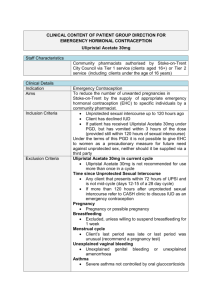
ulipristal acetate 30mg tablet (ellaOne®)
advertisement
")
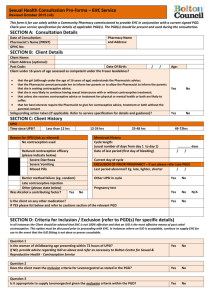
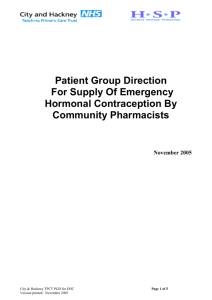
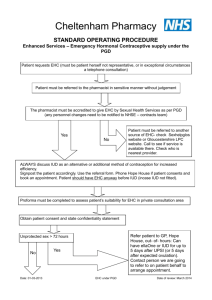
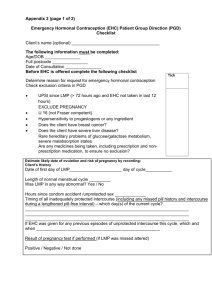
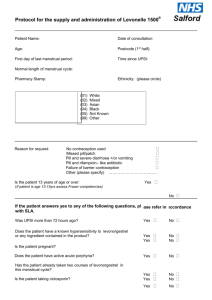
Draft National Template Patient Group Direction for the supply of: ulipristal acetate 30mg tablet (ellaOne®) by Community Pharmacists This direction was prepared by Mr G Holyfield (Public Health Wales) as lead author with advice, comment and support from EHC expert group: - Mr T Banner (Hywel Dda UHB), Dr N Bryant and Ms E Hinks (Cwm Taf UHB), Mr M Curson (Aneurin Bevan UHB), Ms C Poulter (Cardiff University) and Mr A Evans (Welsh Government) as a template to assist organisations to prepare their own documents. It is the responsibility of local organisations to check the accuracy of the information, that the information is up to date, and to amend as required for local use. PGD EHC Ulipristal v1 1 3 December 2014 Patient Group Direction for the Supply of: ulipristal acetate 30mg tablet (ellaOne®) Name and address of organisation: Date PGD comes into effect: Review date: (2 years or less) Expiry date: (2 years or less) Name of Medicine Approved name: ulipristal acetate 30mg tablet ellaOne® Proprietary name: Professionals to whom PGD applies Community pharmacists Lead Doctor’s name, job title, signature and date: Lead Pharmacist’s name, job title, signature and date: Lead Nurse's name, job title, signature and date: On behalf of the Health Organisation name, job title, signature and date: PGD EHC Ulipristal v1 2 3 December 2014 Emergency contraception within 72 – 120 hours of unprotected sexual intercourse (UPSI) or failure of other contraceptive method. Clinical Condition Note on mid-cycle use: The PGD emphasises the importance of additional referral for IUD for women presenting having had UPSI in mid cycle (see mid cycle calculator in appendix 1) Criteria for inclusion: Patient is aged 13 years or over and presents in person at the community pharmacy between 72 and 120 hours of unprotected sexual intercourse (UPSI) or failure of a contraceptive method. (Under 16 year olds are included provided they meet the criteria of the Fraser Guidelines on consent to medical treatment. The patient has capacity to understand the nature and purpose of the treatment and gives their consent to providing the relevant clinical information. In addition, if patient is under 13 years of age a referral to social services should be made in line with the Child Protection Procedures of the Health Board.) Remember a more effective alternative is a copper intra-uterine device (Cu-IUD) Levonorgestrel 1500mcg is still recommended for patients who present at up to 72 hours following unprotected intercourse. NB: If patient has vomited within 3 hours of taking a dose of ulipristal 30mg a further supply can be given provided patient is still within 120hours of UPSI. Patient gives their consent to providing the relevant clinical information to the pharmacist once the pharmacist has assessed their capacity to understand the nature and purpose of the treatment Emergency contraception decision support guide for pharmacists (see appendix 2) Criteria for exclusion: Patients aged 12 years or under. Patient who the pharmacist has assessed as not having capacity to understand the nature PGD EHC Ulipristal v1 3 3 December 2014 and purpose of treatment. Patients who do not agree to share relevant clinical information or there is no valid consent. Requests made by third parties on behalf of patient. UPSI occurred more than120 hours ago. UPSI occurred less than 72 hours after UPSI, advise patient that levonorgestrel (Levonelle® 1500) is recommended - refer to levonorgestrel PGD Previously had one or more episodes of UPSI in current menstrual cycle (whether treated with levonorgestrel or not). Patient used ulipristal for emergency hormonal contraception in current menstrual cycle (NB: unless vomiting occurred within 3 hours of previous dose, in which case another dose can be supplied). Concomitant use with emergency contraception containing levonorgestrel is not recommended. Patients who are/or think may be pregnant (pregnancy should be excluded before ellaOne is administered) Patients whose last menstrual period (LMP) was more than 4 weeks ago (Note: some women have a longer cycle than 28 days so manage accordingly) Patients whose last LMP was abnormal/unusual Patients who have delivered a baby within last 3 weeks (EHC not required in these circumstances). Women who wish to continue breast feeding (see cautions section below) Concomitant use of ulipristal (EllaOne®) with CYP3A4 inducers. (Ulipristal acetate (UPA) is not advised in women using enzyme-inducing drugs or who PGD EHC Ulipristal v1 4 3 December 2014 have taken them within the last 28 days (Faculty of Sexual and Reproductive Health (FSRH)). BNF also indicates that effectiveness of ulipristal may be reduced for up to 4 weeks after stopping enzyme inducer(s)). Antiepileptics: phenytoin, fosphenytoin,carbamazepine, oxcarbazepine, phenobarbital primidone Antivirals: ritonavir HIV infection: efavirenz, nevirapine, rifampicin, rifabutine Herbal medicines containing Hypericum perforatum (St. John's wort). Avoid concomitant use with: Drugs that affect gastric pH: Antacids, H2 antagonists and proton pump inhibitors. Patients with: Known hypersensitivity to ulipristal or any excipients, or patient has previously experienced any severe clinical problems with hormonal contraception. Rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption are excluded from treatment with ulipristal (ellaOne®) under this PGD, as this medicine contains lactose monohydrate. Severe asthma (where asthma is not controlled despite oral glucocorticoid treatment) Unexplained vaginal bleeding Renal or hepatic impairment (in absence of specific studies, no specific dose recommendations can be made) Cautions (including any relevant action to be taken) Severe malabsorption syndromes e.g. severe diarrhoea, Crohn’s. The FSRH advise that oral contraception may be less reliable in women with inflammatory bowel disease who have malabsorption due to severe small bowel disease or resection, or who have vomiting or severe diarrhoea for more than 24 hours. Refer to Sexual health services for IUD/follow up Breast feeding. After taking ulipristal PGD EHC Ulipristal v1 5 3 December 2014 (ellaOne®), breastfeeding is not recommended for 7 days. The manufacturers advise that women who are breast feeding should feed their baby immediately before taking the tablet, then pump and discard the breast milk for the next 7 days in order to stimulate lactation. Breast feeding can be resumed after 7 days. If the woman is unable or unwilling to comply with this advice she is excluded from treatment with ulipristal (ellaOne®) under this PGD- refer to GP or Community Sexual Health Clinic. Potential for other medicines to affect ulipristal (also see Appendix 1 of the current British National Formulary and SPC): progestogens: possible reduced contraceptive effect vinblastine and quinidine (micromedex). CYP3A4 enzyme inhibitors. Ulipristal acetate is metabolized by CYP3A4 in vitro. In vivo results show that administration of ulipristal acetate with a potent and a moderate CYP3A4 inhibitor increased Cmax and AUC of ulipristal acetate with a maximum of 2- and 5.9-fold, respectively. The effects of CYP3A4 inhibitors are unlikely to have any clinical consequences. Although the use of ellaOne does not contraindicate the continued use of regular hormonal contraception, ellaOne may reduce its contraceptive action. Therefore, after using emergency contraception, it is recommended that subsequent acts of intercourse be protected by a reliable barrier method until the next menstrual period starts. If a woman wishes to initiate hormonal contraception as a regular contraception method, she can do so immediately after using ellaOne, but the woman should use a reliable barrier method until the next menstrual period. The UK manufacturer’s SPC (May14) states that in vitro ulipristal acetate may be an inhibitor of P-glycoprotein (P-gp) at clinically relevant concentrations. Results in vivo with the P-gp substrate fexofenadine were PGD EHC Ulipristal v1 6 3 December 2014 inconclusive. If further states that the effects of the P-gp substrates are unlikely to have any clinical consequences. BNF advises to give digoxin at least 1.5 hours before or after ulipristal BNF advises to give dabigatran at least 1.5 hours before or after ulipristal. BNF advises to give fexofenadine at least 1.5 hours before or after ulipristal Action if excluded: All excluded patients should be referred to a Sexual Health Clinic or GP practice. Patient aged 12 years or under - the Child Protection Team must be contacted for children of 12 years and under, who present having had sexual intercourse Consider the supply and administration of levonorgestrel 1500mg (refer to levonorgestrel PGD) If unprotected sex was within the last 5 days (120 hours) the patient may be suitable for IUD (intrauterine device) insertion. Referral should be made in a suitable timeframe to allow this to happen. Advise women using liver enzyme-inducing drugs that an IUD is the only option. Seek further advice: To be completed by LHB according to local arrangements. Know the referral pathway into local sexual and reproductive health services or how to contact the local lead doctor for sexual and reproductive health for medical advice. Description of Treatment Name of Medicine Approved name: ulipristal acetate 30mg tablet ellaOne® Proprietary name: Legal status: Prescription Only Medicine (POM) Form: Tablet PGD EHC Ulipristal v1 7 3 December 2014 Strength: Dosage: Route of Administration: Frequency of Administration: 30mg One tablet as a single oral dose. Oral 30mg tablet as a single dose between 72 and 120 hours after UPSI. NB: If patient has vomited within 3 hours of taking a dose of ulipristal the dose can be repeated. Total treatment quantity: Adverse reactions: One or two 30mg tablet(s) Side effects (BNF) may include; Nausea,vomiting, diarrhoea,abdominal pain Dizziness Fatigue Headache Temporary disturbance of menstrual cycle (bleeding, spotting, next period early or late) Back pain Muscle spasms Less common; tremor, hot flush, uterine spasm, breast tenderness, dry mouth, blurred vision, pruritis and rash. (This list is not exhaustive. Please refer to current SPC for further information.) Reporting procedure of adverse reactions: Side effects should be recorded in the patient record/notes. Refer to a GP where necessary. Consider reporting via the MHRA yellow card reporting scheme. Verbal advice for patient: Advice on likely side effects, action needed if vomiting occurs and delayed menses. All patients should be advised on the option of an emergency intra-uterine device (IUD) as an alternative. An IUD is more effective than hormonal emergency contraception especially when there are multiple risks or the patient is towards the end of the 120 hour time limit. Explain that: the next period may be early or late that a barrier method of contraception needs to be used until the next period the patient should contact their GP if PGD EHC Ulipristal v1 8 3 December 2014 any lower abdominal pain occurs (possibility of an ectopic pregnancy) if the patient has not had their period within 7 days of their expected date of menstruation, abnormal bleeding occurs or pregnancy is suspected, they should attend a sexual health clinic with a urine sample to confirm or exclude pregnancy. Highlight that ulipristal (ellaOne®) is used for emergency contraception only. Suggest where appropriate that patient makes an appointment with their GP or sexual health clinic to discuss their on-going contraceptive needs. Remind the patient that the use of ulipristal (ellaOne®) does not provide ongoing contraceptive protection and that she must continue to use another method for the remainder of the cycle. Patients taking oral contraceptives. Those taking combined oral contraceptives (COC) or progestogen only pills (POP) should be advised to continue taking their pills but to also use additional barrier method contraceptive precautions until their next period. This is because ulipristal (ellaOne®) will reduce the efficacy of regular hormonal contraception. Advise patient that they can be tested and treated for sexually transmitted infections if necessary and sign-post the patient to locally available services. If the patient is breast-feeding advise as noted in cautions section. Written information for patient: The following must be provided: An ellaOne® Patient Information Leaflet A leaflet on currently available forms of contraception Information on local sexual health services Information about local genitourinary medicine (GUM) services Follow Up: With Sexual health service 3 weeks later for pregnancy testing and contraceptive/sexual health advice. PGD EHC Ulipristal v1 9 3 December 2014 Arrangements for referral for medical advice: Refer to a GP or sexual health clinic as necessary. Records of supply for audit: Maintain a record of the supply, batch number and expiry and any advice given (complete EHC community pharmacy proforma) The pharmacist must document Fraser Competence for clients under (or appearing to be under) 16 years of age. The pharmacist will be required to complete the National Electronic Claim and Audit Form (NECAF) for each consultation. NB: Records may need to be shared with LHB representatives subject to appropriate patient confidentiality protocols. Staff Professional qualifications: Training: Community Pharmacists currently registered with the General Pharmaceutical Council (GPhC). The Pharmacist must have completed the Wales Centre for Pharmacy Professional Education’s (WCPPE) All Wales procedure for accreditation to provide the Emergency Contraception Enhanced Service. http://www.wcppe.org.uk/assessment/enhance d-services/ehc-accreditation/emergencyhormonal-contraception The pharmacists must have a certificate demonstrating compliance with the National Competence and Training Framework for the service The pharmacist’s name must be included in the All Wales Pharmacy Database for the service. The pharmacist where required by the Local Health Board, has successfully completed an enhanced Criminal Records Bureau (CRB) check The pharmacist must handle all requests for emergency hormonal contraception in a sensitive and non-judgmental manner, and act PGD EHC Ulipristal v1 10 3 December 2014 in accordance with guidance issued by the General Pharmaceutical Council on consent, raising concerns and confidentiality. The pharmacist must be competent to assess a patient’s capacity to understand the nature and purpose of the treatment in order to give or refuse consent. Competency assessment: The pharmacist must satisfy the requirements of WCPPE. Continuing education: The pharmacist must undertake regular CPD and maintain own level of competence and knowledge in this clinical area to provide the service. The pharmacist must have access to and be familiar with the latest Summary of Product Characteristics for ulipristal (ellaOne®) and BNF. Special Considerations / Additional Information: Pharmacy premises must respect a patient’s right to confidentiality and safety and provide an acceptable level of privacy. References: PGD EHC Ulipristal v1 11 British National Formulary 66 Sept 2013 Summary of Product Characteristics ellaOne® http://www.medicines.org.uk/emc/medici ne/22280 (accessed 7 July 2014) Emergency Contraception Guidelines, Faculty of Sexual & Reproductive Health Clinical Effectiveness Unit (2012) http://www.fsrh.org (accessed 14 March 2014) Drug Interactions with Hormonal Contraception. Faculty of Sexual & Reproductive Healthcare Clinical Guidance (updated 2012) http://www.fsrh.org/pdfs/CEUguidancedr uginteractionshormonal.pdf (accessed 7 July 2014) GPhC Guidance – Consent 2012, Raising Concerns 2012 , and Confidentiality 2012 http://www.pharmacyregulation.org/stan 3 December 2014 dards/guidance (accessed 18 Mar 2014) NICE Good Practice Guidance on Patient Group Directions http://www.nice.org.uk/mpc/goodpractic eguidance/GPG2.jsp (accessed 17 March 2014) This Patient Group Direction is to be read, agreed and signed by all registered community pharmacists authorised to operate the PGD. One copy should be given to each named community pharmacist; the original signed copy should be kept by the nominated member of staff with responsibility for PGDs within the pharmacy. This will usually be the Superintendent Pharmacist or Responsible Pharmacist. I confirm that I have read and understood the content of this patient group direction and that I am willing and competent to work under it within my professional code of conduct. Name of Pharmacist: GPhC Registration Number: Pharmacy location: Signature: Date: Signed copy to be returned to: PGD EHC Ulipristal v1 12 3 December 2014 Appendix 1: Cycle length (in days) Calculating the mid cycle range for varying cycle lengths. 1 2 3 4 5 6 7 8 Day 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 26 28 30 32 Mid cycle is shown in dark blue. Women who present having had UPSI during the mid cycle period must be advised of the risk of EC failure supplied and also be referred for IUD insertion Note: Coils can be fitted up to 5 days post UPSI and also up to 5 days after the earliest possible ovulation, so UPSI on day 8/ 9/10/11 etc (of a 28 day cycle ) can still have a coil up to day 19 even if they have had repeated UPSI. (Bar chart could be used to help show this) Appendix 2 Emergency contraception decision guide for community pharmacists (based on FSRH review document http://www.fsrh.org/pdfs/FSRH_ECDecisionGuide.pdf)