METHOTREXATE – FOR USE IN IBD METHOTREXATE CLINICAL
advertisement

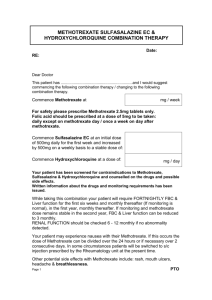
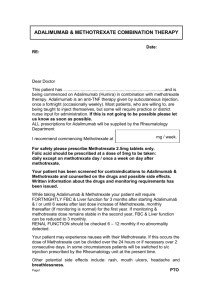
METHOTREXATE – FOR USE IN IBD METHOTREXATE CLINICAL PROTOCOL FOR INFLAMMATORY BOWEL DISEASE (IBD) Approved by: Designation Consultant Gastroenterologists Name Dr K Kapur Signature Dr A Soliman Dr S Riyaz Dr E Said Dr K Mudhi Chief Pharmacist Mike V Smith Lead Pharmacist Gillian Smith Specialist IBD Pharmacist Fernando Garcia Fuertes Written by: Fernando Garcia Fuertes, Specialist IBD Pharmacist Date: May 2014 Approved by Medicines Management Committee Date: July 2014 Review date: May 2018 Date METHOTREXATE – FOR USE IN IBD 1. Aims The aims of this protocol are: - To ensure evidence based care is delivered to patients requiring methotrexate according to BSG guideline and ECCO guideline. - To monitor patients initiated on methotrexate, side effects profile, potential complications and possible drug interactions with methotrexate. - To support healthcare professionals involve by providing up-to-date guidance for use of methotrexate. 2. Gastroenterolgist responsibilities - To assess the suitability of the patient for treatment To initiate treatment To perform baseline tests To inform patient of side effects and long term monitoring required prior to inititisiating treatment. 3. Responsibilities for the IBD Pharmacist, IBD Nurse or PIU Nurse - To counsel the patient on methotrexate To initiate the administration of subcuteneous injection To train patient to self-administer the injection subcutaneously 4. Drug monitoring and discharge by IBD Pharmacists - To monitor blood test on behalf of Gastroenterologist until drug stable To supply methotrexate monitoring booklets once patient is ready to be transferred to GP 5. Indications for use of Methotrexate in IBD Methotrexate 25mg weekly (oral, subcutaneous or intramuscular injection – unlicensed for use in IBD). (A. Dignass, 2010) Methotrexate is generally reserved for treatment of active or relapsing Crohn’s disease in those refractory to or intolerant of thiopurines. (AG., 2003) The evidence base for efficacy of methotrexate in UC is restricted to observational studies. Note: Patients should be advised not to become pregnant or attempt to father a child following 3 months following cessation of treatment. 6. Mechanism of action: Currently, several pharmacological mechanisms of methotrexate action have been suggested, including inhibition of purine and pyrimidine synthesis, suppression of transmethylation reaction with accumulation of polyamines, reduction of antigenWritten by: Fernando Garcia Fuertes, Specialist IBD Pharmacist Date: May 2014 Approved by Medicines Management Committee Date: July 2014 Review date: May 2018 METHOTREXATE – FOR USE IN IBD dependent T-cell profiferation, and promotion of adenosine release with adenosinemediated suppression of inflammation. (BN., 2005). It is possible that a combination of these mechanisms is responsible for the antiinflammatory effects of methotrexate. To date, the adenosine-mediated antiinflammatory effect of methotrexate is best supported by the in vitro, in vivo, and clinical data. Anti-inflammatory Effect of Methotrexate is Mediated by Adenosine: Adenosine is an endogenous purine nucleoside that, following its release into the extracellular space, binds to specific adensosine receptors expressed on the cell surface. Adenosine is an important signaling molecule modulating a vast array of physiological funtions. However, extensive evidence suports the hypothesis that adenosine, acting on adenosine receptors, is a key mediatro of th antiinflammatory effect of methotrexate. 7. Base line tests - Full Blood Counts (FBC) Urea & Electrolytes (U&Es) Liver Function Test (LFTs) Peptide of type III procollagen (P3NP) assay. If it is raised discuss with Gastroenterologist before starting treatment. HBV and HCV screening Chest Xray and pulmonary function test (if pre-existing lung disease) eg. asthma, pulmonary fibrosis etc. (Consultant to confirm on referral form). 8. Contraindication (Medac, 2014) - Hypersensitivity to the active substance or to any of the excipients listed. Severe liver impairment. Contraindicated if bilirubin values are >5 mg/dl (85.5 μmol/L). Note: Methotrexate should be administered with great caution, if at all, to patients with significant current or previous liver disease, especially when caused by alcohol. - Alcohol abuse. Severe renal impairment (Creatinine clearance less than 20 ml/min) Pre-existing blood dyscrasias, such as bone marrow hypoplasia, leukopenia, thrombocytopenia, or significant anaemia. Serious, acute or chronic infections such as tuberculosis and HIV. Ulcers of the oral cavity and known active gastrointestinal ulcer disease. - - Pregnancy: Methotrexate can cause foetal death, embryotoxicity, abortion or teratogenic effects when administered to pregnant women. During pregnancy, especially in the first trimester, cytotoxic drugs must only be given when strictly indicated, weighing the needs of the mother against the risks to the foetus. Treatment with methotrexate during the first trimester has resulted in a high risk of malformations (in particular cranial malformation and malformation of the extremities). Breast-feeding: Methotrexate passes into breast milk in quantities such that there is a risk to the child even at therapeutic doses. Breast feeding must therefore be discontinued during treatment with methotrexate. Written by: Fernando Garcia Fuertes, Specialist IBD Pharmacist Date: May 2014 Approved by Medicines Management Committee Date: July 2014 Review date: May 2018 METHOTREXATE – FOR USE IN IBD - Concurrent vaccination with live vaccines. 9. Dose - - - - The standard induction dose is 25mg subcutaneously ONCE WEEKLY for 16 weeks. Maintenance dose: 15mg orally ONCE WEEKLY thereafter. Subcutaneous route is preferable than oral as it shows less changes in variability in the drug absorption (Kurnik D, 2003) Treatment should be started by subcutaneous route. A switch to oral administration may be attempted for maintenance while carefully monitoring the clinical response. Subcutaneous route is as effective as intramuscular dosing. Doses < 15mg/week are ineffective for active Crohn’s disease. Feagan TRIAL study suggest that many patients who relapse while receiving lowdose maintenance therapy with methotrexate might ultimately be able to discontinue prednisolone therapy if the dose of methotrexate is increased to 25mg weekly (Feagan B, 2000). Note: Retreatment with higher dose of methotrexate (25mg), usually in combination with prednisolone, induced remission in over half the patients who had relapsed (Feagan B, 2000). Gastrointestinal side effects from methotrexate can be limited by co-prescribing folic acid 5mg daily except on the day of methotrexate. 10. Adverse Drug Reaction (Medac, 2014) - - The most frequently reported undesirable effects Ulcerative stomatitis Leucopenia Neutropenia Trombocytopenia Nausea and bloating Lost of appetite Other frequently reported undesirable effects are: Headache Drowsiness Feeling unwell Unusual tiredness Flu-like symptoms Chills and fever Dizziness Reduced resistance to infections Diarrhoea (especially during the first 24-48 hours after administration of methotrexate) Skin rashes – urticaria / pruritis /flushing of the face Joint pains / arthralgia Written by: Fernando Garcia Fuertes, Specialist IBD Pharmacist Date: May 2014 Approved by Medicines Management Committee Date: July 2014 Review date: May 2018 METHOTREXATE – FOR USE IN IBD - Abdominal pain (pancreatitis) Pulmonary complications such as pneumonitis followed by interstitial fibrosis. The latter may be progressive. - Mild elevation in serum liver enzymes and, more importanly, with development of chronic liver injury, progressive fibrosis, cirrhosis and portal hypertension. Symptoms are usually absent until cirrhosis is present, and liver tests are tipically normal or minimally and transiently elevated. Dose regimens (5 to 15mg in one dose weekly with folate supplementation), fibrosis and clinically apparent liver disease are rare even with long term use. The hepatic fibrosis and cirrhosis due to methotrexate typically arise after 2 to 10 years of treatment and can present with ascites, variceal hemorrhage or hepatosplenomegaly. (Medicine, 2014) 11. Folic Acid Folic acid 5mg orally should be prescribed daily except on the day of methotrexate. This helps reduce nausea and hepatotoxicity. (See PGD for folic acid). 12. Routine testing U&E, FBC and LFTs: Fortnightly for 2 months ( 0-2 months) Monthly for 4 months ( 2-6 months) Then 3 monthly (if bloods are stable) Peptide of type III procollagen (P3NP) assay for detection of liver fibrosis induced by methotrexate (Chalmers RJ, (Chalmers RJ, 2005) (Maurice PD, 2005) first 6 month since started therapy then every 12 moths. 13. Monitoring guidelines This section is for guidance only. Each decision should be based on the situations own merits, and discretion used at all times. The patient should be referred back to the Gastroenterologists if: Either WCC < 3.7 x 109/L or 9 Platelets < 150 x 10 /L or Neutrophils <1.7 x 109/L AST or ALT > 3 times the upper limit Patients with neutropenia on blood results and signs or symptoms of an infection will be referred urgently to a Gastroenterologist, who will assess whether admission is necessary. Written by: Fernando Garcia Fuertes, Specialist IBD Pharmacist Date: May 2014 Approved by Medicines Management Committee Date: July 2014 Review date: May 2018 METHOTREXATE – FOR USE IN IBD 14. Treatments of overdose (NPIS, 2011) a. Contact Gastroenterologist b. Check full blood count, urea, electrolytes and liver function tests. The full blood count may be normal initially but pancytopenia may develop over the next 7 - 12 days. Repeat blood tests at weekly intervals, if asymptomatic, for 4 weeks after the overdose. c. Measure the methotrexate concentration no earlier than 4 - 6 hours after last ingestion. Discuss with the biochemistry laboratory. i. Give folinic acid rescue (leucovorin) without waiting for the result of a methotrexate assay in those ingesting more than 3 mg/kg in less than 24 hours or those with reduced elimination (renal failure). ii. If the methotrexate concentration is unknown, give folinic acid 100 mg/m2 body surface area IV 6 hourly until the methotrexate concentration is known. iii. If methotrexate concentration is known see table below for doses. Methotrexate drug level (Molar) Folinic acid dose More than 50 micromol/L (more than 5 x 10-5M) 1000 mg/m2 6 hourly IV (give same dose 3 hourly if the patient has renal impairment) 5 - 50 micromol/L (5 x 10-5M to 5 x 10-6M) 100 mg/m2 3 hourly IV 0.5 - 5 micromol/L (5 x 10-6M to 5 x 10-7M) 30 mg/m2 6 hourly IV/PO Less than 0.5 micromol/L (less than 5 x 10-7M) 10 mg/m2 6 hourly PO/IV Continue treatment until methotrexate concentration is less than 5 x 10-8M (less than 0.05 micromol/L). NB - Folic acid cannot be used as a substitute for folinic acid in patients with methotrexate toxicity because the biological availability of folic acid depends upon the action of dihydrofolate reductase, which is inhibited by methotrexate. Folinic acid does not require activation by dihydrofolate reductase so its function is not affected by the presence of methotrexate. Written by: Fernando Garcia Fuertes, Specialist IBD Pharmacist Date: May 2014 Approved by Medicines Management Committee Date: July 2014 Review date: May 2018 METHOTREXATE – FOR USE IN IBD 15. Drug interactions (BNF, 2014) Acetazolamide Acitretin Aspirin Ciclosporin Ciprofloxacin Dexamethasone Digoxin Doxycycline Leflunomide NSAIDs Neomycin Penicillins Phenytoin Probenecid Proton Pump Inhibitors Pyrimethamine Sulfamethoxazole Sulfonamides Tetracycline Theophylline Trimethoprim excretion of methotrexate increased by alkaline urine due to acetazolamide plasma concentration of methotrexate increased by acitretin (also increased risk of hepatotoxicity)—avoid concomitant use excretion of methotrexate reduced by aspirin (increased risk of toxicity) risk of toxicity when methotrexate given with ciclosporin excretion of methotrexate possibly reduced by ciprofloxacin (increased risk of toxicity) possible increased risk of hepatoxicity when high-dose methotrexate given with dexamethasone methotrexate possibly reduces absorption of digoxin tablets increased risk of methotrexate toxicity when given with doxycycline risk of toxicity when methotrexate given with leflunomide excretion of methotrexate probably reduced by NSAIDs (increased risk of toxicity)—but for concomitant use in rheumatic disease absorption of methotrexate possibly reduced by neomycin excretion of methotrexate reduced by penicillins (increased risk of toxicity) antifolate effect of methotrexate increased by phenytoin excretion of methotrexate reduced by probenecid (increased risk of toxicity) excretion of methotrexate possibly reduced by proton pump inhibitors (increased risk of toxicity) antifolate effect of methotrexate increased by pyrimethamine increased risk of haematological toxicity when methotrexate given with sulfamethoxazole (as co-trimoxazole) increased risk of methotrexate toxicity when given with sulfonamides increased risk of methotrexate toxicity when given with tetracycline methotrexate possibly increases plasma concentration of theophylline increased risk of haematological toxicity when methotrexate given with trimethoprim (also with co-trimoxazole) Written by: Fernando Garcia Fuertes, Specialist IBD Pharmacist Date: May 2014 Approved by Medicines Management Committee Date: July 2014 Review date: May 2018 METHOTREXATE – FOR USE IN IBD 16. Bibliography A. Dignass, G. V. (2010). The second European evidence-based Consensus on the diagnosis and management of Crohn's disease: current management (ECCO). Journal of Crohn's and Colitis, 28-62. AG., F. (2003). Methotrexate : first or second-line immunomodulator? . European Journal Gastroenterology and Hepatology, 15:225-31. BN., C. (2005). Low-dose methotrexate: a mainstay in the treatment of rheumatoid arthritis. Pharmacology Review 57 (2), 163-72. BNF. (2014, March). British National Formulary. Retrieved May 19, 2014, from Medicines Complete: http://www.medicinescomplete.com/mc/bnf/current/bnf_int511-methotrexate.htm Chalmers RJ, K. B. (2005). Replacement of routine liver biopsy by procollagen III aminopeptide for monitoring patients with psoriasi receiving long-term methotrexate: a multicentre audit and health economic analysis. . The British Journal of Dermatology, 152 (3):444-50. Feagan B, F. R. (2000). A comparison of methotrexate with placebo for the maintenance of remission in crohn's disease. The New England Journal of Medicine, 342; 22:1627-1632. Kurnik D, L. R. (2003). Bioavailability of oral vs subutaneous low-dose methotrexate in patients with Crohn's disease. Aliment Pharmacology Therapy, 18:57-63. Maurice PD, M. A. (2005). Monitoring patients on methotrexate: hepatic fibrosis not seen in patients with normal serum assays of aminoterminal peptide of type III procollagen. The British Journal of Dermetalogy, 152(3):451-8. Medac. (2014, 04 23). Medicines Compendium. Retrieved 05 19, 2014, from EMC: https://www.medicines.org.uk/emc/medicine/22145/SPC/Metoject+50+mg+ml+solution+fo r+injection/#PHARMACOKINETIC_PROPS Medicine, U. N. (2014, 5 7). Livertox NIDDK. Retrieved 5 25, 2014, from Livertox: http://livertox.nlm.nih.gov/Methotrexate.htm NPIS, U. (2011, 11). TOXBASE. Retrieved 05 19, 2014, from TOXBASE: http://www.toxbase.org/Poisons-Index-A-Z/M-Products/Methotrexate/ Written by: Fernando Garcia Fuertes, Specialist IBD Pharmacist Date: May 2014 Approved by Medicines Management Committee Date: July 2014 Review date: May 2018