Outpatient MSK Physiotherapy Referral:
advertisement

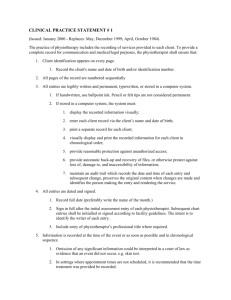
Physiotherapy Referral Form Hillingdon Community Physiotherapy Services Please select and tick required service (1, 2 or 3): 1. Outpatient MSK o o o o o o o (select preferred clinic below) West Drayton Physio Centre The Warren Uxbridge Health Centre Laurel Lodge Clinic Harefield Health Centre Westmead Clinic Eastcote Health Centre PATIENT DETAILS Title: 2. Neuro Physio 3. Community Physio (home visit) PLEASE COMPLETE ALL DETAILS IN BLOCK PRINT Mr /Mrs /Miss /Ms (please circle) Surname………………………………… Forename…………………………… D.O.B……………… Address………………………………………………………………………………………………………. Post Code………………………………………... NHS number……………………………………… Daytime Contact Number………………………. Mobile Tel No…………………………………….. Ethinicity ………..……………………. Speaks English? Yes/No Own Transport? Yes /No If patient needs translator - which Language?................................ REASON FOR REFERRAL: How long has the condition been present? < 6 weeks □ >6 weeks □ <6 months □ > 6 months □ Does this problem mean the patient is…. Off work YES □ NO □ Struggling at work YES □ NO □ Having significant sleep problems YES □ NO □ Having difficulty caring for dependents YES □ NO □ Site of Problem Low Back Pain Neck pain Headaches Referred arm pain Referred leg pain Shoulder Elbow Wrist Hand Hip Knee Ankle Foot Women’s Health Medical History □ □ □ □ □ □ □ □ □ □ □ □ □ □ Heart Disease Hypertension Depression/Anxiety Diabetes Epilepsy Asthma /COAD Steroid therapy Anticoagulants Metabolic bone disease Pacemaker Pregnancy DXT R.A TB Other:- Current Medication □ □ □ □ □ □ □ □ □ □ □ □ □ □ Please list:- Name of referring GP:……………………….. Signature of referring GP: …………………. Date…………………….. Practice stamp: Please Fax completed form to the Contact Centre at Kirk House On: 01895 625268 OR electronically attach with Choose and Book referral booking