InjuryRisksFemale

Michelle Lubrano
Kinesiology
11/29/10
Injury Risks for the Female Athlete
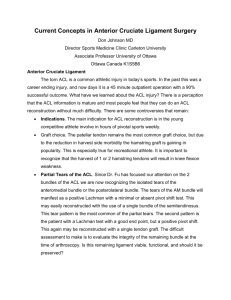
Women should be considered a different population in the study of exercise and athletics than men. The increasing number of women participating in sports also means that more women are likely to sustain injury. Women are more likely than men to sustain musculoskeletal injuries during physical activity. The most documented female injury in female athletics is the anterior cruciate ligament (ACL) tear. Studies show that ACL tears is 3 to 9 times higher for women than men. Soccer and basketball are the most common sports for ACL tears. Females are also at high risk for bone injuries being at least twice as likely as a male to experience a stress fracture.
Reasons that are suggested for greater risk of injury in women include biomechanics, weakness in local musculature, coordination and fatigue, and ligament and tendon properties.
Biomechanics is the most noticeable factor that causes injury. It includes jump landings and sideto-side movements. Women land with their knees less flexed and turned slightly more inward than men which increase risk of injury. This is known as the Q angle. These biomechanic factors also include females having a smaller and narrower intercondylar notch through which the ACL passes to attach the tibia. A smaller notch increases the risk of ACL impingement.
The risk of injury for women may also be related to joint flexibility. Women are more flexible and show greater joint laxity than men. Although flexibility can protect people from injury, joint laxity has been linked to increase incidence of injury. Lax joints may require increased muscle activity to provide support. However, the increase in muscle activation places more strain on surrounding ligaments. An example is muscle activity is gastrocnemius which
works together with the quadriceps and hamstrings to stabilize the knee joint. Joint laxity is known to be influenced by hormones which increase in women during the ovulatory or postovulatory phases of the menstrual cycle.
Female athletes are also more likely to develop a stress fracture. Studies on athletes and military recruits have reported risk 2 to 5 times that of men, and estimates of female athletes with stress fractures range from 4% to 58%. Females start with a lower bone mass and lose it more quickly than males which put them at a higher risk of developing osteoporosis. Approximately
30% of postmenopausal women have osteoporosis. Most stress fractures occur in the hip, spine, and wrist because they occur as a result of a fall from standing height or less, which causes extremely fragile bones. Items that play a role in the risk of fragility fractures are bone protein content, structure, geometry, and mechanical properties.
Overall women are prone to a lot of the same exercises as men such as patellofemoral pain syndrome, iliotibial band friction syndrome, medial tibial stress syndrome, Achilles tendonitis, ACL tears, plantar fasciitis, and lower extremity fractures. Both men and women can benefit from participating in the same preventive measures such as stretching, doing an effective warm-up and cool-down, specific strengthening, and conditioning exercises. There are also treatments available for men and women such as relative rest, icing, antiinflammatories, and physical therapy. However, for women it is important to focus on biomechanical, neuromuscular, and cellular mechanisms for injury risk.