PATIENT HEALTH QUESTIONS
advertisement

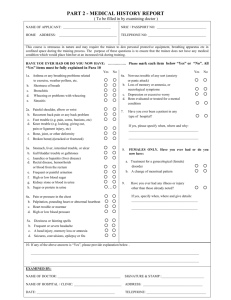
PATIENT HEALTH QUESTIONNAIRE NAME_________________________________ DATE of BIRTH_________________DATE____________ PLEASE TRY TO ANSWER ALL QUESTIONS ON BOTH SIDES. THIS INFORMATION WILL BE TREATED AS CONFIDENTIAL PAST HEALTH Have you ever suffered from any of the following conditions? Yes No Yes No Anemia Thyroid Trouble Diabetes Rheumatic Fever High Blood Pressure Heart Disease Tuberculosis Pneumonia Stomach Ulcers Kidney Disease Yes No Back Pain Emotional Problems Epileptic Seizures Allergies Jaundice (infections) Do you take any medications regularly? Yes No If yes, please list:_________________________________ _________________________________________________________________________________________ Alcohol use? Yes No Illicit Drug use? Yes No Amount:___________________________ Type:______________________________ Please list any significant illnesses or operations you have had. Date Illness or Operation Doctor and/or Hospital _____________________ _____________________________________________ ________________________________ _____________________ _____________________________________________ ________________________________ _____________________ _____________________________________________ ________________________________ _____________________ _____________________________________________ ________________________________ _____________________ _____________________________________________ ________________________________ FAMILY HEALTH Age Father Mother Health Problems If Deceased, Cause of Death Age at Death Has any Blood Relative Had Tuberculosis Heart Disease High Blood Pressure Brothers and Sisters Alcoholism Kidney Disease Diabetes Strokes Children Epilepsy Mental Illness Allergies Lung Disease Page 1 of 2 Y N PATIENT HEALTH QUESTIONNAIRE Are you affected by any of the following? Yes No Fatigue Loss of Appetite Loss of Weight Fever Chills HEAD & NECK Yes No Headaches Eye Trouble Hearing Difficulty Earaches Sinus Trouble RESPIRATORY Yes No Cough Sputum Bloody Sputum CARDIOVASCULAR Yes No Shortness of Breath Chest Pain Palpitations DIGESTIVE Yes No Difficulty Swallowing Heartburn Nausea Vomiting URINARY Yes No Frequency of Urination Painful Urination LOCOMOTOR Yes No Pain, stiffness, joint swelling Limitation joint movement NERVOUS SYSTEM Yes No Forgetfulness Nervousness Depression Spells of Any Kind WOMEN ONLY Yes No Irregular Menstruation Painful Menstruation Very Heavy Periods Bleeding between Periods Page 2 of 2 Yes No Night Sweats Intolerance to Heat Intolerance to Cold Any Skin Trouble Fainting Yes No Difficulty Sleeping Bleeding Tendency Date of Last Tetanus Shot Date of Late Polo Shot Yes No Nasal Congestion Nose Bleeds Hay Fever Dental Trouble Sore Tongue Yes No Frequent Colds Sore Throat Lumps in Neck Neck Pain Yes No Wheezing Shortness of Breath Date of last TB test Yes No Cigarette Smoking Number Daily? Date of last Chest X-Ray Yes No Swelling of Ankles Pains in Legs Varicose Veins Yes No Have you ever has an EKG (Electrocardiogram)? When? High Blood Pressure Yes No Abdominal Pain Gas Constipation Diarrhea Yes No Bloody Stools Black Stools Do you take Laxatives? Do any foods cause indigestion? Yes No Change of Urine Appearance Incontinence Yes No Getting up at night to urinate? How Many Times? Yes No Any broken bones? Foot Trouble Yes No Back Pain Deformities Yes No Abnormal Sensations Loss of Balance Clumsiness Muscle Weakness Yes No Difficulty Walking Tremors Dizziness Yes No Are You Passed Menopause Abnormal Discharge Do you take Birth Control Pills Any trouble with Breasts Number Of Pregnancies Number Of Miscarriages Date of last Menstrual Period Date of Last Pap Smear