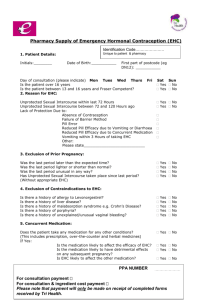
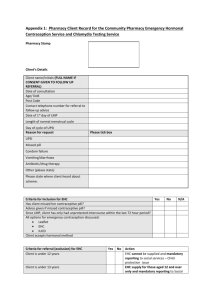
ehc consultation form
advertisement

Record of individual consultation for supply of progestogen only emergency contraception under community pharmacy PGD Date: Time: Client details Name: Address: Postcode: Date of birth: Registered GP: Current medication: Current conditions: Confidentiality Discussed Yes/No Reason for client requesting consultation for EHC Please give a brief summary of reason: Consultation outcome EHC required: YES/NO If no, please state reason why and advice given: MEDICINE SUPPLIED Levonorgestrel YES/ NO BATCH NUMBER: EXPIRY DATE: YES/ NO BATCH NUMBER: EXPIRY DATE: YES/ NO BATCH NUMBER: EXPIRY DATE: 1500mcg tablet Levonelle (Schering) Upostelle (Consilient) If no please state reason why it was not supplied, the advice given and action taken: Name of Pharmacist: GPHC number: Pharmacist Signature: Date: Inclusion and exclusion criteria Refer if NO to one of more of the following Unprotected sex/contraception failure within last 72 hours: Yes/No First episode (only occasion) of UPSI since last menstrual period: Yes/No Vomited within two hours of ingestion of first supply of EHC: Yes/No 13 years old or over: Yes/No If under 16 years of age and fulfils Fraser guidelines: Yes/No Refer if YES to one or more of the following: 1 Not present in person Yes/No Previously taken EHC within current cycle Yes/No Experiencing diarrhoea/vomiting: Yes/No 21 days or less post-partum (if applicable) Yes/No Last period unusually light, heavy or missed@ Yes/No One or more contra-indications to Levonelle: (severe liver dysfunction, malabsorption Yes/No syndromes, known hypersensitivity to Levonorgestrel or any of the ingredients of the product. Acute porphyrias, severe liver disease, Gastric bypass surgery (with exception of gastic band). Ulipristal administered within previous 9 days. Experiences previous severe clinical problems with POEC (excluding nausea). Taking other medications that significantly interact with EHC: Yes/No Likely to be pregnant Yes/No Advice provided (tick box if advice relevant and provided Oral and IUD Methods: Yes/No Mode of action: Yes/No Efficacy / failure rate: Yes/No Dose / how to take; Yes/No Side- effects: Yes/No Risk of ectopic pregnancy: Yes/No Actions to be taken if abdominal pain or heavy bleeding: Yes/No Actions to be taken if vomiting occurs within two hours: Yes/No Timing of next period (early, late or usual): Yes/No Contraception advice (immediate or remainder of cycle): Yes/No Contraceptive advice (future or longer term): Yes/No Condom use discussed Yes/No Risks of sexually transmitted disease / advice: Yes/No Information on sign posting to Sexual Health service (Telephone 0333 000 0014) Yes/No Chlamydia screening testing kit issued (not all people have symptoms): ACTIVITY Yes/No FUNDED IF DECLINED TEST REASON WHY: □ No change of partner since last test □ Not Sexually Active □ Tested elsewhere □ No reason given □ Not enough time since last test □ Not appropriate □ N/A Test Given Inform GP if taking warfarin (with patients consent) C Card scheme offered (ACCREDITED PHARMACIES ONLY (13-24 of age); Yes/No ACCEPTED C CARD (complete C Card Paperwork) Yes/No IF DECLINED C CARD REASON WHY: □ Over 24years old contraception □ No reason given □ Previous use of EHC □ Consent to treat 2 □ Alternative method of