Angola Marburg Hemorrhagic Fever Outbreak Response 2005 (Word)
advertisement
")
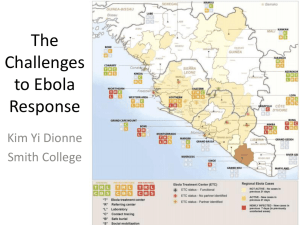
TABLE OF CONTENTS 1. EXECUTIVE SUMMARY ................................................................................................................ 1 1.1 1.2 1.3 2. CONTEXT AND HUMANITARIAN CONSEQUENCES ................................................................. 4 2.1 2.2 3. Context ................................................................................................................................... 4 Humanitarian Consequences................................................................................................. 5 RESPONSE PLAN ......................................................................................................................... 6 3.1 4. Priority Needs......................................................................................................................... 2 Resources Required .............................................................................................................. 3 Timeframe of Appeal .............................................................................................................. 3 Expected Results ................................................................................................................... 7 ADDITIONAL ROLES AND RESPONSIBILITIES ......................................................................... 8 ANNEX I. ACRONYMS AND ABBREVIATIONS ................................................................................... 9 iii UÍGE IS THE MOST AFFECTED REGION iv MARBURG HEMORRHAGIC FEVER OUTBREAK RESPONSE 1. EXECUTIVE SUMMARY As of 6 April 2005, 181 confirmed and suspected cases of Marburg viral hemorrhagic fever (VHF) have been reported in five provinces, with the majority (168) in Uige. Of the 181 cases, 159 have been fatal.1 While children under the age of five years initially accounted for 75% of cases, recent cases are including an increasing number of adults. The epicentre of this outbreak is Uige Province, which remains the primary focus of outbreak response activities. Two cases have been confirmed in Luanda. In addition, alert cases have been reported in four other provinces (Cabinda, Malanje, Kwanza Norte, and Zaire). Three further provinces (Bengo, Kwanza Sul, and Lunda Norte) – sharing internal borders with Uige province – are considered at increased risk. As surveillance and reporting mechanisms improve, the number of alert, suspect and confirmed cases, as well as the number of municipalities affected, is likely to increase. The Angolan Ministry of Health (MINSA) is responsible for coordinating the national response to the Marburg VHF epidemic. The World Health Organization (WHO) Country Office, Regional Office for Africa /AFRO), and Headquarters, in collaboration with the United Nations Children’s Fund (UNICEF), the World Food Programme (WFP), Médecins Sans Frontières (MSF), and the International Federation of Red Cross and Red Crescent Societies (IFRC), are supporting MINSA and coordinating the mobilisation of international technical support. The capacity of the Ministry of Health to implement outbreak control, to enhance surveillance and data collection, is hampered by lack of trained human resources, lack of personal protective equipment and supplies, limited information systems to deal with case finding and contact tracing, and limited technical and operational coordination and logistics. On-going operations on the ground are prioritised as: Addressing immediate needs in Uige Province, to control the outbreak through establishment of an effective isolation facility (taken on board by MSF), intensive case/contact tracing, social mobilisation for community awareness, and support to epidemic control and co-ordination of response activities; Ensuring that Luanda, other provinces in Angola and border areas are on a heightened state of alert and are adequately prepared to deal rapidly with any case(s) that may occur; Investigating events/rumours rapidly in other areas; Raising awareness among the heath personnel for early detection (in particular hospitals and other frontline health facilities) and precautions when taking care of suspected cases; Sustaining multidisciplinary technical support from WHO and the Global Outbreak Alert and Response Network (GOARN) in the field (including clinical management, infection control, epidemiology, laboratory, social mobilisation, medical anthropology, logistics and communications). To effectively support the national surveillance and epidemic preparedness and response, and to ensure coordination of international technical support, WHO has mobilised regional networks of experts and GOARN and has strengthened collaboration and coordination with partners such as UNICEF, MSF and the IFRC in Angola. WHO is coordinating intensive investigation of rumours and alert in other countries, particularly those countries bordering Angola. National health authorities in the Democratic Republic of Congo (DRC) and Republic of Congo have enhanced surveillance in bordering areas. In DRC – in response to an alert case in Matadi – a national team supported by the WHO Country Office is alerting the local population, augmenting surveillance and performing active case finding. MSF teams in Bas-Congo are also on the alert and implementing readiness measures. WHO/AFRO is providing regular situation reports to all WHO Country Offices in the Region to avoid panic and inappropriate restrictions on travel and trade. 1 Cumulative totals since cases of VHF were first reported in Uige in October 2004 (source MINSA/WHO). 1 MARBURG HEMORRHAGIC FEVER OUTBREAK RESPONSE This epidemic is the latest VHF outbreak in central Africa (previous ones having occurred in Gabon, Congo Brazzaville, the Democratic Republic of Congo, southern Sudan and Uganda) and underlines the need to rapidly strengthen a sub-regional alert and response network focused on VHFs, and to capitalise on the limited capabilities developed during outbreak response over the past 5 years. This will be the subject of a further appeal for financial support. Flash Appeal for Angola Marburg VHF 2005 Summary of Requirements - By Appealing Organisation as of 12 April 2005 http://www.reliefweb.int/fts Compiled by OCHA on the basis of information provided by the respective appealing organisation. Appealing Organisation Original Requirements 848,000 UNICEF WFP 285,000 WHO 2,370,000 3,503,000 Grand Total Flash Appeal for Angola Marburg VHF 2005 Summary of Requirements - by Sector as of 12 April 2005 http://www.reliefweb.int/fts Compiled by OCHA on the basis of information provided by the respective appealing organisation. Original Requirements Sector Name COORDINATION AND SUPPORT SERVICES 285,000 HEALTH 3,218,000 3,503,000 Grand Total 1.1 Priority Needs Case management Establish isolation units for care and treatment in Uige and Luanda, and any other focus of the outbreak that may occur; Train and improve safe case management skills of technicians and health care workers; Procure and distribute protective materials to health care workers in Uige and the eight other high-risk provinces; Procure and distribute emergency kits and essential drugs to Uige and the high-risk provinces; Procure and distribute disinfectant materials to Uige and the high-risk provinces; Procure and distribute other case management equipment and consumables to Uige and the high-risk provinces; Provide cash incentives for case management, infection control, and burial teams. Surveillance and epidemiology Set up an active surveillance system in Uige Province, Luanda and Cabinda able to detect any case in the community; Set up mobiles team structure to respond to alerts, identify cases, and follow-up contacts for 21 days; Provide cash incentives for active surveillance teams; Train health care workers, surveillance officers and data managers in all provinces of Angola for surveillance, investigation of alerts, taking of samples and mobilisation of response; 2 MARBURG HEMORRHAGIC FEVER OUTBREAK RESPONSE Provide operation support to maintain the field laboratory in Uige and enzyme-linked immunosorbent assay (ELISA), ribonucleic acid (RNA) and molecular biology testing facilities in Luanda, and ensure rapid transfer of samples for analysis; Provide sustained international technical support for epidemiological investigation, training, surveillance evaluation, and outbreak response activities. Social mobilisation, risk reduction and health education To strengthen public confidence in, and cooperation with, the local and national health authorities and services; Launch intensive social mobilisation campaign through mass media and community activists; Develop tools and appropriate methods (social mobilisation and information, education, and communication (IEC) materials) to avoid risky behaviours, particularly associated with burial practices and customs, and case management at home; Evaluate the situation in the field regarding social mobilisation, and to inform and adapt control strategies to take account of local beliefs and customs; Develop contingency plans for areas not currently directly affected by the outbreak; Provide support to orphaned and widowed family members of health care workers. Logistics Procure and install communication equipment, computers, and other hardware as per provincial priorities; Provide transportation support for surveillance and mobilisation activities (vehicles, motorcycles, bicycles); Provide support for repair and maintenance of vehicles and equipment; Provide cash support for WFP air passenger services directly linked with Marburg VHF response for a minimum of 6 months. Other priority needs Document activities and lessons learned, and disseminate accurate information to all partners. 1.2 Resources Required Appeal Summary Appealing Organisation World Health Organization (WHO) United Nations Children’s Fund (UNICEF)* World Food Programme (WFP) Total Requirements (US$) 2,370,000 848,000 285,000 3,503,000 * The actual recovery rate on individual contributions will be calculated in accordance with the Executive Board Decision 2003/9 of 5 June 2003. Financial Summary Sector Case Management Surveillance and Epidemiology Social Mobilisation Logistics (including support for WFP air passenger services) Total 1.3 Timeframe of Appeal The timeframe of the appeal is three months, April-June 2005. 3 Requirements (US$) 1,007,000 1,254,500 620,200 621,300 3,503,000 MARBURG HEMORRHAGIC FEVER OUTBREAK RESPONSE 2. CONTEXT AND HUMANITARIAN CONSEQUENCES 2.1 Context MINSA and its partners (WHO, UNICEF, the Centre for Disease Control (CDC), and MSF) have created a National Technical Commission to combat the Marburg outbreak. The Commission has strengthened coordination mechanisms in the areas of logistics, epidemiology, and social mobilisation to prevent the further spread of the virus, and to direct isolation and treatment interventions in Uige, Luanda, and other locations where there are now confirmed or suspected cases. The Commission and Sub-commissions of Epidemiological Surveillance, Logistics and Social Mobilisation meet daily. A case definition of VHF has been adopted to enhance knowledge of the disease and promote accurate identification of suspected cases. The Commission has sent a protocol to all Provincial Health Departments to provide orientation for health workers on how to identify alert and suspected cases. Intensive training for health workers is ongoing in Uige and Luanda and now includes staff from private clinics. In addition, the Government has mobilised US$ 3 million and has announced that the Armed Forces of Angola (FAA) will provide logistics support and medical staff to help prevent the further spread of the virus. Angola has eased customs and duty procedures for donor vehicles and shipments of equipment and supplies for the control of the outbreak. Over 60 international experts in various fields representing WHO, MSF, UNICEF and other partners in GOARN have now been mobilised to Angola. Outbreak response teams are in the field in Uige Province, in Cabinda and in Luanda. These teams are providing rapid technical support for case management, intensified contact tracing and surveillance, infection control and to improve public understanding of the disease and its modes of transmission. In Luanda, MSF Holland is supporting MINSA to open a preventive isolation unit in Americo Boa Vista Hospital and a transitory isolation unit will be set up at the Paediatric Hospital to allow for safe screening of potential cases there. In Uige, a WHO outbreak response team is proving technical and operational support to local health authorities and is carrying out intensive case finding and contact tracing, and burying bodies. MSF Spain has established an isolation ward in the Provincial Hospital, which is now operational. MSF Spain has sent 18 staff members to the province who are now fully in charge of case management and infection control and are providing intensive care for patients at the Provincial Hospital. The occurrence of unreported cases in communities is still of concern and case-finding and contact tracing is the priority activity to end the chain of transmission in Uige city and other surrounding municipalities. Five mobile surveillance teams are now working in Uige, following up 100 contacts. Social mobilisation efforts are critically important to the control of VHF outbreaks. Currently the population is - rightly - wary of hospital-related infection, and other local beliefs (linking the disease with witchcraft practices) play an important role. WHO has a team of medical anthropologists working closely with social mobilisation experts and the response team to incorporating these complex elements into the overall control strategy and to adapt social mobilisation activities. Social mobilisation at national level will be stepped up with a multimedia campaign designed by MINSA and UNICEF. Information leaflets, posters and a series of TV and radio spots are under production. In addition to the general population, target groups are health workers, children and people attending funerals. Two social mobilisation specialists from WHO and GOARN have arrived in the country. Traditional partners such as international and national non-governmental organisations (NGOs), as well as the Scouts of Angola are also being trained to support the essential interpersonal communication aspect of the social mobilisation program. Partners are also focusing on increasing the readiness and preparedness of high-risk provinces neighbouring Uige, as well as Luanda and Cabinda. The existing provincial early detection network for Measles and Polio is now ensuring surveillance for identification and classification of Marburg cases. WHO and UNICEF will shortly pre-position protection equipment and medical supplies for health workers in health facilities in all high-risk provinces, with WHO developing similar plans that will eventually include all 18 provinces. MSF and the NGO liaison group, the Consortium of NGOs in Angola (CONGA), are mapping existing NGO capacity in order to optimise the response in Uige and elsewhere. 4 MARBURG HEMORRHAGIC FEVER OUTBREAK RESPONSE Multidisciplinary response teams from WHO (including the country office, inter-country program, regional office and headquarters), together with Collaborating Centres and GOARN partners are providing the additional technical expertise and capability to support the MINSA in the control of this outbreak rapidly. WHO will continue to mobilise and support field teams of epidemiologists, medical anthropologists, infection control specialists, barrier-nursing trainers and supervisors, risk communications and behavioural change experts, sanitation technicians and engineers, information and data managers, laboratory technicians, and many other categories of health and public health experts. It is critically important to sustain the necessary level of technical support and ensure strong coordination until the epidemic is ended. The Canadian National Microbiology Laboratory has set up a mobile laboratory in Uige to help with the rapid identification of cases and for clinical management. In Luanda, the CDC has established ELISA 2 and RNA testing facilities at the National Institute for Public Health in Luanda. In addition to the CDC, the European Program for Intervention Epidemiology Training, the Swiss Agency for Development and Cooperation, Department of Humanitarian Aid are mobilising epidemiologists, infection control experts and communications officers to join the WHO/GOARN team. Experts from the Department of Infectious Diseases, North Manchester General Hospital, United Kingdom and Johannesburg Hospital, South Africa are providing assistance in infection control in Luanda, where training is being provided for health care staff from all provinces in the country. Expert resources and material have been mobilised from across WHO's African Regional and Country offices, including the Republic of Congo/Brazzaville, the Democratic Republic of Congo, and Mozambique. The Brazilian Ministry of Health has mobilised the services of two technical experts who will travel to Angola within the first week of April. Additional resources have been volunteered and are currently on stand-by from France, Norway, South Africa, Sweden and the United Kingdom. 2.2 Humanitarian Consequences Marburg VHF has no specific treatment other than re-hydration and supportive care; there is no licensed commercialised vaccine at present. The Angola epidemic is now the worst known outbreak ever, surpassing the previous total number of Marburg VHF cases (148) recorded in the Democratic Republic of Congo in 1998-2000. When it became apparent to the local community that the epidemic was centred in Uige, specifically Uige Hospital, and when health care workers that had been in contact with infected patients also began dying, the Provincial Hospital effectively shut down and patients were abandoned, as health care staff were too afraid to report to work, knowing that they lacked the most basic protective clothing and equipment. Family members of the sick were exposed to further risk because patients could not be isolated and were cared for at home. In addition, those that had been in contact with patients avoided quarantine measures out of fear that if they were not already infected by the virus, they soon would be if they remained in the proximity of the hospital or confined to their homes. The analysis of the epidemiological situation of Marburg VHF in Angola and the response to the epidemic reveals major public health concerns. Five provinces have had alerts related to suspect cases of disease originating from Uige Province. To date case fatality is very high (91.8%) and most of the cases are children (61%). The case incidence is increasing and in-migration patterns suggest that at least nine districts (municipalities) are at high risk or already have confirmed/suspected cases of the virus. Although a national epidemic control management committee is in place and functioning, provincial structures are not yet ready in all high-risk provinces. Health and public health staff in Uige remained at risk of acquiring the infection because of the lack of specialised training and protective equipment. Technical guidelines are now being distributed, including information on how the community can participate in case reporting and verification, social mobilisation, and to promote safe burial practice, and avoid other risky behaviours. Until active surveillance and social mobilisation is effective in all high-risk provinces, new, perhaps preventable cases will continue to be identified. As the virus Enzyme-linked immunosorbent assay. ELISA tests are widely utilised to detect substances that have antigenic properties, including hormones, bacterial antigens and antibodies. 2 5 MARBURG HEMORRHAGIC FEVER OUTBREAK RESPONSE spreads and affects more parts of the country, effective case management and isolation becomes even more complicated, and humanitarian consequences more dire. Given the impact of the outbreak on movement into and out of Uige Province, and the disruption of normal commercial activities, food and other consumer prices in the city of Uige have skyrocketed. Anecdotal reports indicate that the price of household bleach, if it can be found, has increased by ten times, as residents implement their own disinfection methods, following the advice of public health officials. In the coming days, more communities, including those in other provinces that depend on Uige for trade, may face some difficulty with shortages of basic commodities In addition to the loss of life, family members of those infected by the virus, as well as the general population of Uige Province, have been stigmatised due to a lack of understanding of how the virus is spread and who is at risk. 3. RESPONSE PLAN Under the auspices of the Resident/Humanitarian Coordinator's office, WHO with the active support of UNICEF, is leading the international response to the Marburg VHF epidemic in Angola. Following laboratory confirmation of Marburg virus by CDC on 21 March, MINSA formally declared the outbreak of Marburg hemorrhagic fever on 24 March and requested assistance from WHO and international partners. Since then there has been an immediate mobilisation of resources by the international community, donors, and the Government of Angola to fight the outbreak. As part of a coordinated approach, WHO, UNICEF, WFP, and other UN agencies are currently supporting MINSA with logistical and technical support. MINSA and WHO are responsible for coordinating all activities in response to the epidemic. To date, MSF (Belgium, France, Holland and Spain) has assumed the bulk of the responsibility in establishing isolation units and case management procedures. In addition to MSF, NGOs already on the ground in Uige have played a crucial role in social mobilisation and case detection, and in the case of one NGO, have lost health personnel in the fight against the virus. The Provincial Department of Health has reengaged with the Uige Provincial Hospital, despite the fact that several of its staff were among the first victims of the virus prior to the provision of protective clothing and equipment and introduction of barrier-nursing procedures. MSF, WHO, UNICEF and other collaborating organisations will continue to provide support to MINSA with mobilisation of technical expertise and material support to help facilitate co-ordination and rapid response. MSF, WHO, UNICEF and other UN agencies will continue to participate in National Technical Commission meetings as well as provide strong technical support to the Sub-commissions, as well as participation at provincial level task force meetings in Uige, Luanda and other affected provinces. To date, WHO and UNICEF have utilised resources planned for alternative activities. WHO and UNICEF will need to replenish those already utilised resources as well as ensure adequate supplies to meet the known needs and have adequate contingency stocks to ensure rapid response in the event of further spread of the epidemic. Case management The most important and necessary supplies include protective clothing for health care workers, specifically goggles, face masks, heavy duty boots, gloves, and head wear, disinfectants for health units, mortuaries, and homes, as well as body bags, emergency kits and essential drugs. The priority is that personal protective equipment and supplies are provided to health authorities in Uige to fill gaps in existing materials, and ensure adequate supplies during the outbreak response. The remaining items will form pre-positioned strategic stockpiles in those provinces deemed high-risk, and as a contingency to support rapid investigation of alerts and rumours elsewhere, and respond appropriately to any new case. 6 MARBURG HEMORRHAGIC FEVER OUTBREAK RESPONSE Surveillance and epidemiology Active search for cases as well as the follow-up of people who have been in contact with suspected cases will continue. UNICEF and WHO will support MINSA to increase its logistics capacity, by providing vehicles, motorcycles, and bicycles. WHO has identified communications equipment and computers that MINSA requires to be able to adequately monitor the trends of the current epidemic and to maintain surveillance efforts and contribution to timely case detection and evidence-based interventions. Social mobilisation WHO and UNICEF have been working with MINSA, as part of participation of the Sub-Commission on Social Mobilisation, to develop public information messages and information for health care workers. The public awareness campaign has the following five objectives: To provide the general public with information about the disease, its symptoms and methods of prevention; To address the concerns and fears of health care workers; To disseminate information amongst children about the disease and actions they can take to ensure they and their families stay healthy; To address cultural customs of corpse management in order to reinforce the idea that the bodies of those affected by the disease must be immediately buried, omitting in such cases traditional funeral rites requiring contact with the body; To provide information on the management of suspected cases, empowering people with the knowledge of what to do if a suspected case is encountered. By the end of March, more than 500 activists were trained and mobilised to conduct an interpersonal, door-to-door campaign in the Province of Uige, aiming to ensure that essential messages about the disease and means of prevention reach all areas of the province, including remote and hard-to-reach regions. In addition, UNICEF and WHO are currently developing and producing communication materials including pamphlets, posters for use in health units, communiqués for distribution to the general public, TV and radio spots, stickers, and procuring megaphones for mobilisation teams. These materials will be distributed throughout the country's 18 provinces. A multi-media campaign is also being prepared, including five television spots in Portuguese and five radio spots, produced in Portuguese as well as eight of the country's most widely spoken indigenous languages. Logistics WHO, UNICEF and other UN agencies are supporting MINSA with procurement, information and logistics support to move existing supplies to Uige and other provinces as well as to develop IEC materials to alert and prepare all Provincial Departments of Health. UNICEF will continue to provide information on supplies, pricing and support to the Technical Sub-commission on Supply and Logistics to facilitate procurement by all partners and the distribution of supplies to the different provinces. In addition, UNICEF will compliment the logistics capacity provided by the Angolan military to provide supplies to Uige, by supporting distribution and delivery of supplies to the health centre level for the Ministry of Health in Uige and Luanda, as well as the other high-risk provinces. 3.1 Expected Results The primary objective of the Marburg VHF response is to successfully contain the spread of the virus, prevent further infection, and provide quality treatment and care to all infected individuals. Expected results include the following: MINSA human resource capacity is strengthened to facilitate early detection of and timely response to Marburg and other virus hemorrhagic fever outbreaks in Angola; MINSA coordination capacity is strengthened to ensure the early detection and timely response to Marburg and other virus hemorrhagic fever; Coordinated technical and operational support to MINSA from WHO, UNICEF, MSF and technical institutions in the areas of communicable disease surveillance and epidemic alert and response, especially for the control of Marburg, and to strengthen preparedness for other viral hemorrhagic fever outbreaks and emerging diseases. 7 MARBURG HEMORRHAGIC FEVER OUTBREAK RESPONSE 4. ADDITIONAL ROLES AND RESPONSIBILITIES WFP: WFP has joined efforts with WHO, UNICEF and other UN agencies and international and national organisations to assist in the control of the Marburg VHF epidemic in Uige and other high-risk provinces. WFP Air Passenger Services are providing transportation and critical logistics support to medical specialists and other essential staff working in Uige and elsewhere. WFP Air Services are also essential for the transportation of medical supplies, medicine, and equipment. WFP is currently considering the reintroduction of Air Services to additional locations, due to the refusal of some overland transporters to travel to parts of country, including Uige, affected by the outbreak. Because of these unforeseen activities, remaining limited resources for the Air Passenger Services are being used much faster than planned. For this reason, additional funding is urgently sought. CDC: Support for ELISA and RNA testing laboratory facilities in Luanda. MSF-Spain: Case Management in Uige Province and support of a mobile field laboratory. MSF-Holland: Support to MINSA in case management and coordination in Luanda. MSF-France: Mobilisation of emergency supplies and personnel to support all MSF operations in Angola. 8 MARBURG HEMORRHAGIC FEVER OUTBREAK RESPONSE ANNEX I. ACRONYMS AND ABBREVIATIONS AFRO Regional Office for Africa CDC CONGA Centres for Disease Control Consortium of NGOs in Angola DRC Democratic Republic of Congo ELISA Enzyme-linked immunosorbent assay FAA Armed Forces of Angola GOARN IEC IFRC Global Outbreak Alert and Response Network Information, Education, Communication International Federation of Red Cross and Red Crescent Societies MINSA MSF Ministry of Health Médecins Sans Frontières NGO Non-Governmental Organisation RNA Ribonucleic Acid UNICEF United Nations Children’s Fund VHF Viral Hemorrhagic Fever WFP WHO World Food Programme World Health Organization 9 OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS (OCHA) NEW YORK GENEVA OFFICE UNITED NATIONS PALAIS DES NATIONS NEW YORK, N.Y. 10017 1211 GENEVA 10 USA SWITZERLAND TELEFAX: (1 212) 963.3630 TELEFAX: (41 22) 917.0368