Management of Urinary tract infection in Childhood – Based NICE
advertisement

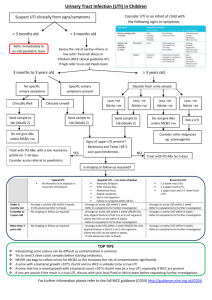
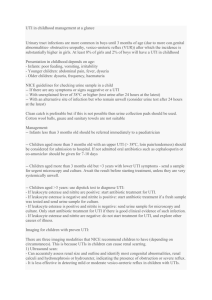
Management of Urinary tract infection in Childhood – Based NICE 54 (Aug07) 1. History and Examination To include recording presence or absence: poor urine flow, previous UTI or recurrent PUO, antenatal anomalies, FH of ureteric reflux or kidney disease, constipation, dysfunctional voiding, enlarged bladder, abdominal mass, evidence of spinal anomaly, poor growth , high blood pressure 2. Obtain urine for testing Clean catch urines should be obtained from all children with unexplained fever greater than 38 deg C or symptoms or signs of UTI: vomiting, frequency, dysuria, poor feeding, failure to thrive, abdo pain, acute incontinence, malaise, offensive urine – Supply sterile galipot while waiting Alternatives to clean catch such as bag urine, CSU and SPA should only be used if clean catch not possible. E.g. urgent full infection screen indicated in young child – SPA should always use ultrasound to confirm urine in bladder 3. Testing urine Less than 3 years – send for urgent microscopy and culture Over 3 years – Use dipstick to diagnose UTI Managing results: Microscopy less than 3 years: Bacturia positive Bacturia negative Leucocytes positive UTI UTI if supportive signs Leucocytes neg. UTI Not UTI Dipstick – over 3 years Leuc + nitr+ Treat send for culture if previous infection or risk of serious illness Leuc – nitr + Treat send for culture Leuc + nitr Send for culture treat only if good clinical evidence Leuc – nitr Do not treat Do not send for culture unless recurrent 4. Treatment Less than 3 months – treat as per childhood fever – full septic screen and iv antibiotics Over three months and unwell – 7- 10 day oral antibiotics – trimethoprim If not tolerated or septicaemic then iv cefuroxime Over three months,if bacturia /dysuria frequency alone with no systemic features- cystitis trimethoprim 3 days only) 5. Further Investigations: Child < 6 months: USS within 6 weeks alone unless: Atypical or recurrent: Urgent USS, MCUG as OPD, DMSA @ 4-6 months 6 month -3 years: no investigations unless: Atypical – Urgent USS, DMSA @4-6 month Recurrent – USS within 6 weeks, DMSA @4-6 month Child > 3 years: No investigations unless: Atypical - Urgent USS Recurrent – USS within 6 weeks DMSA @ 4-6 months Definitions: Atypical : severely ill, poor urine flow, abdominal or bladder mass, raised creatanine, septicaemia, failure to respond to antibiotics within 48 hrs, infection with non E.coli organisms Recurrent: one Pylonephritis plus any other UTI or three cystitis ( pylonephritis = bacturia with fever or loin pain) 6. Prophylaxis – not covered in NICE guideline (trimethoprim 2 mg kg nocte) Recurrent UTI – 6 weeks pending ultrasound, consider 3 months treatment if 2 infections in 3 months Known antenatal renal tract dilatation – until resolved or 2 years Proven renal scar – until 4 years 7. Follow up: No follow up: if no investigations or if investigations are normal (letter to parents) Recurrent UTI or with abnormal tests – follow up at 3 months – if scar need growth blood pressure and proteinuria screening (unilateral small scar use judgement)