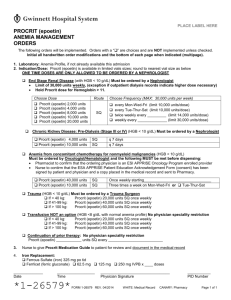
Epogen/Procrit® epoetin alfa
advertisement

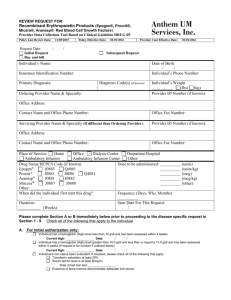
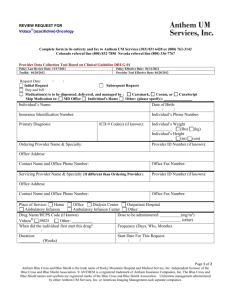
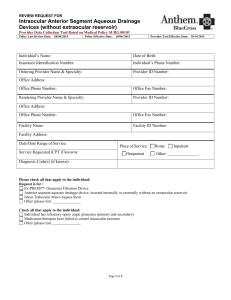
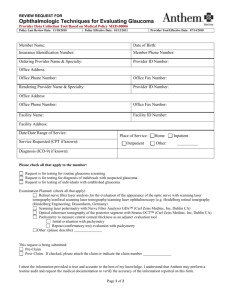
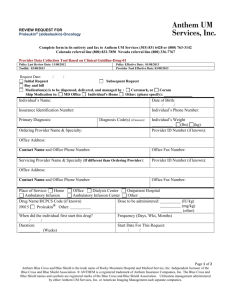
REVIEW REQUEST FOR Epogen/Procrit® (epoetin alfa), Aranesp® (darbepoetin alfa), Omontys® (peginesatide) Red Blood Cell Growth Factors Complete form in its entirety and fax to: Anthem Blue Cross 866-408-7195 Provider Data Collection Tool Based on Clinical Guideline DRUG-05 Policy Last Review Date: 05/09/2013 Request Date: Initial Request Buy and bill / Policy Effective Date: 07/09/2013 Provider Tool Effective Date: 07/09/2013 / Subsequent Request Individual’s Name: Date of Birth: / / Individual’s Phone Number: Insurance Identification Number: Primary Diagnosis: ICD-9 Code(s) (if known): Ordering Provider Name & Specialty: Individual’s Weight (lbs) (kg) Provider Tax ID or NPI Number: Office Address: Contact Name and Office Phone Number: Office Fax Number: Servicing Provider Name & Specialty (If different than Ordering Provider): Provider Tax ID or NPI Number: Office Address: Contact Name and Office Phone Number: Office Fax Number: Place of Service: Home Office Dialysis Center Outpatient Hospital Ambulatory Infusion Ambulatory Infusion Center Other: Drug Name/HCPCS Code (if known) Dose to be administered: Epogen® J0885 J0886 Q4081 Procrit® J0885 J0886 Q4081 Aranesp® J0881 J0882 Omontys® J0890 Other: When did the individual first start this drug? Frequency (Days, Wks, Months) / / Duration: Start Date For This Request: (Weeks) / / (units) (units/kg) (mcg) (mcg/kg) (mg/kg) (other) Please complete Section A or B immediately below prior to proceeding to the disease specific request in Section 1 - 9 A. For initial authorization only: Individual has a hemoglobin (Hgb) level less than 10 g/dl and has been assessed within 4 weeks Current Hgb: Date: / / (section A continues below) Anthem Blue Cross is the trade name of Blue Cross of California. Anthem Blue Cross and Anthem Blue Cross Life and Health Insurance Company are independent licensees of the Blue Cross Association. ®ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross name and symbol are registered marks of the Blue Cross Association. Page 1 of 3 Individual has a hemoglobin (Hgb) level greater than 10.0 g/dl and less than or equal to 13.0 g/dl and has been assessed within 4 weeks (if request is for number 5 outlined below) Current Hgb: Date: / / Individual’s iron status been evaluated. If checked, please check all of the following that apply: Transferrin saturation at least 20% Serum ferritin level is at least 80ng/ml Date of last Iron test: Evidence of bone marrow demonstrates adequate iron stores Individual’s endogenous erythropoietin level less than 500 mU/ml (ONLY NEED TO COMPLETE IF REQUEST IS FOR NUMBER 3 or 4 OUTLINED BELOW) Individual does NOT have uncontrolled hypertension B.For Re-authorization only: Individual does NOT have uncontrolled hypertension? Individual responded to previous treatment with Epogen®, Procrit®, Aranesp® or Omontys® Individual has a hemoglobin (Hgb) level less than or equal to 11.0 g/dl and has been assessed within 4 weeks Current Hgb: Date: / / Epogen®/Procrit®, Aranesp®, Omontys®: (1) Anemia of Chronic Kidney Disease (CKD) For anemia of chronic kidney disease Individual is on dialysis Other m Epogen®/Procrit®, Aranesp®: (2) Anemia in Individuals on Chemotherapy Individual has anemia and on chemotherapy Chemotherapy planned for a minimum of 2 months Individual has a diagnosis of non-myeloid cancer The anticipated outcome not a cure Other (3) Anemia in Myelodysplastic Syndrome For anemia in Myelodysplastic syndrome Other Epogen®/Procrit®: (4) Anemia in Zidovudine Treated human immunodeficiency virus (HIV)-Infected Individuals For anemia in Zidovudine treated human immunodeficiency virus (HIV) – infected individual Individual’s current Zidovudine dose is 4200mg/week or less Other (5) Anemia in Reduction of Allogeneic Blood Transfusion in Pre-Operative Surgery Individuals For anemia and reduction of allogeneic blood transfusion in pre-operative surgery individual Individual is scheduled for elective, noncardiac, nonvascular surgery Individual is at high risk for perioperative transfusions with significant anticipated blood loss Individual is unable or unwilling to donate autologous blood Antithrombotic prophylaxis has been considered Other (6) Anemia in Individuals with Hepatitis C For anemia in individual with hepatitis C Individual is currently on concomitant therapy of ribavirin plus interferon alfa or peginterferon alfa Other (7) Chronic Inflammatory Disease Individual has chronic inflammatory disease Individual is currently on myelosuppresive drugs (e.g. disease modifying anti-rheumatic drugs) known to produce anemia Other Anthem Blue Cross is the trade name of Blue Cross of California. Anthem Blue Cross and Anthem Blue Cross Life and Health Insurance Company are independent licensees of the Blue Cross Association. ®ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross name and symbol are registered marks of the Blue Cross Association. Page 2 of 3 (8) Allogeneic Bone Marrow Transplant Individual has allogeneic bone marrow transplantation Other (9) Other Use(s) (Please submit all supporting documents including labs, progress notes, imaging, etc., for review.) This request is being submitted: Pre-Claim Post–Claim. If checked, please attach the claim or indicate the claim number I attest the information provided is true and accurate to the best of my knowledge. I understand that the health plan or its designees may perform a routine audit and request the medical documentation to verify the accuracy of the information reported on this form. / / Name & Title of Provider or Provider Representative Completing Form Date & attestation (Please Print)* *The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted Anthem Blue Cross is the trade name of Blue Cross of California. Anthem Blue Cross and Anthem Blue Cross Life and Health Insurance Company are independent licensees of the Blue Cross Association. ®ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross name and symbol are registered marks of the Blue Cross Association. Page 3 of 3