Patients 16 years and above
advertisement

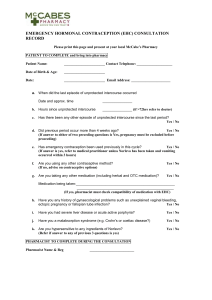
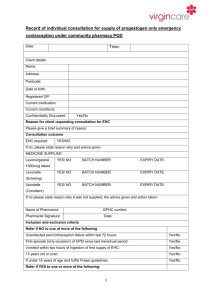
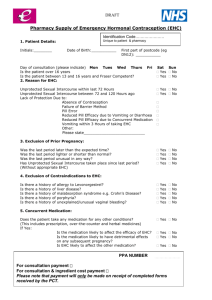
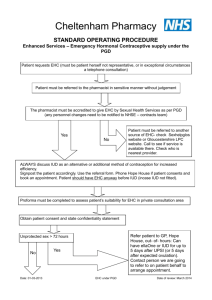
Appendix 2 (page 1 of 2) Emergency Hormonal Contraception (EHC) Patient Group Direction (PGD) Checklist Client’s name (optional) _____________________________________ The following information must be completed: Age/DOB _______________ Full postcode _______________ Date of Consultation _______________ Before EHC is offered complete the following checklist Tick Determine reason for request for emergency hormonal contraception Check exclusion criteria in PGD UPSI since LMP (> 72 hours ago and EHC not taken in last 12 hours) EXCLUDE PREGNANCY U 16 (not Fraser competent) Hypersensitivity to progestogens or any ingredient Does the client have breast cancer? Does the client have severe liver disease? Rare hereditary problems of glucose/galactose metabolism, severe malabsorption states Are any medicines being taken, including prescription and nonprescription medication, to ensure no exclusion? Estimate likely date of ovulation and risk of pregnancy by recording: Client’s History Date of first day of LMP______________________ day of cycle___________ Length of normal menstrual cycle _________ Was LMP in any way abnormal? Yes / No Hours since condom accident /unprotected sex _____________ Timing of all inadequately protected intercourse (including any missed pill history and intercourse during a lengthened pill-free interval) – which day(s) of the current cycle? _____________________________________________________________________ _____________________________________________________________________ _____________________________________________________________________ If EHC was given for any previous episodes of unprotected intercourse this cycle, which and when ____________________________________________________ Result of pregnancy test if performed (if LMP was missed altered) Positive / Negative / Not done Appendix 2 (page 2 of 2) COUNSELLING Yes Mode of action, Side effects and risks discussed Possible effects on foetus discussed & possible effects on menstrual cycle. Effectiveness including failure rate discussed Discuss future contraception and if appropriate arrange for the next cycle Give relevant client leaflet, FPA leaflet and manufacturer’s product information within the pack. Discuss the need to abstain from sexual intercourse or use of a barrier method correctly and consistently for the remainder of the current menstrual cycle as EHC does not provide contraceptive cover for the remainder of the cycle Advise of the possibility of an ectopic pregnancy if the method should fail Discuss safe sex, breast awareness, cervical screening and other health promotion issues Clients under the age of 16 years must be counselled / assessed using Fraser Guidelines Check client’s understanding of the method, and willingness to use Dose taken on premises Summary Less than 72 hours since first episode of unprotected intercourse Explain method options, to include the better efficacy of an IUD and the fact that EHC is not as effective as conventional, regular use of hormonal contraceptives and is suitable only as an emergency measure Discuss future contraception – LARC and risk of STIs Signpost for LARC (GP/CASH) Client prefers and accepts hormonal method Supplied: Levonelle® 1500 microgram tablets (1500 micrograms Levonorgestrel) Batch number No Tick Yes / No (Advice only) Expiry date _______________ Referred to GP / CASH for LARC/ Yes / No Action Taken: The above information is correct to the best of my knowledge. I have been counselled on the use of emergency contraception and understand the advice given to me by the Pharmacist. Clients Signature: _____________________________ Date _____________ The action specified was based on the information given to me by the client, which, to the best of my knowledge, is correct. Name of Pharmacist ___________________________ Date _____________ For those signed up to offering clients Chlamydia testing kits, please discuss this issue if the patient meets the inclusion criteria as per the SLA.