The Arthritis Research Institute of America
advertisement

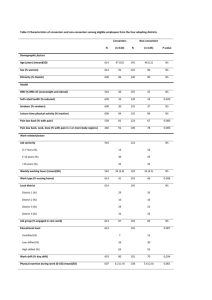
The Arthritis Research Institute of America 300 S. Duncan Ave, Suite 188 Clearwater, FL 33755 (727) 461-4054 October 27, 2008 Joseph Dunckley Assistant Editor BMC-series journals Re: MS 1838846535217525 Dear Mr. Dunckley, Thank you for your comments on our manuscript The association of BMI and knee pain among persons with radiographic knee osteoarthritis: A cross-sectional study. We did implement your suggestion to use a copy editing service. We also have provided a point by point response to all reviewers’ comments. The ‘Statistics’ paragraph has been re-written and several references added (17, 22 – 27) to address the concerns of the second reviewer regarding the Uniform Requirements. You will also notice minor changes to the Discussion and Conclusion sections. The copy editor caught a small error in that I had stated in the conclusion that we were the first to look at this relationship. Actually, we are the first to look at in this manner (risk ratios for each BMI category) but not the first to report results related to this question. I had referenced three papers in the Background that had looked at this question in some manner. I now mention this in the first part of the Discussion section and have removed reference to it in the Conclusions. Specific replies to reviewers’ comments are attached. Please let me know if anything further is required for this revised submission. Sincerely, Matthew W. Rogers, MS MS: 1838846535217525 The association of BMI and knee pain among persons with radiographic knee osteoarthritis: A cross-sectional study Matthew W Rogers and Frances Vaughn Wilder Reviewer: Max Reijman Reviewer's report: Major Compulsory revisions: The study population consisted of subjects with radiographic signs of knee OA, determined by the Kellgren & Lawrence criteria. (³ grade 2). As stated by the authors is knee pain related with radiographic severity. So the relation between knee pain status and BMI should also be adjusted for the severity of ROA of the knee. Absolutely. This factor was included in the adjusted model. The revised statistics now reflect the consideration of RKOA disease severity. Minor essential revisions: The authors reported that there is a positive linear relationship between the 4 categories of BMI and pain. Did the authors test for linearity? Another reviewer of this manuscript felt that linearity could be confusing in reporting our analyses. The text has been re-worded as follows: OLD: Unadjusted and adjusted odds ratios demonstrated a positive, linear association between BMI group and pain for each successive BMI category. REVISED: Unadjusted and adjusted odds ratios demonstrated a consistent, positive risk for pain for each successive BMI category. OLD: For the four BMI groups, a positive linear relationship with pain is demonstrated in the unadjusted and adjusted analyses REVISED: For successively higher BMI groups, a positive increase in the risk of pain is demonstrated in the unadjusted and adjusted analyses Footnote Table2: The adjusted odds ratio models should be: pain = bmi + age + gender (+ severity of ROA) The footnote now reads: BMI = Pain + age + gender + RKOA grade. Figure 2 presented similar results as Table 2, so one can be deleted. Only the old Table 2 (now Table 3) has been kept in the current revision. Reviewer: Annette W-Dahl Reviewer's report: 1. The main reason for major compulsory revision is the lack of description of the statistical methods used, with reference to the Uniform Requirements. It’s not possible to follow how the association of pain and BMI has been analyzed and thereby limited possibility to interpret the findings. Numerous changes have been made to our description of the statistical methods used. We reviewed the Uniform Requirements section on statistical methods shown below. “IV.A.6.c. Statistics Describe statistical methods with enough detail to enable a knowledgeable reader with access to the original data to verify the reported results. When possible, quantify findings and present them with appropriate indicators of measurement error or uncertainty (such as confidence intervals). Avoid relying solely on statistical hypothesis testing, such as the use of P values, which fails to convey important information about effect size. References for the design of the study and statistical methods should be to standard works when possible (with pages stated). Define statistical terms, abbreviations, and most symbols. Specify the computer software used.” The revised text below shows that we: Described in more details our general statistical approach; We noted our reporting of confidence internals for the odds ratios; We stated clearly our cross-sectional study design and provided a reference. Using our sample of subjects with RKOA, our cross-sectional study aimed to quantify the association between BMI and knee pain among subjects with radiographic evidence of knee OA; We added clarity to the statistical tests and concepts noted and referenced them in the text. This includes odds ratios, logistic regression, adjustment for confounding adjustment, and the kappa statistic; and We specified the computer software used, “SAS/STAT® software version 9.2 was used for all analyses.” “Frequencies, percentages, and means were calculated to provide descriptive data about our study sample. To estimate the strength of the association between BMI and knee pain, we computed odds ratios (OR) [Kleinbaum DG, Kupper, LL, and Morgenstern, H. Epidemiologic Research Principles and Quantitative Methods. John Wiley & Sons, New York 1982, pp243-250.] using logistic regression [DawsonSaunders B, Trapp, RG. Basic and Clinical Biostatistics, 2nd ed. Norwalk, CN: Appleton & Lange; 1994; 222-223; SAS Institute Inc., Logistic Regression Examples Using the SAS System, Version 6, First Edition, Cary, NC; SAS Institute Inc., 1995.] . Knee pain status (yes/no) was the outcome factor. With BMI as the exposure factor, subjects with normal BMI (18.5 to 24.9 kg/m2) served as the referent group for the analyses (e.g. Normal vs. Obese III). To address potential confounding when assessing the association between BMI and knee pain, we ran an adjusted statistical model (Pain = BMI + age + gender + RKOA grade). Logistic regression was used as we had a binary outcome and several explanatory factors (e.g. gender) in the statistical model [Walker, GA. Common Statistical Methods for Clinical Research with SAS® Examples Cary, NC: SAS Institute Inc. 1997, pp 225-226.]. Confidence internals were reported for the odds ratios. Every tenth subjects’ assembled radiographs were independently interpreted by a non-affiliated radiologist blinded to the results of the first reading. The inter-observer variability of x-ray interpretations was calculated using the kappa coefficient [20] measuring the amount of agreement that is above random chance. SAS/STAT® software version 9.2 was used for all analyses [SAS/STAT software, Version 9.2, SAS System for Windows. Copyright © 2008. SAS Institute Inc. Cary, NC, USA.].” a. The potential confounders, except age and gender, have only been described but not analyzed. We included the following information in the Results section, “Evaluation for potential confounding showed no significant differences, by Pain Group, for occupation (p=0.85), education (p=0.73), and self-reported disease status for diabetes (p=0.63), heart disease (p=0.53), nor stroke (p=0.37). Although the mean age was similar for each group, a significant group difference was evident for gender (p < 0.01). Based on preliminary analyses, as well as consideration of known factors related to OA, we built our adjusted model. BMI, age, gender, and disease severity (as measured by OA grade) were included in the final adjusted model. It might also be considered if there are other potential confounders that might be interesting and necessary. For example grade of radiographic knee OA might be interesting to include in the adjusted analyses. RKOA disease severity, as measured by grade, was a solid addition to the study. This factor was included in the adjusted model. The revised statistics now reflect the consideration of RKOA disease severity. The final adjusted model is: BMI = Pain + age + gender + RKOA grade. Disease status is not presented in table 1 or elsewhere. Further it would be informative to know how many of the patients in each BMI category who had pain and no pain respectively. Good point. This information has been added to the manuscript. Shown below, a new table was created to display these data. (Note previous Table 2 is now Table 3). Table 2 BMI Category and OA Grade counts, by pain status among subjects (N = 576) with radiographic knee osteoarthritis a Pain No Pain n (N=329) (N=247) Normal BMI b 155 66 89 Pre-Obese 208 113 95 Obese I 119 75 44 Obese II 61 47 14 Obese III 33 28 5 RKOA Grade 2 331 155 176 RKOA Grade 3 150 100 50 RKOA Grade 4 95 74 21 a Kellgren and Lawrence scale for radiographic osteoarthritis (Grades 2+). b BMI = body mass index (kg / m2) WHO Classification: Normal 18.5-24.9; Pre-Obese 25.0-29.9; Obese I 30.0-34.9; Obese II 35.0-39.9; and Obese III 40.0 +. b. My guess is that ¨Pain/No pain¨ has been used as dependent variable in the regression analysis and BMI category as independent variable as well as age and gender. However table 2 says; BMI=pain+age+gender it would then rather be Pain= BMI+age+gender. Our error. The footnote (for what is now Table 3) now reads: BMI = Pain + age + gender + RKOA grade. c. In the result part the authors write ¨a positive linear relationship with pain …..¨ .The analyses are paired comparison and not linear regression which make the statement that there is a linear relation not possible. The text has been re-worded as follows: OLD: Unadjusted and adjusted odds ratios demonstrated a positive, linear association between BMI group and pain for each successive BMI category. REVISED: Unadjusted and adjusted odds ratios demonstrated a consistent, positive risk for pain for each successive BMI category. OLD: For the four BMI groups, a positive linear relationship with pain is demonstrated in the unadjusted and adjusted analyses REVISED: For successively higher BMI groups, a positive increase in the risk of pain is demonstrated in the unadjusted and adjusted analyses 2. There is a lack of definition/description that makes the purpose of the study unclear. a. The use of the word ¨quantification¨ in the background of the abstract is confusing. Quantification has two distinct meanings, one in mathematics and empirical science and one in logic. Do the authors mean to quantify the association between pain and BMI among RKAO individuals as stated as the aim of the study by reporting the OR (is OR 1.6 an expression of quantifying the association between pain and BMI?). However transforming the continuous data of BMI to categorical data and analyze pain with categorical data become then confusing. The choice of words should be considered and well defined (major compulsory revision). Our goal was communicate to the reader as clearly as possible. The purpose of the study has been re-worded in the abstract and main text. In the main text it now reads, “Our current study will help clarify these findings by reporting odds ratios to further quantify the relationship between pain and BMI among persons with RKOA. Using our sample of subjects with RKOA, our cross-sectional study [Hennekens CH, Buring JE. Epidemiology in Medicine. Boston, MA and Toronto: Little, Brown and Co. 1987; 108-112.] aimed to quantify the association between BMI and knee pain among subjects with radiographic evidence of knee OA. “ b. The use of the term ¨ symptomatic¨ includes more than pain. Why not use the terms ¨pain¨ and ¨no pain¨ as it is pain that is of interest (minor essential revision). Good point, thank you. The terms have been changed to Pain and No Pain throughout the manuscript and tables. 3. The purpose of the study is not stated in the abstract (major compulsory revision). Purpose has been more clearly stated in the abstract as follows: The purpose of the study is to explore the relationship of BMI and knee pain among persons with RKOA. Old: As researchers seek a clear profile of which factors contribute to knee pain, quantification of the role of BMI is vital. 4. The background includes written errors and/or wrong use of words (minor essential revision). a. The cause of RKOA may be the cause of knee OA. For this revision, the manuscript was sent to a copy editing service. (Comment 4a appears to be a quoted typographical error, but we were not able to locate this phrase in our manuscript.) b. High-risk occupations of what? “High-risk occupations” has been changed to “certain occupations” (as described in the listed references; certain occupations have been linked to the development of OA) c. What is RKOA knee pain? Knee pain in individuals with RKOA? Wording has been changed to include RKOA related knee pain d. Considerations of the last sentence, page 3 ¨Subsequently ….¨ most patients seek medical care due to pain and disabilities not due to RKOA which makes the clinicians possibility to delay and prevent the onset of pain and impairment in these individuals unrealistic. Further, it’s only few of the patients with knee OA who need knee replacement, not ¨often¨ as written but rather in worse cases. Thank you, this is a good point. More realistically clinicians (e.g. physicians, physical therapists, fitness professionals) might counsel their overweight and obese patients on weight loss (as one example of a modifiable risk factor, and relevant to our study) to prevent or reduce knee pain. “Often” was changed to “may”. This text was modified as follows: As there is no cure for OA on the horizon, it is important to identify what factors influence the risk of symptomatic knee OA. Subsequently, clinicians could guide their patients to take steps (e.g., weight loss) to prevent or delay the onset of pain and impairments which may lead to work disability, daily living disability, and joint replacement surgery. e. In the background, the first part of page 4 includes partly author interpretations that are irrelevant to referred studies. The authors’ logical connection of BMI as a cause of knee OA becomes illogical when considers that even normal-weighted individuals suffer from knee OA and the authors may distinguish between cause and risk factor. Normal weight subjects report knee pain at lower rates vs. overweight and obese persons. This paragraph has been modified as follows: It is known that persons with higher body mass indexes (BMI; kg/m2) are more likely to report idiopathic knee pain and accompanying disability in comparison to persons with normal BMI [11-13]. This is suggestive of elevated BMI as a potential risk factor for knee pain among persons with RKOA. Despite this logical connection, a paucity of research has been conducted in this area. Further the present study has scanty any possibility to clarify the relationship between pain and BMI among patients with RKOA neither by reporting the OR for each BMI category in a cross-sectional study nor with the very narrow perspective used (major compulsory revision). Per your recommendations as noted in 1a, and those of another reviewer, these relationships have now been reported. The result, discussion and conclusion sections are difficult to interpret as the methods of statistics are scanty described as well as the purpose of the study is unclear. The authors have an excellent cohort and together with a clear defined research question, with a wider perspective of a systemic disease and appropriate, well described statistical methods the paper has the potential to be interesting and may contribute to increasing knowledge. These issues have been addressed and modified in response to reviewers’ comments. ******