Have you had any of the following within the last 6 months
advertisement

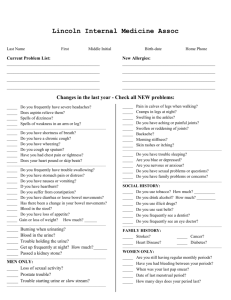
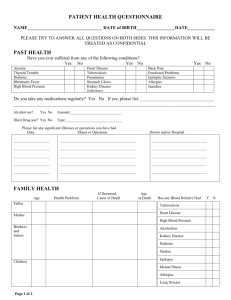
Have you had any of the following within the last 6 months? GENERAL Tire easily, weakness Marked weight change Night sweats Persistent fever YES YES YES YES NO NO NO NO SKIN Eruptions/rash Change in color Change in hair Change in nails YES YES YES YES NO NO NO NO EYES Trouble seeing Eye pain Inflamed eyes Double vision YES YES YES YES NO NO NO NO EARS Loss of hearing Ringing in ears Drainage YES YES YES NO NO NO NOSE Loss of smell Frequent colds Obstruction Excess drainage Nosebleeds YES YES YES YES YES NO NO NO NO NO MOUTH Sore gums Sore tongue Dental problems YES YES YES NO NO NO HEART/LUNGS Persistent cough YES Sputum (phlegm) YES Bloody sputum YES Wheezing YES Chest pain/discomfort YES Pain with breathing YES Shortness of breath YES Difficulty breathing while lying down YES Swelling of ankles YES Blue-tinged lips/nails YES High blood pressure YES Palpitations YES DIGESTIVE SYSTEM Change in appetite Difficulty swallowing Heartburn Abdominal distress Belching/excess gas Bloating Nausea Vomiting Vomiting of blood Rectal bleeding Tarry stools Dark urine Jaundice Constipation Diarrhea Hemorrhoids GENITOURINARY Urinary frequency Urinary urgency Unable to hold urine Pain or burning on urination Blood in urine Impotence Lack of sex drive Pain with intercourse YES YES YES NERVOUS SYSTEM NO Headaches YES NO NO Dizziness YES NO NO Fainting YES NO NO Convulsions YES NO NO Nervousness YES NO NO Sleeplessness YES NO NO Depression YES NO Change in sensation YES NO NO Numbness in fingers YES NO NO Numbness in toes YES NO NO Tingling in fingers YES NO NO Tingling in toes YES NO NO Memory loss YES NO Poor coordination YES NO Weakness/paralysis YES NO NO NO GYN/OB NO Age menstruation began ______ NO Date of last PAP_____________ NO Number of pregnancies _______ NO Number of miscarriages_______ NO Number of births_____________ NO NO MISC. NO Do you have any other concerns NO you would like the physician to NO be aware of? NO __________________________ NO __________________________ NO __________________________ NO __________________________ __________________________ __________________________ NO __________________________ NO __________________________ NO __________________________ YES YES YES YES YES NO NO NO NO NO YES YES YES YES YES YES NO NO NO NO NO NO YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES YES THROAT Postnasal drainage Soreness Hoarseness YES YES YES NO NO NO BREASTS Lumps Discharge YES YES NO NO ENDOCRINE Thyroid trouble Adrenal trouble Cortisone treatment Diabetes YES YES YES YES NO NO NO NO Patient Signature Date ________________________________________ ________________________________________ Physician Signature Date ________________________________________ ________________________________________ LOCOMOTOR Muscle cramps Muscle weakness Pain in joints Swollen joints Stiffness Deformity of joints