Guidelines of Erythropoietin Therapy in Chronic Kidney Disease
advertisement

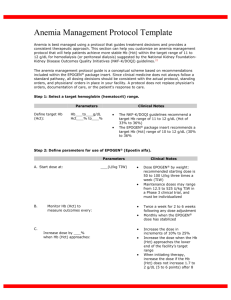
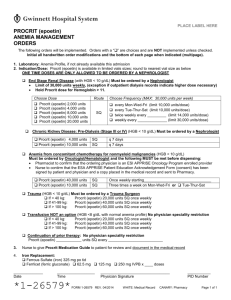
Guidelines of Erythropoietin Therapy in Chronic Kidney Disease Patients A. when to initiate anemia work-up in chronic kidney disease (CKD) patients: 1. Hgb < 11 g/dl , Hct <33% in pre-menopausal females and pre-pubertal patients 2. Hgb < 12 g/dl, Hct < 37% in adult males and post-menopausal females B. The following work-up should be performed before Erythropoietin (Epoetin) therapy is begun: 1. 2. 3. 4. Hgb and/or Hct RBC indices Reticulocyte count Iron parameters: - serum iron (50-160mcg/dl) - total iron binding capacity (TIBC) (250-400mcg/dl) - percent transferring saturation (TSAT) (20-40%) - Serum ferritin (F=12-150ng/ml, M=15-200ng/ml) 5. A test for occult blood in stool C. Correct any iron deficiency anemia if present with iron supplement. D. If no cause for anemia other than chronic kidney disease is detected, based on the previous work-up, and serum creatinine is ≥ 2 mg/dl, anemia is most likely due to Erythropoietin deficiency. - See figure number 1- E. Administration of Epoetin 1. Epoetin should be given subcutaneously (SC) in CKD and peritoneal dialysis patients. 2. The most effective route of Epoetin administration is SC in hemodialysis patients 3. When Epoetin is given SC, the site of injection should be rotated with each administration. 4. The SC adult dose should be 80-120 units/kg/wk in 2-3 divided doses. 5. Pediatric patients < 5 years old frequently require higher doses ( 300 units/kg/wk) than older pediatric patients and adults. 6. If the initial administration of Epoetin is IV for hemodialysis patients, the dose should be 120-180 units/kg/wk given in three divided doses (50% higher than the SC dose). 7. For hemodialysis patients who are being switched from IV to SC administration of Epoetin but have not yet achieved the target 1 Hgb/Hct, the total weekly IV dose should be administered SC in two to three divided doses. For those achieving the target Hgb/Hct, the initial weekly SC dose should be two-thirds the weekly IV dose. F. Monitoring and titration of Epoetin therapy 1. Hgb/Hct should be measured every 1-2 weeks following initiation of treatment or following a dose increase or decrease, until a stable target Hgb/Hct and Epoetin dose have been achieved. 2. Once a stable target Hgb/Hct and Epoetin dose have been achieved, Hgb/Hct should be monitored every 2-4 weeks. 3. The target range for hemoglobin and hematocrit should be 11-12 g/dl and 33%-36%, respectively. 4. The target range for TSAT and serum ferritin should be ≥20% and ≥100ng/ml, respectively. 5. If Hct level increased by < 2 percentage points over a 2-4-week period, increase the Epoetin dose by 50%. 6. If Hct level increased by 8% per month, or if exceeds the target level reduce the dose of Epoetin by 25%. 7. For peritoneal dialysis patients in whom SC or IV administration of Epoetin is not feasible, intraperitoneal (IP) administration may be considered. IP administration must be done into a dry abdomen or one with a minimal amount of dialysate. 8. Blood pressure should be monitored in all patients with CKD, particularly during initiation of Epoetin therapy. 2 Serum creatinine ≥ 2mg/dl? Yes Check Hgb No ≤12.5 (♂, postmenopausal ♀) ≤ 11 (♀/prepubertal)? No work-up Yes Work-up CBC, indices, Retics, iron,TIBC,Fe,TSAT,Ferritin , stool guaiac Refer for hematology work-up No Normal? No Yes No Treat with Epoetin if indicated Treat with iron Anemia not corrected 3 Fe deficiency? Anemia corrected; periodic follow-up Figure 1. Anemia workup for CKD patients Iron Support Guidlines Iron supplementation usually is essential to assure an adequate response to Epoetin in patients with CKD because the demands for iron by the erythroid marrow frequently exceed the amount of iron that is immediately available for erythropoiesis ( as measured by percent transferrin saturation) as well as iron stores ( as measured by serum ferritin. These guidelines suggest that the regular use of small doses of intravenous iron (IV), particularly in the hemodialysis patients, will prevent iron deficiency and promote better erythropoiesis than can oral iron therapy. 1. To achieve and maintain an Hgb 11 to 12 g/dl ( Hct of 33% to 36%), most hemodialysis patients will require intravenous iron on a regular basis. 2. The adult CKD, home hemodialysis, and peritoneal dialysis patient may need 500 to 1000 mg of iron dextran administered IV in a single infusion, and repeated as needed. 3. The Anemia Work Group recommends for administering IV iron dextran or iron gluconate in adult hemodialysis patients with absolute iron deficiency ( TSAT is < 20% and/or the serum ferritin is < 100 ng/ml) is 100 mg of iron dextran or 125 mg of iron gluconate during each dialysis for 10 or 8 doses respectively. 4. For maintenance iron therapy, treatment, and prevention of functional iron deficiency ( once the patient’s TSAT is ≥20% and the serum ferritin is ≥100 ng/ml), the recommendation is 25 to 100 mg of intravenous dextran every week for 10 weeks, or 31.25 to 125 mg of iron gluconate every week for 8 weeks, with measurement of TSAT and serum ferritin no sooner than 2 to 7 days after the last dose, depending on the magnitude of the above doses. Doses of 100 to 125 mg require 7 days to elapse for accurate monitoring. Measurement of TSAT and serum ferritin may be inaccurate if they are performed within 14 days of receiving a single dose of 1 gram or more of iron intravenously. 5. In patients in whom TSAT is ≥50% and/or serum ferritin is ≥800ng/ml, IV iron should be withheld for up to 3 months, at which time the iron parameters should be re-measured before IV iron is resumed. When TSAT and serum ferritin have fallen to ≤50% and ≤800ng/ml, IV iron can be resumed weekly at a dose reduced by one third to one half. Monitoring Iron Status 1. During the initiation of Epoetin therapy and while increasing the Epoetin dose in order to achieve an increase in Hgb/Hct, The TSAT and the serum ferritin should be checked every month in patients not receiving IV iron, and at least once every 3 months in patients receiving IV iron, until target Hgb/Hct is reached. 4 2. Following attainment of the target Hgb/Hct, TSAT and serum ferritin should be determined at least once every 3 months. Reference: National Kidney Foundation. K/DOQI. Clinical practice guidelines for anemia of chronic kidney disease. Am J Kidney Dis 2001;37:s182-s238. 5