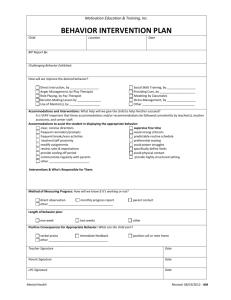
Structural Family Therapy
advertisement

Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Structural Family Therapy Assumptions Families are hierarchically organized with rules for interacting across and within subsystems. Insight is not sufficient for change. Normal developmental crises can create problems within a family. Inadequate hierarchy and boundaries maintain symptomatic behavior. Improving a subsystem’s boundary improves the functioning of the parts of the subsystem. Problems are a product of social relationships, e.g., they have a context. Families are evolving organizations continually regulating their internal structure in response to internal and external change. Developmental life demands change in the structure of the family, as well as rules and roles. Good functioning is determined by the fit of a family’s structure to its operational functions. Conflict is not to be avoided, but used for change. Family members develop a preferred degree of emotional proximity/distance in relating to one another. Structures and substructures are related. The individual is a subunit of her or his family as well as a subunit of other social contexts. Family members relate to each other in patterned ways that are observable. Family structure determines the effectiveness of family functioning. People are competent and resourceful, although interactional circumstances handicap competent functioning. A faulty structure prohibits movement through various stages (accomplishment of life tasks). Families are organized entities (developmentally and economically). Families are their own best resource for change. Family structure is defined by family transactional patterns (rules). Families inherently promote predictable organization (structure) for stability. Techniques Accommodation: A general term referring to the adjustments a therapist may make to a family (e.g., joining, maintenance, mimesis) in order to achieve a therapeutic alliance with the family). Boundary marking: A strategy in which the therapist reinforces appropriate boundaries and diffuses inappropriate boundaries by modifying transactional patterns (e.g., a therapist may sit between an intrusive mother and her child so that the mother will have difficulty speaking for the child). Creating a workable reality: A strategy in which the therapist attends to certain family issues, ignores others, and reframes still others to emphasize a family situation that has a solution. for example, a presenting problem of childhood schizophrenia may be de-emphasized, and the need for parental cooperation and control in the family may be emphasized. Thus a “workable reality” is created in which the parents have specific tasks to accomplish in relation to their “misbehaving” child. Enactment: The acting out of dysfunctional transactional patterns within the family therapy session, encouraged by the therapist. Through setting up these transactions in the present, the therapist learns much about the family’s structure and interactional patterns. The therapist is then able to intervene in 1 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. the process by increasing its intensity, indicating alternative transactions, marking boundaries, and so forth. The therapist may also have the family enact more positive transactional patterns within the therapy session, which will serve as a template for more positive interactions outside therapy. Intensity: The degree of impact of a therapeutic message, selectively regulated by the therapist. Intensity can be achieved by increasing the length of a transaction, or by frequently repeating the same message in different transactions. Intervening isomorphically: The therapist’s focusing on events that are dissimilar in content, but nevertheless are structurally equivalent. for example, whether an anorectic girl says she doesn’t know something, complains about the clothes she wears, or won’t eat, the therapist can reframe such statements as disrespect for her parents’ authority. Joining: An accommodating maneuver in which the therapist establishes rapport with family members and temporarily becomes part of the family system. The family accepts the therapist more openly, thus enhancing the therapist’s ability to being about change. Maintenance: An accommodation technique in which the therapist provides planned support of the family structure while he/she analyzes it. For example, comments like “I see,” “Tell me more about....,” and “Uh-huh” are noncommittal and give the therapist the time to understand the family better. Mimesis: The paralleling of a family’s mood or behavior, which solidifies a therapeutic alliance. For example, a therapist may talk slowly with a slow-talking family or be animated with an animated family. Restructuring: Any therapeutic intervention that confronts and challenges a family and facilitates structural changes. Examples of restructuring maneuvers include assigning tasks, shifting power systems, escalating stress, and marking boundaries. Unbalancing: Any therapeutic intervention that supports one member of the family, thus interfering with the homeostasis of the family system. from: Piercy, F. P., Sprenkle, D. H., and Associates. (1986). Family Therapy Sourcebook. New York: Guilford Press. Multisystemic Therapy TABLE 2.1 Treatment Principles Principle 1: The primary purpose of assessment is to understand the fit between the identified problems and their broader systemic context. Principle 2: Therapeutic contacts emphasize the positive and use systemic strengths as levers for change. Principle 3: Interventions are designed to promote responsible behavior and decrease irresponsible behavior among family members. 2 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Principle 4: Interventions are present focused and action oriented, targeting specific and well-defined problems. Principle 5: Interventions target sequences of behavior within and between multiple systems that maintain the identified problems. Principle 6: Interventions are developmentally appropriate and fit the developmental needs of the youth. Principle 7: Interventions are designed to require daily or weekly effort by family members. Principle 8: Intervention effectiveness is evaluated continuously from multiple perspectives with providers assuming accountability for overcoming barriers to successful outcomes. Principle 9: Interventions are designed to promote treatment generalization and long-term maintenance of therapeutic change by empowering caregivers to address family members' needs across multiple systemic contexts. 3 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. FAMILY NAME: Maggie STRENGTHS Individual: Athletic, enjoys sports. Attractive and likeable. Average intelligence. Takes care of siblings. Antisocial behavior limited to aggression. Cares deeply for her mother and wants things to be better at home and school. She responds well to praise. Family: Extended family lives close by and are concerned about M's behavior and home life. Grandmother and aunts willing to do "whatever it takes." mother is seriously concerned about her drug use and M's school and home behavior. Childrens basic needs are met by the mother-she is a survivor. Strong family bond. Peers: Prosocial peers in grandmother's neighborhood. School: Athletic programs. A counselor has a close relationship with Maggie and wants her to do well. Neighborhood Community: Several churches located. in the neighborhood. NEEDS Individual: History of school and community aggression. Physically fights mother. Victim of child sexual abuse. Family: Maternal crack cocaine dependence, Poor monitoring. High conflict, crowded living conditions. Low financial resources. Mother feels hopeless about changing her and M's behavior. Mother has minimal parenting skills. Family is socially isolated. Grandmother has cancer. Peers: Aggressive and antisocial. peers. Peers have little commitment to school. School: Limited resources. Policy of zero tolerance for threatening teachers. View behavior problems as moral flaw. Quick to expel students. Poor relationship to surrounding community. History of conflict with the family. Neighborhood/Community: Drug infested. Criminal subculture. minimal prosocial outlets. FIGURE 2.1. Initial contact sheet. 4 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. HYPOTHESIS DEVELOPMENT After obtaining the information needed to understand fit, the therapist in collaboration with the treatment team and clinical supervisor develops "testable" hypotheses based on the strengths and needs of the pertinent systems. Generally, hypothesis development takes the form of one element A, contributes to a second element B, for a person, C, under X conditions. HYPOTHESIS TESTING Generally, MST therapists test hypotheses by evaluating the effects of interventions derived from the hypotheses. As suggested above, for example, if the hypothesis is that mother-adolescent conflicts precipitate Maggie's aggression at home and school, the therapist would help the family to develop strategies to decrease the frequency of mother-daughter conflicts and then determine whether such changes led to decreased aggression. 5 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Principle 2: Therapeutic Contacts Emphasize the Positive and Use Systemic Strengths as Levers for Change The successful treatment of serious behavioral problems in children is contingent on engaging the family in treatment collaboration and developing a supportive therapeutic alliance. Focusing on family strengths: Sets the stage for cooperation and collaboration by decreasing the untoward effects of negative affect and builds feelings of hope and positive expectations, which are linked with favorable outcomes (Greenberg & Pinsof, 1986). Helps to identify protective factors (e.g., family resources and social supports) that lead to the development of better informed interventions and to solutions that have increased ecological validity and can be sustained by the family over time. Decreases therapist and family frustration by emphasizing problem solving (e.g., focusing on how desired changes can happen as opposed to why problems are so bad). Bolsters the caregiver's confidence, which is a prerequisite for empowerment. 6 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. DEVELOPING AND MAINTAINING A STRENGTH FOCUS The MST therapist and treatment team can take several straightforward steps to develop and maintain a strength focus. 1. Mandate that MST therapists, supervisors, and administrators use nonpejorative language in verbal (e.g., informal discussions, and group supervision) and written (e.g., Initial Contact Sheet and case summaries) communications. For example, clients are not viewed as "resistant" but as presenting a "challenge." When therapists have difficulty identifying positive aspects of the family, the treatment team should assist. 2. Teach and use techniques of refraining. For example, when Maggie's mother felt hopeless and overwhelmed and blamed herself for Maggie's difficulties, the therapist responded that the mother may or may not have caused Maggie's problems but she is certainly a critical part of the solution. 3. Use positive reinforcement liberally. The therapist should strive to find "evidence" of client effort and improvement and positively reinforce such, regardless of how small. For example, a client should be reinforced for attending sessions, giving his or her best, and so on. During the initial phase of treatment, Maggie's mother felt considerable apprehension, frustration, and hopelessness. The therapist reminded the mother that she was making important progress in helping her daughter by meeting with the therapist and helping to plan for changes. 4. Incorporate and maintain a problem-solving stance. A problem-solving stance emphasizes the examination of factors that can increase the probability of success as opposed to detailing what failed. For example, when barriers to success arise in treatment, the therapist, family, and MST treatment team should focus their attention on understanding the fit of the barrier, developing hypotheses, and testing the hypotheses by designing interventions to overcome the barrier. In Maggie's case, the mother's drug use was a constant barrier to treatment, and she refused to enter an intensive specialized treatment program for cocaine abuse. Instead of continuing to focus on the barrier presented by this refusal, the therapist took a different tack-enlisting the support of extended family to help serve as parental surrogates and attempting to identify and understand the events and situations leading up to and following the mother's cocaine use (i.e., closely examining the fit of the cocaine use). 5. Provide hope. Many families referred for MST are told repeatedly by family, friends, and social service professionals "how bad things are" for the child and family. To counter this pessimistic stance, the therapist should, through optimism and a "can do" attitude, engender hope among family members and attempt to energize the family and key members of their social ecology to effect change. 7 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. 6. Find and emphasize what the family does well. The therapist should focus on identifying and encouraging what the family does well. To facilitate this process, breaking large, seemingly insurmountable tasks into small steps is often useful. With Maggie and her mother, for example, the therapist helped to set small, "achievable" daily homework assignments and goals (e.g., saying hello to one another when Maggie got home from school and getting Maggie's homework to grandmother to be checked). These goals were designed to provide incremental progress toward the larger goals of treatment. PARENTAL RESPONSIBLE AND IRRESPONSIBLE BEHAVIOR Parents have several interrelated responsibilities that are linked with the favorable development, socialization, and well-being of their children. These responsibilities include providing for basic needs, nurturance, protection, advocacy, support, guidance, and discipline (Small, 1990). From an MST perspective, responsible parents engage in behaviors that prepare their children to become competent members of society. Principle 4: Interventions Are Present Focused and Action Oriented, Targeting Specific and Well-Defined Problems The overall purpose of this treatment principle is to encourage family transactions that are facilitating clinical progress toward unambiguous outcomes. PRESENT FOCUSED MST interventions emphasize changing the family's present circumstances as a step toward changing future functioning. Such an approach contrasts with treatment models that devote a great deal of attention to examining the client's or family's past (e.g., psychoanalysis and Bowenian family therapy). ACTION ORIENTED In light of the serious nature of the problems presented by youth and families referred for MST, interventions aim to activate the family and their social ecology to make multiple, positive, observable changes. Making and sustaining such changes requires a high-energy and action-oriented focus. TARGETING SPECIFIC AND WELL-DEFINED PROBLEMS Two types of well-specified treatment goals are used within MST-overarching goals and intermediate goals. Overarching goals refer to the family's ultimate aims by the end of treatment (e.g., have the youth pass to the 10th grade). Intermediate goals refer to the daily nuts and bolts of reaching the overarching goals (e.g., completing homework assignments each evening, studying for exams, parental reward for academic efforts, and linking parents and school to support educational efforts), and development of the intermediate goals is usually led by the therapist. 8 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Principle 5: Interventions Target Sequences of Behavior within and between Multiple Systems that Maintain the Identified Problems This principle orients the practitioner toward modifying those aspects of family relations and of the social ecology that are linked with identified problems. Principle 6: Interventions Are Developmentally Appropriate and Fit the Developmental Needs of the Youth Children and their caregivers have different needs at different periods of their lives, and interventions should be designed in consideration of such. For example, the nature of family-based interventions will vary with the developmental level of the youth as well as the developmental stage of the caregiver. Principle 7: Interventions Are Designed to Require Daily or Weekly Effort by Family Members A basic assumption of MST is that therapists can help families resolve their problems more quickly if everyone involved (e.g., caregivers, extended family, siblings, friends, neighbors, and social service personnel) works together diligently. This assumption is predicated on the family and therapist agreeing on and collaborating with the goals of treatment. Designing interventions that require daily and weekly effort provides several advantages. 1. Identified problems can be resolved more quickly if everyone involved is working on them. 2. Backsliding and nonadherence to treatment protocols become readily apparent. Consequently, therapists can respond immediately to identify and address barriers to change. 3. Treatment outcomes can be assessed continually, which provides many opportunities for corrective actions. 4. Because intervention tasks occur daily, family members have frequent opportunity to receive positive feedback in moving toward goals, praise from therapist and others in the ecology, and satisfaction inherent in completing tasks. Such reinforcers promote family motivation and maintenance of change. 5. Family empowerment is supported as families learn that they are primarily responsible for and capable of progressing toward treatment goals. 9 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Principle 9: Interventions Are Designed to Promote Treatment Generalization and Long-Term Maintenance of Therapeutic Change by Empowering Caregivers to Address Family Members' Needs across Multiple Systemic Contexts Ensuring that treatment gains will generalize and be maintained when treatment ends is a critical and continuous thrust of MST interventions. Therapeutic interventions should do the following: 1. Emphasize the development of skills that family members will use to navigate their social ecology. 2. Develop the capacity of family members to negotiate current and future problems. 3. Be delivered primarily by caregivers, with therapists playing primarily supportive and consultative roles. 4. Accentuate and build family strengths and competencies. 5. Make abundant use of protective and resiliency factors available in the natural environment. EMPOWERMENT Empowering clients requires MST therapists to possess at least three attitudes or characteristics. First, therapists must restrain themselves from entering the family system and affecting change through the force of their own personalities and skills. Instead, MST therapists must maximize the capacity of family members to affect changes in their own lives. Practitioners, therefore, should demonstrate "benevolent demanding" (Linehan, 1993), which recognizes the client's existing capacities, reinforces adaptive behavior and self-control, and refuses to take care of clients when they can care for themselves. Second, MST therapists must recognize that families are composed of autonomous individuals with the right to decide what they do and what happens to them. Families have a right to choose the goals of treatment and clinicians must respect their choices. A corollary of this second point is that MST therapists must assume families have competencies when given appropriate opportunities and resources. Third, MST therapists must be creative in finding indigenous resources for families to use in gaining control over their lives. As suggested next and discussed in Chapter 8, priority is clearly given to the development of natural resources (i.e., friends, neighbors, and extended family) versus agency resources (i.e., case managers). These resources must be in place by the time MST treatment is terminated. 10 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. DESIGNING INTERVENTIONS FOR GENERALIZATION AND MAINTENANCE Therapists can increase the probability of treatment generalization and maintenance by taking several straightforward steps. Teach relevant behaviors or skills in the environments and under the conditions in which clients will eventually behave. For example, the therapist taught Maggie's mother behavior management techniques at home and had her use the skills as she was consequating Maggie's behavior after school. 1. Encourage and reinforce the development of problem-solving skills. Reinforce families for (or their efforts toward) identifying problems (i.e., well-defined and specified), generating alternative solutions, evaluating solutions, analyzing possible barriers to solutions, choosing an alternative, and preparing for possible consequences of the solution. 2. Find individuals in the ecology who can and will reinforce family members'new behaviors and skills across settings (e.g., home, school, and community). 3. Alert significant others (e.g., teachers, probation officers, and case managers) to the new behaviors of the family members. 4. Provide positive reinforcement when generalization occurs. For example, the therapist taught the mother to reinforce Maggie when she exhibited "respectful behavior" to siblings and peers, not just to adults. 6. Allow clients to do as much of the development and implementation of interventions as they can. 11 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Providing MST via the Home-Based Model of Service Delivery Low caseloads, typically three to six families per full-time therapist. Provision of services in the family's natural environment-home, school, and neighborhood settings. Time-limited duration of treatment, 3-5 months per family depending on the seriousness of the problems and success of interventions. Therapist functioning within a team of three to four practitioners, though each has an individual caseload. 24-hour-per-day and 7-day-per-week availability of therapists, or at least one practitioner on the MST team. Scheduling appointments at the family's convenience, such as evening hours and weekends. Daily contact, face to face or by phone, with families. 12 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Assessment of Family Functioning Multisystemic conceptualizations of effective family functioning are guided by social-ecological and family systems theories and by research on child development, developmental psychopathology, parenting practices, marital relations, and individual parent and child characteristics associated with positive and negative outcomes for youth. Effective Family Functioning The Family as a System The MST perspective on effective family functioning embodies systems theories and the assumptions of multicausality and reciprocity of interactions that characterize these theories. Thus, the behavioral and psychological functioning of all family members is understood in terms of ongoing and repetitive patterns of family transactions rather than in terms of unidirectional and linear interpersonal or intrapsychic processes. Family problems are seen as both affecting and being affected by how the family interacts as a whole. Consistent with pragmatic (i.e., focused on changing behavior in the present) as versus esthetic models of the family and family therapy (see Alexander, HoltzworthMunroe, & Jameson, 1994; Henggeler, Borduin, & Mann, 1993), MST family interventions aim to change the everyday patterns of interaction thought to sustain the identified problems. The present-focused and solution-oriented nature of MST is particularly consonant with structural (S. Minuchin, 1974) and strategic (Haley, 1976) models of family therapy. Structural family therapy The structural model conceptualizes the family in terms of marital, parental, and sibling subsystems that are constructed along generational and role lines. Each subsystem has boundaries such that all family members do not have equal access to the subsystem. Boundaries should be flexible, however, to facilitate the capacity of the family system to respond to the needs of individual family members or to environmental demands. The structural model views child emotional and behavioral problems as signs that subsystem boundaries are too weak or too strong. Terms such as enmeshment and disengagement describe family interaction patterns in which boundaries are excessively porous or rigid. Porous boundaries, for example, can fail to promote the emancipation and independent achievements of children; rigid boundaries can limit the family's capacity to respond to environmental stress and meet the affective needs of family members. Constructs such as triangulation and parent-child coalition describe transactional patterns that confuse parent-child and spousal boundaries, often in ways that involve the child in the negotiation of adult subsystem conflict. Treatment-related changes in these patterns are associated with improvements in the antisocial behavior of adolescents (Mann, Borduin, Henggeler, & Blaske, 1990). 13 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Strategic family therapy Strategic formulations also inform the MST clinician's assessment of family functioning. To design interventions that effectively address interactions within and between systems (Principle 5), the MST practitioner undertakes assessment of the "recursive sequences of behavior" (Haley, 1976) associated with an identified problem. The strategic family therapy tenet that emotional and behavioral problems are intimately linked with recurrent sequences of family interactions is consistent with research on the etiology of childhood aggression and conduct disorder. This research identifies predictable and repetitive cycles of aversive interaction between parents and children and among siblings as contributing factors in the development of antisocial behavior (Patterson, 1982; Patterson & Reid, 1984). The Parent-Child Subsystem Family systems constructs can render the complexity of interactions among multiple family members understandable and predictable, and, therefore, alterable. System principles do not, however, address the central issues and topics around which family interactions occur, namely power/control and affection/intimacy. WARMTH The warmth dimension of parent-child relations reflects verbal and nonverbal behaviors that are emotional in tone, ranging from warmth to rejection. CONTROL Parental control strategies have several important functions in child development. They teach the child frustration tolerance, which is essential to the development of successful interpersonal relations. Control strategies also teach the child socially acceptable norms of behavior, including the avoidance of aggression, cooperation with others, and respect for authority. 14 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. PARENTING STYLE Authoritative parents are responsive to the reasonable needs and desires of the child but also make maturity demands appropriate to the child's stage of development. Parents have clear and well-defined expectations and rules regarding the child's school performance, participation in household chores, and interpersonal behavior with family members, peers, and adults and authority figures outside the home (teachers, other relatives, neighbors, coaches, etc.). Authoritative parenting is associated with a range of positive outcomes, such as positive academic achievement, social responsibility, and positive peer relationships. Authoritarian (high control, low warmth) parents are directive and overcontrolling, and require that children have an unquestioning obedience to parental authority. When a child deviates from parental rules, punishment tends to be severe and is often physical. When teaching the child new skills, behaviors, or tasks, the authoritarian parent is directive, giving direct verbal orders and often physically taking over the activity being taught. Thus, the parent's responsiveness to the child's needs is often overridden by his or her efforts to direct or control those situations. Authoritarian parents also fail to make appropriate maturity demands. By rigidly prescribing child behavior, the child rarely participates in making choices and decisions and therefore has little opportunity to grapple with the consequences of his or her own choices and decisions (Baumrind, 1989). Authoritarian parenting is linked to child aggression, social withdrawal from peers, poor self-confidence, and internalized distress (Baunuind, 1989; Steinberg et al., 1994) as well as continuity of such patterns into adolescence (Baunnind, 199 1; Lamborn, Mounts, Steinberg, & Dornbusch, 1991; Steinberg et al., 1994). Pennissive (high warmth, low control) parents provide their children with little structure and discipline, make few demands for mature behavior, and tolerate even those impulses in children that meet with societal disapproval. Permissive parents are typically warm and responsive but not demanding. Permissive parenting is associated with aggression (Olweus, 1980), impulsivity, and a lack of social responsibility and independence in children (Baumrind, 1989, 1991) and with school misconduct, drug and alcohol use, and heightened orientation toward and value of peer activities and norms in adolescents (Baumrind, 1991; Steinberg et al., 1994). Neglectjul (low warmth, low control) parents offer little affection or discipline to their children and appear to have little concern for or interest in parenting. That is, neglectful parents are neither responsive to the reasonable needs and desires of the youth nor demanding of responsible, age-appropriate behavior with respect to tasks or interpersonal relationships. Of the four parenting types, neglectful parenting is most strongly related to children's distress. Children from neglectful homes are characterized by poorer adjustment on many indices of functioning than children from permissive or authoritarian homes, and this negative trajectory continues through adolescence, when neglectful parenting is associated with sizable increases in adolescent delinquency and drug use (Steinberg et al., 1994). 15 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. The Marital Subsystem In families headed by two married adults, the marital relationship is the foundation of the family system. INTIMACY AND POWER Just as the major dimensions of parent-child interactions are warmth and control, so the major dimensions of marital interactions reflect intimacy and power (Emery, 1992, 1994). Intimacy refers to the strength of the emotional bond between adults, and a positive emotional bond is important to the longevity of intimate relationships. CONFLICT Research indicates that conflict between parents is associated with a host of problems in children and families, including externalizing problems, childhood aggression (particularly in boys), depression in mothers, inconsistent parenting practices, and increased parent-child conflict (for reviews, see Cummings & Davies, 1994; Grych & Fincham, 1992). The frequency and intensity of conflict and the presence of both verbal and physical conflict (Fantuzzo et al., 1991; Vissing, Strauss, Gelles, & Harrop, 1991) are associated with higher levels of evels of conduct problems in youth. Several mechanisms may account for the association between marital conflict and child behavioral problems. Marital problems may be linked with behavioral problems because the resulting emotional distress interferes with parental responsiveness to children's needs, marital conflicts interfere with parents' abilities to deliver consistent discipline, parents in conflict may be modeling poor conflict-resolution skills, and the emotionally charged environment may be stressful to children. 16 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Family System Transitions: Divorced, Remarried, and Single-Parent Families The fact that divorce is often followed by remarriage and/or living in a singleparent family means that many children experience more than one set of the multiple and sometimes difficult transitions (Cherlin, 1992) described next. DIVORCED FAMILIES Longitudinal research indicates that divorce is a developmental process during which a series of "partially predictable events" often occurs (Emery, 1994, p. 17). REMARRIED FAMILIES As with divorce, research on the reconstitution of families through marriage supports a developmental, family systems perspective (Hetherington & Clingempeel, 1992). Remarriage requires renegotiation of relationships, roles, and boundaries among all members of the two families coming together to form a new family group. SINGLE-PARENT FAMILIES Many families headed by a single parent function effectively to meet the instrumental and affective needs of the children and the parent. In some families, the responsibilities of childrearing are supported by, or shared with, another family member such as a grandparent or another relative. KIN AS PARENT FIGURES In a significant percentage of families with a youth presenting serious antisocial behavior, grandparents or other relatives are the surrogate parents, often assuming guardianship, if not legal custody, of the youth. In some of these cases, surrogate parents had substantial involvement with the youth prior to assuming primary parenting responsibility. 17 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Assessing Family Functioning Assessment of family functioning is an ongoing process initiated when the practitioner first meets the family and refined throughout treatment as interventions are implemented and their effects are observed. Together, the practitioner and family members observe and try to tease out the specific family interactions that are the most powerful, proximal predictors of the identified problems. Throughout this process, practitioners do the following: I. Develop hypotheses (e.g., explanations, hunches, or beliefs a practitioner or family member develops regarding the possible causes of the referral problem) regarding the relative contributions of familial factors to problem behaviors. Consistent with MST Principles 4 and 5 (present focused, targeting specific, well-defined problems; targeting sequences of behavior within or between multiple systems), hypotheses focus primarily on observable interactions and behaviors. 2. Gather evidence (i.e., information that was observed, self-reported, or concretely monitored, such as checklists, charts, check-in phone calls by the parent, other family members, school personnel, neighbors, etc., and the practitioner) to support or refute those hypotheses. 3. Implement interventions that target the hypothesized contributing factors. 4. Observe whether the interventions result in changes in problem behaviors. 5. Identify barriers to intervention success. 6. Design interventions to overcome these barriers. These steps are part of the iterative process of MST case conceptualization and intervention implementation depicted in Figure 2.2 of Chapter 2. 18 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Family-School Linkage Parents' involvement in their children's schooling is an important determinant of academic achievement and psychosocial functioning in school. Therapists should assess, therefore, such parental involvement in school-related activities as the following: Monitoring homework assignments and exam grades. Setting aside a block of time and a quiet place for the child to study after school. Supporting extracurricular school functions. Implementing contingencies that are based on the child's efforts and performance. Providing overt support for teachers' educational demands, behavioral demands, and goals. PARENTAL ATTITUDES TOWARD EDUCATION Youth academic and behavioral problems can be exacerbated when academic success is not a high priority for the parents. PARENT-SCHOOL CONFLICT Children's school performance usually suffers when conflicts develop between parents and school personnel. Such conflict can be linked with several circumstances, including the following: Miscommunications that can occur when parents and educators are of disparate sociocultural backgrounds (e.g., parents might feel intimidated by or resentful of the educators). Perceived insults or "putdowns" based on previous interactions between the parents and school personnel. The youth playing the parent off against the school (e.g., convinces his parents that the teacher does not like him and is discriminating against him). Parental perceptions that the school is not committed to meeting the needs of the youth. The perception of school personnel that the parent has little concern for the youth's performance or behavior in school. 19 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. The goals of the meeting between the therapist, parents, and school personnel, therefore, are to do the following: 1 . Clarify that all parties have the youth's best interest at heart. 2. Explain the rationale (i.e., fit) of the proposed interventions to all parties. 3. Provide an opportunity to revise the proposed interventions, pending additional input from school personnel (assuming that any revisions are approved by the parents and therapist). 4. Delineate the exact responsibilities of each party vis-a-vis the interventions, with the parents assuming the bulk of the responsibility. 5. Develop a system for monitoring implementation and outcome of the interventions. 6. Develop a system for providing all parties with feedback regarding the outcomes. 7. Delineate strategies for revising the school-related intervention protocol, with the parents and therapists taking responsibility for such. 20 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. When and How to Conduct Individually Oriented Interventions In our experience, team (i.e., practitioner and clinical supervisor) decisions to pursue individual treatment with parent figures most often (1) pertain to problems that interfere with parental functioning, such as depression, anxiety disorders, and substance abuse; and (2) are made at two "ends" of the MST treatment period. These two ends are: 1. Early in treatment, if the parent figure's functioning is compromised so frequently or to such an extent that the practitioner is unable to develop a working alliance, identify the parent's treatment goals, or engage the parent in making even minor changes toward a goal he or she has identified as important. 2. Well into treatment, when interventions targeting intrafamilial (parent-child, marital, kin) or extrafamilial (family-school, peer, neighborhood) interactions have been implemented inconsistently or implemented with poor results, and specific aspects of the parent's functioning are identified as critical barriers to implementation or success. With respect to adolescents, four types of situations can warrant the implementation of individual interventions. These are: When a youth continues to display serious aggressive or impulsive behaviors in one or more contexts (e.g., in the classroom, with certain peers, and with siblings) after systemic interventions have been consistently implemented by parents, teachers, and other relevant players in the youth's natural ecology. 1. When a youth with biologically influenced difficulties (e.g., ADHD, bipolar disorder, or clinical depression) is consistently taking appropriately prescribed medication and well-implemented ecological interventions are in place, yet, problems with impulsive or aggressive behavior continue to occur at home, in school, or with peers. 2. When the sequelae of victimization (i.e., physical abuse, sexual abuse, and criminal victimization) contribute to referral problems. 3. When intensive and comprehensive efforts to engage caregivers in changing parenting practices or other aspects of the youth's ecology are unsuccessful, efforts to overcome barriers to change are unsuccessful, and the adolescent will continue to live in a home in which the lack of favorable clinical change will exacerbate the identified problems. FAMILY NAME: Maggie STRENGTHS Individual: Athletic, enjoys sports. Attractive and likeable. Average intelligence. Takes care of siblings. Antisocial behavior limited to aggression. Cares deeply for her mother and wants things to be better at home and school. She responds well to praise. 21 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Family: Extended family lives close by and are concerned about M's behavior and home life. Grandmother and aunts willing to do "whatever it takes." mother is seriously concerned about her drug use and M's school and home behavior. Childrens basic needs are met by the mother-she is a survivor. Strong family bond. Peers: Prosocial peers in grandmother's neighborhood. School: Athletic programs. A counselor has a close relationship with Maggie and wants her to do well. Neighborhood Community: Several churches located. in the neighborhood. NEEDS Individual: History of school and community aggression. Physically fights mother. Victim of child sexual abuse. Family: Maternal crack cocaine dependence, Poor monitoring. High conflict, crowded living conditions. Low financial resources. Mother feels hopeless about changing her and M's behavior. Mother has minimal parenting skills. Family is socially isolated. Grandmother has cancer. Peers: Aggressive and antisocial. peers. Peers have little commitment to school. School: Limited resources. Policy of zero tolerance for threatening teachers. View behavior problems as moral flaw. Quick to expel students. Poor relationship to surrounding community. History of conflict with the family. Neighborhood/Community: Drug infested. Criminal subculture. minimal prosocial outlets. FIGURE 2.1. Initial contact sheet. 22 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. HYPOTHESIS DEVELOPMENT After obtaining the information needed to understand fit, the therapist in collaboration with the treatment team and clinical supervisor develops "testable" hypotheses based on the strengths and needs of the pertinent systems. Generally, hypothesis development takes the form of one element A, contributes to a second element B, for a person, C, under X conditions. HYPOTHESIS TESTING Generally, MST therapists test hypotheses by evaluating the effects of interventions derived from the hypotheses. As suggested above, for example, if the hypothesis is that mother-adolescent conflicts precipitate Maggie's aggression at home and school, the therapist would help the family to develop strategies to decrease the frequency of mother-daughter conflicts and then determine whether such changes led to decreased aggression. 23 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Principle 2: Therapeutic Contacts Emphasize the Positive and Use Systemic Strengths as Levers for Change The successful treatment of serious behavioral problems in children is contingent on engaging the family in treatment collaboration and developing a supportive therapeutic alliance. Focusing on family strengths: Sets the stage for cooperation and collaboration by decreasing the untoward effects of negative affect and builds feelings of hope and positive expectations, which are linked with favorable outcomes (Greenberg & Pinsof, 1986). Helps to identify protective factors (e.g., family resources and social supports) that lead to the development of better informed interventions and to solutions that have increased ecological validity and can be sustained by the family over time. Decreases therapist and family frustration by emphasizing problem solving (e.g., focusing on how desired changes can happen as opposed to why problems are so bad). Bolsters the caregiver's confidence, which is a prerequisite for empowerment. 24 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. DEVELOPING AND MAINTAINING A STRENGTH FOCUS The MST therapist and treatment team can take several straightforward steps to develop and maintain a strength focus. 1. Mandate that MST therapists, supervisors, and administrators use nonpejorative language in verbal (e.g., informal discussions, and group supervision) and written (e.g., Initial Contact Sheet and case summaries) communications. For example, clients are not viewed as "resistant" but as presenting a "challenge." When therapists have difficulty identifying positive aspects of the family, the treatment team should assist. 2. Teach and use techniques of refraining. For example, when Maggie's mother felt hopeless and overwhelmed and blamed herself for Maggie's difficulties, the therapist responded that the mother may or may not have caused Maggie's problems but she is certainly a critical part of the solution. 3. Use positive reinforcement liberally. The therapist should strive to find "evidence" of client effort and improvement and positively reinforce such, regardless of how small. For example, a client should be reinforced for attending sessions, giving his or her best, and so on. During the initial phase of treatment, Maggie's mother felt considerable apprehension, frustration, and hopelessness. The therapist reminded the mother that she was making important progress in helping her daughter by meeting with the therapist and helping to plan for changes. 4. Incorporate and maintain a problem-solving stance. A problem-solving stance emphasizes the examination of factors that can increase the probability of success as opposed to detailing what failed. For example, when barriers to success arise in treatment, the therapist, family, and MST treatment team should focus their attention on understanding the fit of the barrier, developing hypotheses, and testing the hypotheses by designing interventions to overcome the barrier. In Maggie's case, the mother's drug use was a constant barrier to treatment, and she refused to enter an intensive specialized treatment program for cocaine abuse. Instead of continuing to focus on the barrier presented by this refusal, the therapist took a different tack-enlisting the support of extended family to help serve as parental surrogates and attempting to identify and understand the events and situations leading up to and following the mother's cocaine use (i.e., closely examining the fit of the cocaine use). 5. Provide hope. Many families referred for MST are told repeatedly by family, friends, and social service professionals "how bad things are" for the child and family. To counter this pessimistic stance, the therapist should, through optimism and a "can do" attitude, engender hope among family members and attempt to energize the family and key members of their social ecology to effect change. 25 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. 6. Find and emphasize what the family does well. The therapist should focus on identifying and encouraging what the family does well. To facilitate this process, breaking large, seemingly insurmountable tasks into small steps is often useful. With Maggie and her mother, for example, the therapist helped to set small, "achievable" daily homework assignments and goals (e.g., saying hello to one another when Maggie got home from school and getting Maggie's homework to grandmother to be checked). These goals were designed to provide incremental progress toward the larger goals of treatment. PARENTAL RESPONSIBLE AND IRRESPONSIBLE BEHAVIOR Parents have several interrelated responsibilities that are linked with the favorable development, socialization, and well-being of their children. These responsibilities include providing for basic needs, nurturance, protection, advocacy, support, guidance, and discipline (Small, 1990). From an MST perspective, responsible parents engage in behaviors that prepare their children to become competent members of society. Principle 4: Interventions Are Present Focused and Action Oriented, Targeting Specific and Well-Defined Problems The overall purpose of this treatment principle is to encourage family transactions that are facilitating clinical progress toward unambiguous outcomes. PRESENT FOCUSED MST interventions emphasize changing the family's present circumstances as a step toward changing future functioning. Such an approach contrasts with treatment models that devote a great deal of attention to examining the client's or family's past (e.g., psychoanalysis and Bowenian family therapy). ACTION ORIENTED In light of the serious nature of the problems presented by youth and families referred for MST, interventions aim to activate the family and their social ecology to make multiple, positive, observable changes. Making and sustaining such changes requires a high-energy and action-oriented focus. TARGETING SPECIFIC AND WELL-DEFINED PROBLEMS Two types of well-specified treatment goals are used within MST-overarching goals and intermediate goals. Overarching goals refer to the family's ultimate aims by the end of treatment (e.g., have the youth pass to the 10th grade). Intermediate goals refer to the daily nuts and bolts of reaching the overarching goals (e.g., completing homework assignments each evening, studying for exams, parental reward for academic efforts, and linking parents and school to support educational efforts), and development of the intermediate goals is usually led by the therapist. 26 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Principle 5: Interventions Target Sequences of Behavior within and between Multiple Systems that Maintain the Identified Problems This principle orients the practitioner toward modifying those aspects of family relations and of the social ecology that are linked with identified problems. Principle 6: Interventions Are Developmentally Appropriate and Fit the Developmental Needs of the Youth Children and their caregivers have different needs at different periods of their lives, and interventions should be designed in consideration of such. For example, the nature of family-based interventions will vary with the developmental level of the youth as well as the developmental stage of the caregiver. Principle 7: Interventions Are Designed to Require Daily or Weekly Effort by Family Members A basic assumption of MST is that therapists can help families resolve their problems more quickly if everyone involved (e.g., caregivers, extended family, siblings, friends, neighbors, and social service personnel) works together diligently. This assumption is predicated on the family and therapist agreeing on and collaborating with the goals of treatment. Designing interventions that require daily and weekly effort provides several advantages. 1. Identified problems can be resolved more quickly if everyone involved is working on them. 2. Backsliding and nonadherence to treatment protocols become readily apparent. Consequently, therapists can respond immediately to identify and address barriers to change. 3. Treatment outcomes can be assessed continually, which provides many opportunities for corrective actions. 4. Because intervention tasks occur daily, family members have frequent opportunity to receive positive feedback in moving toward goals, praise from therapist and others in the ecology, and satisfaction inherent in completing tasks. Such reinforcers promote family motivation and maintenance of change. 5. Family empowerment is supported as families learn that they are primarily responsible for and capable of progressing toward treatment goals. 27 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Principle 9: Interventions Are Designed to Promote Treatment Generalization and Long-Term Maintenance of Therapeutic Change by Empowering Caregivers to Address Family Members' Needs across Multiple Systemic Contexts Ensuring that treatment gains will generalize and be maintained when treatment ends is a critical and continuous thrust of MST interventions. Therapeutic interventions should do the following: 1. Emphasize the development of skills that family members will use to navigate their social ecology. 2. Develop the capacity of family members to negotiate current and future problems. 3. Be delivered primarily by caregivers, with therapists playing primarily supportive and consultative roles. 4. Accentuate and build family strengths and competencies. 5. Make abundant use of protective and resiliency factors available in the natural environment. EMPOWERMENT Empowering clients requires MST therapists to possess at least three attitudes or characteristics. First, therapists must restrain themselves from entering the family system and affecting change through the force of their own personalities and skills. Instead, MST therapists must maximize the capacity of family members to affect changes in their own lives. Practitioners, therefore, should demonstrate "benevolent demanding" (Linehan, 1993), which recognizes the client's existing capacities, reinforces adaptive behavior and self-control, and refuses to take care of clients when they can care for themselves. Second, MST therapists must recognize that families are composed of autonomous individuals with the right to decide what they do and what happens to them. Families have a right to choose the goals of treatment and clinicians must respect their choices. A corollary of this second point is that MST therapists must assume families have competencies when given appropriate opportunities and resources. Third, MST therapists must be creative in finding indigenous resources for families to use in gaining control over their lives. As suggested next and discussed in Chapter 8, priority is clearly given to the development of natural resources (i.e., friends, neighbors, and extended family) versus agency resources (i.e., case managers). These resources must be in place by the time MST treatment is terminated. 28 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. DESIGNING INTERVENTIONS FOR GENERALIZATION AND MAINTENANCE Therapists can increase the probability of treatment generalization and maintenance by taking several straightforward steps. Teach relevant behaviors or skills in the environments and under the conditions in which clients will eventually behave. For example, the therapist taught Maggie's mother behavior management techniques at home and had her use the skills as she was consequating Maggie's behavior after school. 5. Encourage and reinforce the development of problem-solving skills. Reinforce families for (or their efforts toward) identifying problems (i.e., well-defined and specified), generating alternative solutions, evaluating solutions, analyzing possible barriers to solutions, choosing an alternative, and preparing for possible consequences of the solution. 6. Find individuals in the ecology who can and will reinforce family members'new behaviors and skills across settings (e.g., home, school, and community). 7. Alert significant others (e.g., teachers, probation officers, and case managers) to the new behaviors of the family members. 8. Provide positive reinforcement when generalization occurs. For example, the therapist taught the mother to reinforce Maggie when she exhibited "respectful behavior" to siblings and peers, not just to adults. 6. Allow clients to do as much of the development and implementation of interventions as they can. 29 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Providing MST via the Home-Based Model of Service Delivery Low caseloads, typically three to six families per full-time therapist. Provision of services in the family's natural environment-home, school, and neighborhood settings. Time-limited duration of treatment, 3-5 months per family depending on the seriousness of the problems and success of interventions. Therapist functioning within a team of three to four practitioners, though each has an individual caseload. 24-hour-per-day and 7-day-per-week availability of therapists, or at least one practitioner on the MST team. Scheduling appointments at the family's convenience, such as evening hours and weekends. Daily contact, face to face or by phone, with families. 30 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Assessment of Family Functioning Multisystemic conceptualizations of effective family functioning are guided by social-ecological and family systems theories and by research on child development, developmental psychopathology, parenting practices, marital relations, and individual parent and child characteristics associated with positive and negative outcomes for youth. Effective Family Functioning The Family as a System The MST perspective on effective family functioning embodies systems theories and the assumptions of multicausality and reciprocity of interactions that characterize these theories. Thus, the behavioral and psychological functioning of all family members is understood in terms of ongoing and repetitive patterns of family transactions rather than in terms of unidirectional and linear interpersonal or intrapsychic processes. Family problems are seen as both affecting and being affected by how the family interacts as a whole. Consistent with pragmatic (i.e., focused on changing behavior in the present) as versus esthetic models of the family and family therapy (see Alexander, HoltzworthMunroe, & Jameson, 1994; Henggeler, Borduin, & Mann, 1993), MST family interventions aim to change the everyday patterns of interaction thought to sustain the identified problems. The present-focused and solution-oriented nature of MST is particularly consonant with structural (S. Minuchin, 1974) and strategic (Haley, 1976) models of family therapy. Structural family therapy The structural model conceptualizes the family in terms of marital, parental, and sibling subsystems that are constructed along generational and role lines. Each subsystem has boundaries such that all family members do not have equal access to the subsystem. Boundaries should be flexible, however, to facilitate the capacity of the family system to respond to the needs of individual family members or to environmental demands. The structural model views child emotional and behavioral problems as signs that subsystem boundaries are too weak or too strong. Terms such as enmeshment and disengagement describe family interaction patterns in which boundaries are excessively porous or rigid. Porous boundaries, for example, can fail to promote the emancipation and independent achievements of children; rigid boundaries can limit the family's capacity to respond to environmental stress and meet the affective needs of family members. Constructs such as triangulation and parent-child coalition describe transactional patterns that confuse parent-child and spousal boundaries, often in ways that involve the child in the negotiation of adult subsystem conflict. Treatment-related changes in these patterns are associated with improvements in the antisocial behavior of adolescents (Mann, Borduin, Henggeler, & Blaske, 1990). 31 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Strategic family therapy Strategic formulations also inform the MST clinician's assessment of family functioning. To design interventions that effectively address interactions within and between systems (Principle 5), the MST practitioner undertakes assessment of the "recursive sequences of behavior" (Haley, 1976) associated with an identified problem. The strategic family therapy tenet that emotional and behavioral problems are intimately linked with recurrent sequences of family interactions is consistent with research on the etiology of childhood aggression and conduct disorder. This research identifies predictable and repetitive cycles of aversive interaction between parents and children and among siblings as contributing factors in the development of antisocial behavior (Patterson, 1982; Patterson & Reid, 1984). The Parent-Child Subsystem Family systems constructs can render the complexity of interactions among multiple family members understandable and predictable, and, therefore, alterable. System principles do not, however, address the central issues and topics around which family interactions occur, namely power/control and affection/intimacy. WARMTH The warmth dimension of parent-child relations reflects verbal and nonverbal behaviors that are emotional in tone, ranging from warmth to rejection. CONTROL Parental control strategies have several important functions in child development. They teach the child frustration tolerance, which is essential to the development of successful interpersonal relations. Control strategies also teach the child socially acceptable norms of behavior, including the avoidance of aggression, cooperation with others, and respect for authority. 32 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. PARENTING STYLE Authoritative parents are responsive to the reasonable needs and desires of the child but also make maturity demands appropriate to the child's stage of development. Parents have clear and well-defined expectations and rules regarding the child's school performance, participation in household chores, and interpersonal behavior with family members, peers, and adults and authority figures outside the home (teachers, other relatives, neighbors, coaches, etc.). Authoritative parenting is associated with a range of positive outcomes, such as positive academic achievement, social responsibility, and positive peer relationships. Authoritarian (high control, low warmth) parents are directive and overcontrolling, and require that children have an unquestioning obedience to parental authority. When a child deviates from parental rules, punishment tends to be severe and is often physical. When teaching the child new skills, behaviors, or tasks, the authoritarian parent is directive, giving direct verbal orders and often physically taking over the activity being taught. Thus, the parent's responsiveness to the child's needs is often overridden by his or her efforts to direct or control those situations. Authoritarian parents also fail to make appropriate maturity demands. By rigidly prescribing child behavior, the child rarely participates in making choices and decisions and therefore has little opportunity to grapple with the consequences of his or her own choices and decisions (Baumrind, 1989). Authoritarian parenting is linked to child aggression, social withdrawal from peers, poor self-confidence, and internalized distress (Baunuind, 1989; Steinberg et al., 1994) as well as continuity of such patterns into adolescence (Baunnind, 199 1; Lamborn, Mounts, Steinberg, & Dornbusch, 1991; Steinberg et al., 1994). Pennissive (high warmth, low control) parents provide their children with little structure and discipline, make few demands for mature behavior, and tolerate even those impulses in children that meet with societal disapproval. Permissive parents are typically warm and responsive but not demanding. Permissive parenting is associated with aggression (Olweus, 1980), impulsivity, and a lack of social responsibility and independence in children (Baumrind, 1989, 1991) and with school misconduct, drug and alcohol use, and heightened orientation toward and value of peer activities and norms in adolescents (Baumrind, 1991; Steinberg et al., 1994). Neglectjul (low warmth, low control) parents offer little affection or discipline to their children and appear to have little concern for or interest in parenting. That is, neglectful parents are neither responsive to the reasonable needs and desires of the youth nor demanding of responsible, age-appropriate behavior with respect to tasks or interpersonal relationships. Of the four parenting types, neglectful parenting is most strongly related to children's distress. Children from neglectful homes are characterized by poorer adjustment on many indices of functioning than children from permissive or authoritarian homes, and this negative trajectory continues through adolescence, when neglectful parenting is associated with sizable increases in adolescent delinquency and drug use (Steinberg et al., 1994). 33 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. The Marital Subsystem In families headed by two married adults, the marital relationship is the foundation of the family system. INTIMACY AND POWER Just as the major dimensions of parent-child interactions are warmth and control, so the major dimensions of marital interactions reflect intimacy and power (Emery, 1992, 1994). Intimacy refers to the strength of the emotional bond between adults, and a positive emotional bond is important to the longevity of intimate relationships. CONFLICT Research indicates that conflict between parents is associated with a host of problems in children and families, including externalizing problems, childhood aggression (particularly in boys), depression in mothers, inconsistent parenting practices, and increased parent-child conflict (for reviews, see Cummings & Davies, 1994; Grych & Fincham, 1992). The frequency and intensity of conflict and the presence of both verbal and physical conflict (Fantuzzo et al., 1991; Vissing, Strauss, Gelles, & Harrop, 1991) are associated with higher levels of evels of conduct problems in youth. Several mechanisms may account for the association between marital conflict and child behavioral problems. Marital problems may be linked with behavioral problems because the resulting emotional distress interferes with parental responsiveness to children's needs, marital conflicts interfere with parents' abilities to deliver consistent discipline, parents in conflict may be modeling poor conflict-resolution skills, and the emotionally charged environment may be stressful to children. 34 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Family System Transitions: Divorced, Remarried, and Single-Parent Families The fact that divorce is often followed by remarriage and/or living in a singleparent family means that many children experience more than one set of the multiple and sometimes difficult transitions (Cherlin, 1992) described next. DIVORCED FAMILIES Longitudinal research indicates that divorce is a developmental process during which a series of "partially predictable events" often occurs (Emery, 1994, p. 17). REMARRIED FAMILIES As with divorce, research on the reconstitution of families through marriage supports a developmental, family systems perspective (Hetherington & Clingempeel, 1992). Remarriage requires renegotiation of relationships, roles, and boundaries among all members of the two families coming together to form a new family group. SINGLE-PARENT FAMILIES Many families headed by a single parent function effectively to meet the instrumental and affective needs of the children and the parent. In some families, the responsibilities of childrearing are supported by, or shared with, another family member such as a grandparent or another relative. KIN AS PARENT FIGURES In a significant percentage of families with a youth presenting serious antisocial behavior, grandparents or other relatives are the surrogate parents, often assuming guardianship, if not legal custody, of the youth. In some of these cases, surrogate parents had substantial involvement with the youth prior to assuming primary parenting responsibility. 35 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Assessing Family Functioning Assessment of family functioning is an ongoing process initiated when the practitioner first meets the family and refined throughout treatment as interventions are implemented and their effects are observed. Together, the practitioner and family members observe and try to tease out the specific family interactions that are the most powerful, proximal predictors of the identified problems. Throughout this process, practitioners do the following: I. Develop hypotheses (e.g., explanations, hunches, or beliefs a practitioner or family member develops regarding the possible causes of the referral problem) regarding the relative contributions of familial factors to problem behaviors. Consistent with MST Principles 4 and 5 (present focused, targeting specific, well-defined problems; targeting sequences of behavior within or between multiple systems), hypotheses focus primarily on observable interactions and behaviors. 2. Gather evidence (i.e., information that was observed, self-reported, or concretely monitored, such as checklists, charts, check-in phone calls by the parent, other family members, school personnel, neighbors, etc., and the practitioner) to support or refute those hypotheses. 3. Implement interventions that target the hypothesized contributing factors. 4. Observe whether the interventions result in changes in problem behaviors. 5. Identify barriers to intervention success. 6. Design interventions to overcome these barriers. These steps are part of the iterative process of MST case conceptualization and intervention implementation depicted in Figure 2.2 of Chapter 2. 36 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. Family-School Linkage Parents' involvement in their children's schooling is an important determinant of academic achievement and psychosocial functioning in school. Therapists should assess, therefore, such parental involvement in school-related activities as the following: Monitoring homework assignments and exam grades. Setting aside a block of time and a quiet place for the child to study after school. Supporting extracurricular school functions. Implementing contingencies that are based on the child's efforts and performance. Providing overt support for teachers' educational demands, behavioral demands, and goals. PARENTAL ATTITUDES TOWARD EDUCATION Youth academic and behavioral problems can be exacerbated when academic success is not a high priority for the parents. PARENT-SCHOOL CONFLICT Children's school performance usually suffers when conflicts develop between parents and school personnel. Such conflict can be linked with several circumstances, including the following: Miscommunications that can occur when parents and educators are of disparate sociocultural backgrounds (e.g., parents might feel intimidated by or resentful of the educators). Perceived insults or "putdowns" based on previous interactions between the parents and school personnel. The youth playing the parent off against the school (e.g., convinces his parents that the teacher does not like him and is discriminating against him). Parental perceptions that the school is not committed to meeting the needs of the youth. The perception of school personnel that the parent has little concern for the youth's performance or behavior in school. 37 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. The goals of the meeting between the therapist, parents, and school personnel, therefore, are to do the following: 1 . Clarify that all parties have the youth's best interest at heart. 2. Explain the rationale (i.e., fit) of the proposed interventions to all parties. 3. Provide an opportunity to revise the proposed interventions, pending additional input from school personnel (assuming that any revisions are approved by the parents and therapist). 4. Delineate the exact responsibilities of each party vis-a-vis the interventions, with the parents assuming the bulk of the responsibility. 5. Develop a system for monitoring implementation and outcome of the interventions. 6. Develop a system for providing all parties with feedback regarding the outcomes. 7. Delineate strategies for revising the school-related intervention protocol, with the parents and therapists taking responsibility for such. 38 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. When and How to Conduct Individually Oriented Interventions In our experience, team (i.e., practitioner and clinical supervisor) decisions to pursue individual treatment with parent figures most often (1) pertain to problems that interfere with parental functioning, such as depression, anxiety disorders, and substance abuse; and (2) are made at two "ends" of the MST treatment period. These two ends are: 1. Early in treatment, if the parent figure's functioning is compromised so frequently or to such an extent that the practitioner is unable to develop a working alliance, identify the parent's treatment goals, or engage the parent in making even minor changes toward a goal he or she has identified as important. 2. Well into treatment, when interventions targeting intrafamilial (parent-child, marital, kin) or extrafamilial (family-school, peer, neighborhood) interactions have been implemented inconsistently or implemented with poor results, and specific aspects of the parent's functioning are identified as critical barriers to implementation or success. With respect to adolescents, four types of situations can warrant the implementation of individual interventions. These are: When a youth continues to display serious aggressive or impulsive behaviors in one or more contexts (e.g., in the classroom, with certain peers, and with siblings) after systemic interventions have been consistently implemented by parents, teachers, and other relevant players in the youth's natural ecology. 4. When a youth with biologically influenced difficulties (e.g., ADHD, bipolar disorder, or clinical depression) is consistently taking appropriately prescribed medication and well-implemented ecological interventions are in place, yet, problems with impulsive or aggressive behavior continue to occur at home, in school, or with peers. 5. When the sequelae of victimization (i.e., physical abuse, sexual abuse, and criminal victimization) contribute to referral problems. 6. When intensive and comprehensive efforts to engage caregivers in changing parenting practices or other aspects of the youth's ecology are unsuccessful, efforts to overcome barriers to change are unsuccessful, and the adolescent will continue to live in a home in which the lack of favorable clinical change will exacerbate the identified problems. Source: Henggler, S. et. al. ( 1998). Multisystemic Therapy. New York, Guilford press. 39 Theories and Methods of Family Intervention Cynthia Franklin, Ph.D. The Hard Side of Hierarchy The Soft Side of Hierarchy Who Makes the Rules Who Soothes Them Who Determines and Carries out the Consequences Who Provides Reassurance to Whom Who Tells Whom What to Do Who Protects Them Who Makes Major Decisions Who Has the Responsibility for Expressing Love And Empathy Who Is the Provider of Good Things and Good Times Who Usually Determines the Mood of Situations Who Has the Responsibility to Listen to Whom? 40