Procrit (epoetin) Anemia Management Orders
advertisement
 Anemia Management Orders")
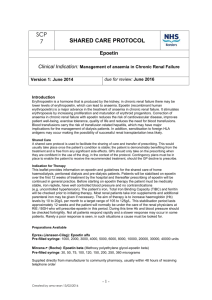
PLACE LABEL HERE PROCRIT (epoetin) ANEMIA MANAGEMENT ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). 1. Laboratory: Anemia Profile, if not already available this admission 2. Indication/Dose: Procrit (epoetin) is available in limited vials sizes; round to nearest vial size as below ONE TIME DOSES ARE ONLY ALLOWED TO BE ORDERED BY A NEPHROLOGIST End Stage Renal Disease (with HGB < 10 g/dL) Must be ordered by a Nephrologist Limit of 30,000 units weekly, (exception if outpatient dialysis records indicate higher dose necessary) Hold Procrit dose for Hemoglobin > 11. Choose Dose Route Procrit (epoetin) 2,000 units Procrit (epoetin) 4,000 units Procrit (epoetin) 8,000 units Procrit (epoetin) 10,000 units Procrit (epoetin) 20,000 units SQ Choose Frequency (MAX: 30,000 units per week) every Mon-Wed-Fri (limit 10,000 units/dose) every Tue-Thur-Sat (limit 10,000 units/dose) twice weekly every _________ (limit 14,000 units/dose) weekly every ______________ (limit 30,000 units/dose) Chronic Kidney Disease: Pre-Dialysis (Stage III or IV) (HGB < 10 g/dL) Must be ordered by a Nephrologist Procrit (epoetin) 4,000 units Procrit (epoetin) 10,000 units SQ SQ q 7 days q 7 days Anemia from concomitant chemotherapy for nonmyeloid malignancies (HGB < 10 g/dL) Must be ordered by Oncologist/Hematologist and the following MUST be met before dispensing: Pharmacist to confirm that the ordering physician is an ESI APPRISE Oncology Program enrolled provider Nurse to contirm that the ESA APPRISE Patient Education Acknowledgement Form (consent) has been signed by patient and physician and a copy placed in the medical record and sent to Pharmacy. Procrit (epoetin) 40,000 units Procrit (epoetin) 10,000 units SQ SQ Once weekly starting________________________________ Three times a week on Mon-Wed-Fri or Tue-Thur-Sat Trauma (HGB < 10 g/dL) Must be ordered by a Trauma Surgeon If < 40 kg: Procrit (epoetin) 20,000 units SQ once weekly If 41-99 kg: Procrit (epoetin) 40,000 units SQ once weekly If > 100 kg: Procrit (epoetin) 60,000 units SQ once weekly Transfusion NOT an option (HGB <8 g/dL with normal anemia profile) No physician speciality restriction If < 40 kg: Procrit (epoetin) 20,000 units SQ once weekly If 41-99 kg: Procrit (epoetin) 40,000 units SQ once weekly If > 100 kg: Procrit (epoetin) 60,000 units SQ once weekly Continuation of prior therapy: No physician speciality restriction Procrit (epoetin) ____________ units SQ every __________________________ 3. Nurse to give Procrit Medication Guide to patient for review and document in the medical record 4. Iron Replacement: Ferrous Sulfate (iron) 325 mg po tid Ferrlicet (ferric gluconate) 62.5 mg 125 mg 250 mg IVPB x ____ doses ______________ Date __________________ Time *1-26579* _________________________________ Physician Signature FORM 1-26579 REV. 04/2014 WHITE: Medical Record CANARY: Pharmacy ___________ PID Number Page 1 of 1