of
radiodense ACL graft marking by measuring postoperative marker migration over time and consequently, to establish a new diagnostic tool
for ACL graft rupture or insufficiency.
2. Materials and methods
Between September and December 2010 in 27 patients an ACL reconstruction was performed using a hamstring autograft marked with
radiodense sutures. Eight patients had an additional meniscal procedure
during surgery, either partial meniscectomy or meniscal repair. All
P. Borbas et al. / The Knee 21 (2014) 1018–1022
1019
surgical procedures were performed by the same two experienced orthopaedic surgeons.
All patients received on a regular basis clinical follow-ups after six
weeks, three, six and finally 12 months after ACL reconstruction. Standardized anteroposterior (ap) (with an extended knee) and lateral
(with 30° flexion) radiographs were performed postoperatively, after
six weeks and 12 months. At 12-month follow-up measurement of
anteroposterior translation in 30° knee flexion by using a Rolimeter
(Aircast Europe, Neubeuern, Germany) device and clinical examination
with IKDC (International Knee documentation committee) score was
performed.
2.1. Surgical technique
The pes anserinus was visualized through a three centimeter incision anteromedially at the proximal tibia. The semitendinosus tendon
was harvested with a tendon stripper and the length and thickness
were measured. If the length or diameter of the quadrupled
semitendinosus graft was not sufficient, gracilis tendon was harvested
as well and the graft consisted of doubled gracilis and doubled
semitendinosus tendon. Afterwards the grafts were prepared using a
nonabsorbable braided suture to hold both ends using baseball stitches
(FiberWire, Arthrex, Naples, FL, USA). Finally, two intra-ligamentary
metallic suture knots (stainless steel monofilament, USP No. 4–0,
Ethicon Inc., Somerville, NJ, USA), grasping approximately one to two
millimeters of tendon tissue were placed in the approximate center of
the graft. The positions were chosen such that the markers would be
at or close to the tibial and femoral openings of the bone tunnels,
resulting in a distance of about two centimeters between the knots.
Standard medial and lateral parapatellar arthroscopy portals were
used. The femoral tunnel was drilled first via the anteromedial portal. A
guide wire was placed with a guide system (Karl Storz, Tuttlingen,
Germany) at the femoral footprint of the ACL in the intercondylar notch
in a knee flexion of at least 100°. After overdrilling with a 4.5 mm drill,
the final femoral graft tunnel was created by a cannulated drill with a
diameter according to the prepared graft. Afterwards the tibial tunnel
was prepared by using a drillguide (Karl Storz, Tuttlingen, Germany)
targeted at the center of the tibial ACL footprint. Femoral fixation was
achieved using a flipping device on the cortical bone (Fliptack, Karl
Storz, Tuttlingen, Germany), combined with a resorbable interference
screw compressing a bone wedge to the transplant (Megafix, Karl Storz,
Tuttlingen, Germany). In the tibial tunnel the graft was secured with an
interference screw (Megafix, Karl Storz, Tuttlingen, Germany) with the
knee close to full extension. Additionally, the sutures of the tibial graft
side were again fixed on cortical bone using a small plate (Endotack,
Karl Storz, Tuttlingen, Germany) covering the bone tunnel.
Mobilisation was started the day after surgery with flexion limit of
120° and extension limit of 0° for six weeks. After six weeks free
range of motion was allowed. Weight bearing was limited to half body
weight on crutches in an extension brace for three weeks. Running
was permitted after three months, high-demand pivoting sport was
allowed after a minimum of six months postoperatively.
2.2. Marker distances and measurements
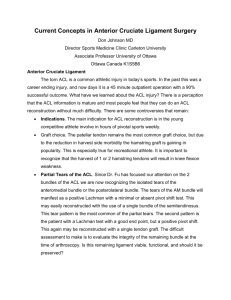
Seven radiographic marker distances were measured at three times
(postoperatively, after 6 weeks and after 12 months) by two independent observers. Of these, four marker distances were determined in
ap- (named “A1”–“A4”) and three marker distances were determined
in lateral X-rays (named “L1”–“L3”) (Fig. 1 a and b).
Changes of marker distances over time were calculated for all seven
distances and for all different time-points and named as ΔAa/ΔLa for the
difference from postoperative to 6 weeks and as ΔAb/ΔLb for the difference from 6 weeks to 12 months. Changes were detected in proximal or
distal directions and calculated as positive values no matter if the
distances increased or decreased (Fig. 2).
Fig. 1. a: Anteroposterior (ap) X-ray with four ap marker distances: A1: proximal fixation–
proximal marker; A2: proximal marker–distal marker; A3: distal marker–distal fixation;
A4: intercondylar eminence–distal marker. The center of the proximal fixation (Fliptack,
Karl Storz, Tuttlingen, Germany) and distal fixation (Endotack, Karl Storz, Tuttlingen,
Germany) device was used for measurements. b: Lateral X-ray with three lateral marker
distances: L1: proximal fixation–proximal marker; L2: proximal marker–distal marker;
and L3: distal marker–distal fixation.
2.3. Statistical analysis
Statistical analysis was performed using IBM SPSS® statistics software (version 20.0, Chicago, Illinois) by an independent biostatistician.
Interclass observer correlation between two independent observers
was measured. The intraclass correlation coefficient (κ) can have a
value between 0 (no agreement) and 1 (absolute agreement) and was
classified according to Fleiss as excellent if larger than 0.75. One-way
paired Student t test was performed to analyse differences of marker
distances between the time periods. Sub-groups of patients with aptranslation side–side difference of less than three millimeters and patients with side–side difference of minimum three millimeters were
built. Unpaired Student t test was performed to examine the data. pValues ≤ 0.05 were deemed to be statistically significant. Furthermore
a Pearson correlation analysis was performed to examine the association between clinical changes of ap-translation and radiological distance
changes.
3. Results
Of the 27 operated patients four emigrated within 12 months after surgery. Three patients did not show up for 12 months follow-up evaluation. One of them could not be
traced and two refused a followup visit, despite a favourable clinical outcome as verified
by telephone interview. All of these patients had to be excluded leading to a study
group of twenty patients. However, three of them had history of an ACL reconstruction
on the contralateral knee and were therefore excluded from the statistical analysis
concerning side-to-side differences. In one case the distal marker dislocated out of the
ACL graft. Therefore only the A1 distance could be calculated in this case.
1020
P. Borbas et al. / The Knee 21 (2014) 1018–1022
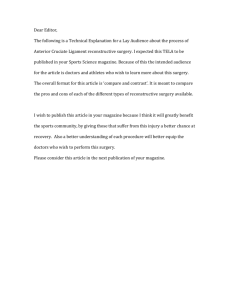
Fig. 2. Enlarged X-ray demonstrating a steel suture used as intra-ligamentary ACL graft
marker. The crossing points (marked with a cross) were used for measurements of marker
distances.
The measurements of the marker distances on X-rays showed an excellent interobserver reliability (κ = 0.97).
Of the remaining 17 patients, eleven (65%) had side-to-side differences of less than
three millimeters in ap translation and were defined as “normal ACL”. Six patients (35%)
with a side-to-side difference of three millimeters or more than three millimeters in
ap-translation were defined as patients with “ACL elongation/insufficiency”. One of
those six patients had an ACL re-rupture confirmed on MRI after a knee distortion during
football and finally underwent ACL re-reconstruction using a bone–patella–bone autograft.
However, the other five patients are having slight or no complaints and are willing to
proceed with conservative treatment.
Characteristics and differences between the groups are depicted in Table 1. Additional
procedures included partial meniscectomy or meniscal suture (n = eight) as well as
open-wedge high tibial osteotomy (n = three) for correction of a varus angulated knee
with signs of medial osteoarthritis. In five patients the procedure was a revision ACL reconstruction. As expected, increased ap-translation side–side difference of at least three millimeters was more likely in patients who underwent high tibial osteotomy for valgisation
and in patients who underwent ACL revision (re-reconstruction) because of failed ACL
reconstruction in the past.
In the subgroup with “ACL elongation/insufficiency” ΔA3b (p = 0.007) and ΔA4b
(p = 0.004) were significantly higher than in the control group without clinical signs of
ACL insufficiency (Fig. 3a,b). Similar changes could be seen as well on lateral radiographs.
However, those changes were not as clear and did not reach statistical significance.
At a ΔA4b cut off value of five millimeters a sensitivity of 100% and specificity of 72%
was reached for detecting side-to-side difference of three millimeters or more than three
millimeters in ap-translation.
The highest correlation was detected for ΔA4b (r = 0.47) and ΔA3b (r = 0.41).
4. Discussion
To objectively evaluate whether a reconstructed cruciate ligament is
intact, elongated or ruptured can be very challenging both clinically and
radiologically. Conventional radiographs are routinely performed after
ACL reconstructions, however the reconstructed ligaments are not
radiodense and thus invisible on radiographs. It appears therefore
attractive to mark the transplants with a radiodense suture marker in
order to see positional changes of the ligament relative to bone on
conventional radiographs, without the need for further sophisticated
radiological tools or methods.
We were able to confirm our hypothesis, that the application of
radiodense ACL graft markers has the potential to visualize the
position of the graft on conventional radiographs. We could detect
a significant correlation of clinical insufficiency and change of two
measured parameters, from the distal marker to the distal fixation
device (A3) and from the intercondylar eminence to the distal marker (A4) between six weeks and 12 months postoperatively. In three
of seven patients with clinical signs of ACL insufficiency the A3 and
A4 distances increased, whereas in four patients those distances
decreased. These results indicate that ACL graft elongation may
occur both proximal and distal to the opening of the tibial canal.
This is in certain contrast to the report of Van Eck et al., showing
that autografts tended to rupture or elongate mainly proximally
[8]. We have to state that in our data only one MRI-documented
ACL rerupture occurred (Fig. 4). In this case the failure area was
mid-substance with distal movement of the marker.
ACL graft markers have been used in vivo before, however in combination with RSA. Tantalum markers were inserted as beads into the
femur, the tibia and the graft for detection of three dimensional
micromotions [5], however with documented micromotion of the
beads within the graft. Roos et al. first used stainless steel sutures in
ACL graft marking, but only as cages for tantalum balls that were used
as RSA markers [7]. Cashman et al. finally used stainless steel sutures
as RSA markers in an in vitro study [4]. They showed that stainless
steel sutures were not as exact as tantalum beads when used as RSA
markers, but were still accurate within approximately 1 mm. The
same research group further published an in vivo study where they
used stainless steel sutures as soft tissue markers in reconstructed rotator cuff tendons for monitoring the behaviour of rotator cuff after repair
with RSA [3]. Even though RSA appears to be a very reliable experimental tool, due to the technical difficulties the application of RSA in a routine clinical practice to detect ACL graft rupture or insufficiency appears
not to be a realistic scenario.
This is to our best knowledge the first study that evaluates the use of
radiodense ACL graft marking with standard X-rays in two planes and
correlates these results with the clinical patients' outcome. We are
aware of the limitations of this preliminary report. The number of patients is limited and not fully homogeneous, as there were additionally
performed procedures such as high tibial osteotomy and there were a
considerable number of patients lost to follow-up. However, with the
available numbers and data, the technical aspects regarding the radiological projection are already well visible and additional surgical procedures should not have relevantly influenced this analysis. Furthermore,
due to the retrospective nature of the study there is no control group
with markers in intact ligaments. The implantation of the radiodense
markers was as expected a quick and simple surgical step, which did
Table 1
Illustration of patients and results of two groups divided by ap-translation side–side difference: The terms ΔA3b and ΔA4b are demonstrating the change of the measured distances between distal X-ray marker and distal fixation device (A3) and between intercondylar eminence and distal X-ray marker (A4) from 6 weeks to 12 months postoperatively on ap
radiographs.
Number (m:f)
Age (in years)
Mean side–side difference of ap-translation
Additional meniscal procedures
Additional valgisation osteotomy
Revision ACL reconstruction
Mean IKDC
Mean ΔA3b
Mean ΔA4b
ap-translation side–side difference b 3 mm
ap-translation side–side difference ≥ 3 mm
p
11 (9:2)
30 (20–48)
1.5 mm
5 (45%)
1 (9%)
2 (18%)
Normal–nearly normal
3,6 mm
3,8 mm
6 (4:2)
36 (18–55)
4.3 mm
3 (50%)
2 (33%)
3 (50%)
Nearly normal–abnormal
9.9 mm
10.4 mm
0.007
0.004
P. Borbas et al. / The Knee 21 (2014) 1018–1022
1021
Figs. 3. a, b: Illustrations of the statistically significant distance differences measured between distal X-ray marker and distal fixation device (A3) and between intercondylar eminence and
distal X-ray marker (A4) from 6 weeks to 12 months postoperatively on ap radiographs.
not increase surgical time in our hands. As a technical problem however,
in one patient an obvious distal marker dislocation was radiologically
detected, but without clinical instability and with no detectable associated clinical or radiological disadvantage.
Although we found encouraging results when analysing ap radiographs, in lateral radiographic measurements there was a large variation of the marker positions and a poor correlation with clinical ACL
lengthening. This effect was most pronounced in the images performed
immediately postoperatively without the use of fluoroscopy and is most
likely due to angular variations in the radiographic projection. The nature of this effect and how to address it will therefore further be
analysed in an on-going research project. From the current data we conclude so far, that strictly standardized radiographs are a prerequisite for
reliable results.
5. Conclusion
The application of radiodense ACL graft markers seems to be a
straight-forward, non-expensive and potentially useful diagnostic tool
to identify the position of the transplant and for diagnosis of ACL
graft elongation and insufficiency. However, there is still room for improvement of the optimal technique for reproducible radiologic
1022
P. Borbas et al. / The Knee 21 (2014) 1018–1022
imaging and therefore further gain of the diagnostic value of this
method.
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] Oh YH, Namkoong S, Strauss EJ, Ishak C, Hecker AT, Jazrawi LM, et al. Hybrid femoral
fixation of soft-tissue grafts in anterior cruciate ligament reconstruction using the
EndoButton CL and bioabsorbable interference screws: a biomechanical study.
Arthrosc 2006;22–11:1218–24.
[2] Ashmore AM, Rout R, Beard DJ, Price AJ, Murray DW, Gill HS. A new technique for the
radiostereometric analysis of soft tissues. J Biomech 2012;45–16:2931–4.
[3] Baring TK, Cashman PP, Reilly P, Emery RJ, Amis AA. Rotator cuff repair failure in vivo:
a radiostereometric measurement study. J Shoulder Elbow Surg 2011;20–8:1194–9.
[4] Cashman PM, Baring T, Reilly P, Emery RJ, Amis AA. Measurement of migration of soft
tissue by modified Roentgen stereophotogrammetric analysis (RSA): validation of a
new technique to monitor rotator cuff tears. J Med Eng Technol 2010;34–3:159–65.
[5] Khan R, Konyves A, Rama KR, Thomas R, Amis AA. RSA can measure ACL graft
stretching and migration: development of a new method. Clin Orthop Relat Res
2006;448:139–45.
[6] Roos PJ, Hull ML, Howell SM. Lengthening of double-looped tendon graft constructs in
three regions after cyclic loading: a study using Roentgen stereophotogrammetric
analysis. J Orthop Res 2004;22–4:839–46.
[7] Roos PJ, Hull ML, Howell SM. How cyclic loading affects the migration of radio-opaque
markers attached to tendon grafts using a new method: a study using roentgen
stereophotogrammetric analysis (RSA). J Biomech Eng 2004;126–1:62–9.
[8] van Eck CF, Kropf EJ, Romanowski JR, Lesniak BP, Tranovich MJ, van Dijk CN, et al.
Factors that influence the intra-articular rupture pattern of the ACL graft following
single-bundle reconstruction. Knee Surg Sports Traumatol Arthrosc 2011;19–8:1243–8.
Fig. 4. ap radiograph of a patient 6 weeks (left image) and 12 months (right image)
postoperatively. The patient had a MRI-documented ACL rerupture after a knee distortion
during football.