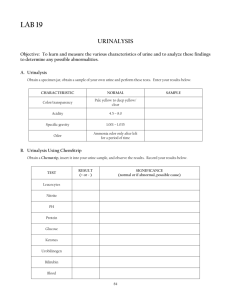
Urobilinogen/Blood/Ketone/Glucose/Protein/pH
advertisement

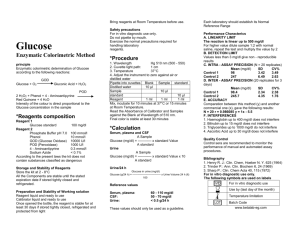
Atlas Link 12720 Dogwood Hills Lane, Fairfax, VA 22033 USA Phone: (703) 266-5667, FAX: (703) 266-5664 http://www.atlaslink-inc.com, info@atlaslink-inc.com INTENDED USE: Urine reagent strips- 7 parameters (URS-7) for Urinalysis are firm plastic strips to which are affixed several separate reagent areas. Urine reagent strips provide tests for the semi-quantitative determinations of pH, protein, glucose, ketone, bilirubin, blood, and urobilinogen in urine. Test results may provide information regarding the status of carbohydrate metabolism, kidney function, liver function, and acid-base balance.1,2 SUMMARY AND EXPLANATION: The reagent test areas of urine reagent strips are ready to use upon removal from the bottle. The entire reagent strip is disposable. No additional laboratory equipment is necessary for testing. The directions must be followed exactly. Accurate timing is essential to provide optimal results. The reagent strips must be kept in the bottle with the cap tightly closed (as specified on the cap) to maintain reagent reactivity. To obtain optimal results, it is necessary to use fresh, well-mixed, and uncentrifuged urine. TEST PRINCIPLES pH: This test is based on a double indicator principle that gives a broad range of colors covering the entire urinary pH range. Colors range from orange through yellow and green to blue. Protein: This test is based on the protein error-of-indicators principle. At a constant pH, the development of any green color is due to the presence of protein. Colors range from yellow for "Negative" through yellow-green and green to green-blue for "Positive" reactions. Glucose: This test is based on a double sequential enzyme reaction. One enzyme, glucose oxidase, catalyzes the formation of gluconic acid and hydrogen peroxide from the oxidation of glucose. A second enzyme, peroxidase, catalyzes the reaction of hydrogen peroxide with a potassium iodide chromogen to oxidize the chromogen to colors ranging from green to brown. Ketone: This test is based on the reaction between acetoacetic acid with nitroprusside. The colors range from buff-pink, for a "Negative" reading to purple. Bilirubin: This test is based on the coupling of bilirubin with diazotized dichloroaniline in a strongly acid medium. Blood: This test is based on the peroxidase-like activity of hemoglobin which catalyzes the reaction of cumene-hydroperoxide and 3,3',5,5' tetramethylbenzidine. The resulting color ranges from orange through green to dark blue. Urobilinogen: This tests is based on the Ehrlich reaction in which pdimethylaminobenzaldehyde reacts with urobilinogen in a strong acid medium to produce a brown-orange color. REAGENTS: (Based on dry weight at time of impregnation) pH: 0.2% w/w methyl red; 2.8% w/w bromthymol blue; 97% w/w nonreactive ingredients. Protein: 0.3% w/w tetrabromphenol blue; 99.7% w/w buffer and nonreactive ingredients. Glucose: 16.3% w/w glucose oxidase (Aspergillus niger, 1.3 IU); 0.6% w/w peroxidase (Horseradish, 3300 IU); 7.0% w/w of potassium iodide; 76.1% w/w buffer and nonreactive ingredients. Ketone: 7.1% w/w sodium nitroprusside buffer balanced with buffer and nonreactive ingredients. Bilirubin: 0.4% w/w 2,4-dichloroaniline diazonium salt, balanced with buffer and nonreactive ingredients Blood: 22.5% w/w cumene hydroperoxide, balanced with buffer and nonreactive ingredients Urobilinogen: 2.9% w/w p-dimethylaminobenzaldehyde, balanced with buffer and nonreactive ingredients URINE REAGENT STRIPS (7 PARAMETERS) pH, Glucose, Protein, Ketone, Bilirubin, Blood, and Urobilinogen WARNINGS AND PRECAUTIONS: Urine reagent strips are for in vitro diagnostic use. STORAGE: Store at temperature between 4 - 30°C (39 - 86° F) and out of direct sunlight. Do not use after expiration date. RECOMMENDED HANDLING PROCEDURES: All unused strips must remain in the original bottle. Transfer to any other container may cause reagent strips to deteriorate and become unreactive. Do not remove desiccant(s) from bottle. SPECIMEN COLLECTION AND PREPARATION: Collect urine in a clean container according to NCCLS GP16-T guideline and test as soon as possible. If testing cannot be done within an hour after voiding, refrigerate the specimen immediately and let it return to room temperature before testing. Prolonged exposure of unpreserved urine to room temperature may result in microbial proliferation with resultant changes in pH. A shift to alkaline pH may cause false positive results with the protein test area. Urine containing glucose may decrease in pH as organisms metabolize the glucose. Contamination of the urine specimen with skin cleansers containing chlorhexidine may affect protein test results. The user should determine whether the use of such skin cleansers is warranted. MATERIALS PROVIDED: 1. 1 bottle containing 100 URS-7 urine reagent strips. 2. A visual color chart for reading results is printed on the bottle. MATERIALS REQUIRED BUT NOT PROVIDED: 1. Clean dry container for urine sample. 2. Commercial urine controls. 3. A timer capable of reading accurately in seconds. PROCEDURE: MUST BE FOLLOWED EXACTLY TO ACHIEVE RELIABLE TEST RESULTS. 1. Collect FRESH urine specimen in a clean dry container. Mix well immediately before testing. 2. Remove one strip from bottle and close the cap immediately. Completely immerse reagent areas of the strip in FRESH urine and remove immediately to avoid dissolving out reagents. 3. While removing, run the edge of the strip against the rim of the container to remove excess urine. Alternatively, run the edge of the strip against a paper towel to remove excess urine. Hold the strip in a horizontal position to prevent possible mixing of chemicals from adjacent reagent areas and/or soiling of hands with uirne. 4. Compare reagent areas to corresponding color chart on the bottle label at the time specified. HOLD STRIP CLOSE TO COLOR BLOCKS AND MATCH CAREFULLY.Do not use the same urine sample more than once, as the urine may have been contaminated with the dissolving of the different reagent areas. Proper read time is critical for optimal results. All reagent areas may be read between 1 and 2 minutes for screening positive from negative specimens. QUALITY CONTROL: For best results, performance of reagent strips should be confirmed by testing known negative and positive specimens or control whenever a new test is performed or whenever a new bottle is first opened. Negative and positive specimens or controls may also be randomly hidden in each batch of specimens tested. Each laboratory should establish its own goals for adequate standards of performance, and should question handling and testing procedures if these standards are not met. Atlas Link, 12720 Dogwood Hills Lane, Fairfax, VA 22033 USA Phone: (703) 266-5667, FAX: (703) 266-5664 http://www.atlaslink-inc.com, info@atlaslink-inc.com RESULTS: Results are obtained by direct comparison of the color blocks printed on the bottle label. LIMITATIONS OF PROCEDURE: pH: If proper procedure is not followed and excess urine remains on the strip, a phenomenon known as "runover" may occur, in which the acid buffer from the protein reagent will run onto the pH area, causing a false lowering in the pH result. measured with the exception of interferences listed previously (see LIMITATIONS OF PROCEDURE). For visually read strips, accuracy is a function of the manner in which the color blocks on the bottle label are determined and the discrimination of the human eye in reading the test. Precision is difficult to assess in a test of this type because of the variability of the human eye. It is for this reason that users are encouraged to developed their own standards of performance. Protein: False positive results may be obtained with highly buffered or alkaline urine. Contamination of the urine specimen with quaternary ammonium compounds may also produce false positive results.3 Glucose: Large amounts of ketone bodies (50 mg/dl or greater) may decrease color development. However, it is unlikely that the presence of ketones simultaneously with glucose in the urine is sufficient to produce false negative results. At glucose levels of 1 g/dl or greater, the color may appear somewhat mottled. The darkest color should be used in interpreting results with the color chart. The reactivity of the glucose test decreases as the SG of the urine increases. Reacttivity may also vary with temperature.4 Ketone: Color reaction that could be interpreted as "positive" may be obtained with urine specimens containing MESNA or large amounts of phenylketones or L-dopa metabolites.5 Bilirubin: Reactions may occur with urine specimens containing large doses of chlorpromazine or rafampen which might be mistaken for positive bilirubin. 6 The following table lists % agreement in laboratory comparison study between Teco's URS-7 and Ames’ Multistix, using 76 samples. Reagent Parameter % Agreement pH 96% Protein 97% Glucose 96% Ketone 96% Bilirubin 97% Blood 95% Urobilinogen 97% Blood: the sensitivity of the blood test is reduced in urine with high specific gravity and/or high ascorbic acid content. Microbial peroxidase, associated with urinary tract infection, may cause a false positive reaction. *Those samples that produced different results were off by no greater than one color block. Urobilinogen: The test area will react with interfering substances known to react with ehrlich's reagent, such as porphobilinogen and p-aminosalicylic acid.6 The test is not a reliable method for the detection of porphobilinogen. Drugs containing azo-dyes (e.g., Azo Gantrisin) may give a masking golden color. The absence of urobilinogen cannot be determined with the product. Sensitivity: pH Test: The pH test area permits quantitative differentiation of pH values to one unit within the range of 5 - 9. pH readings are not affected by variation in the urinary buffer concentration. EXPECTED VALUES: pH:3 newborn: 5 - 7 thereafter: 4.5 - 8 average: 6 Protein: In 24 hours urine, 1-14 mg of protein in 1 dL of urine may be excreted by the normal kidney.3 A color matching any block greater than Trace indicated significant proteinuria. For urine of high specific gravity, the test area may most closely match the trace color block even though only normal concentrations of protein are present. Clinical judgment is needed to evaluate the significance of trace results. Glucose: Small amount of glucose are normally excreted by the kidney. 4 Concentrations of as little as 0.1 g/dl glucose, read either at 10 or 30 seconds, may be significantly abnormal if found consistently. At 10 seconds, results should be interpreted qualitatively; i.e., negative or positive. for quantitation, read at 30 seconds only. Ketone: Normally no ketones are present in urine. Detectable levels of ketone may occur in urine during physiological stress conditions such as fasting, pregnancy, and frequent strenuous exercise. 5-8 In starvation diets, or in other abnormal carbohydrate metabolism situation, ketones appear in the urine in excessively large amounts before serum ketones are elevated.9 Bilirubin: Normally no bilirubin is detectable in urine by even the most sensitive methods. Even trace amounts of bilirubin are sufficiently abnormal to require further investigation. Atypical colors (colors produced which are different than the negative or positive color blocks shown on the Color Chart) may indicate that bilirubin derived bile pigments are present in the urine sample and are possibly masking the bilirubin reaction. Blood: Any blue spots or blue color developing on the reagent area within 40 seconds is significant and the urine should be examined further. Blood is frequently, but not invariably, found in the urine of menstruating females. Urobilinogen: In a healthy population, the normal urine urobilinogen range obtained with this test is 0.1 to 1.0 Ehrlich unit per dl. SPECIFIC PERFORMANCE CHARACTERISTICS: The performance characteristics of URS-7 urine reagent strips have been determined both in the laboratory and in clinical tests. Parameters of importance to the user are sensitivity, specificity, accuracy and precision. Generally, this test has been developed to be specific for the constituent to be Protein Test: Quantitative results are obtained from this test area. 5 to 20 mg of albumin per dl urine may be detected as a "Trace" result. The test area is more sensitive to albumin than to globulin, hemoglobin, and mucoprotein; a negative result, therefore, does not rule out the presence of these other proteins. Glucose Test: This reagent test area may be read at 10 seconds for qualitative results or 30 seconds for quantitative results. The test is specific for glucose; no substance excreted in urine other than glucose is known to give a positive result. The reagent area does not react with lactose, galactose, fructose, nor reducing metabolites of drugs; e.g., salicylates and nalidixic acid. This test may be used to determine whether the reducing substance found in urine is glucose. Approximately 0.1 g of glucose per dl or urine is detectable. Ketone Test: The ketone test area provides semi-quantitative results (small, moderate, and large) and reacts with acetoacetic acid in urine. It does not react with beta-hydroxybutyric acid or acetone. The reagent area detects as little as 5 to 10 mg acetoacetic acid per dl of urine. Bilirubin Test: The test has a sensitivity of 0.2 - 0.4 mg bilirubin/dl. The test is considered specific for bilirubin in urine. Blood Test: At the time of reagent manufacture, the test when read as instructed has a sensitivity to free hemoglobin of 0.015 mg/dl or 5 intact red blood cells/ul in urines with a specific gravity and ascorbic acid content. The test is slightly more sensitive to free hemoglobin and myoglobin than to intact erythrocytes. Urobilinogen Test: This test area gives quantitative results and will detect urobilinogen in concentrations as low as an Ehrlich unit/dl in urine. The absence of urobilinogen in the specimen being tested cannot be determined. BIBLIOGRAPHY: 1. Free, A.H. and Free, H.M.: Urinalysis, Critical Discipline of Clinical Science. CRC Crit. Rev. Clin. Lab. Sci. 3(4): 481-531; (1972). 2. Yoder, J..Adams, E.C., and Free, H.M.: Simultaneous screening for urinary occult blood, protein, glucose and pH. Amer. J. Med Tech. 31: 285; (1965). 3. Tietz, N.W.: Clinical Guide to Laboratory Tests; W.B. Saunders Company, (1976). 4. Schersten, B. and Fritz, H.: Subnormal Levels of Glucose in urine. JAMA 201:129-132; (1967). Atlas Link, 12720 Dogwood Hills Lane, Fairfax, VA 22033 USA Phone: (703) 266-5667, FAX: (703) 266-5664 http://www.atlaslink-inc.com, info@atlaslink-inc.com 5. 6. 7. 8. 9. McGurry, J.D.: Lilly Lecture, 1978: New Perspectives in the Regulation of Ketogenesis. Diabetes 28: 517-523 May, (1978). Burtis C.A. and Ashwood E.R.: Tietz Textbook of Clinical Chemistry 2nd. Ed. 2205; 1994 Williamson, D.H. Physiological Ketoses, or Why Ketone Bodies? Postgrad. Med. J. (June Suppl.): 371-375; (1971). Paterson, P. et al.: Maternal and Fetal Ketone Concentrations in Plasma and Urine. Lancet: 862-865; April 22, (1967). Fraser, J.et al.: Studies with a Simplified Nitroprusside Test for Ketone Bodies in Urine, Serum, Plasma and Milk. Clin. Chem. Acta II: 372-378; (1965). Rev: 8/96 Atlas Link, 12720 Dogwood Hills Lane, Fairfax, VA 22033 USA Phone: (703) 266-5667, FAX: (703) 266-5664 http://www.atlaslink-inc.com, info@atlaslink-inc.com