gc_EGYPT - jeans4genes.org
advertisement

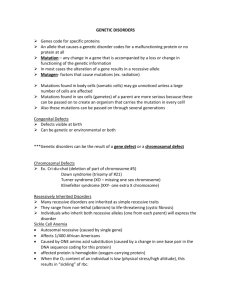
Eastern Mediterranean Health Journal | Back to Health Journal page | Health Journal back issues | Home Autosomal recessive disorders among patients attending the genetics clinic in Alexandria Volume 4, Issue 3, 1998, Page 470-479 M.M. Mokhtar, S.M. Kotb and S.R. Ismail ABSTRACT A total of 660 patients referred to the genetics clinic, Medical Research Institute, Alexandria were assessed to determine the frequency of genetic disorders and the proportion of autosomal recessive disorders. It was found that 298 (45.2%) patients had genetic disorders, 100 (33.6%) of whom had an autosomal recessive disorder; these included 32 patients with metabolic defects, 18 with haemoglobinopathies and 50 with syndromes and single defects. The frequency of consanguinity among parents of patients with autosomal recessive disorders was high (60%, with 48% first cousins). The average inbreeding coefficient was higher (0.03) than that reported for the Egyptian population in general (0.01). Maladies autosomiques récessives chez des patients consultant dans un service de génétique à Alexandrie REsumE Un nombre total de 660 patients qui avaient été orientés vers le service de génétique de l'Institut de Recherche médicale d'Alexandrie a fait l'objet d'une évaluation visant à déterminer la fréquence des maladies génétiques et la proportion des maladies autosomiques récessives. On a constaté que 298 patients (45,2%) présentaient des maladies génétiques dont 100 (33,6%) une maladie autosomique récessive; parmi ces derniers, 32 patients avaient des anomalies du métabolisme, 18 des hémoglobinopathies et 50 des syndromes ou des anomalies simples. La fréquence de la consanguinité chez les parents des patients présentant des maladies autosomiques récessives était élevée (60%, avec 48% de cousins germains). Le coefficient de consanguinité moyen était plus élevé (0,03) que celui rapporté pour la population égyptienne en général (0,01). Introduction It is a useful concept to consider all diseases as being on a spectrum. At one extreme we have those disorders which are largely environmental in cause; at the other extreme we have those disorders which are largely genetic [1]. A number of surveys have indicated that globally at least 2 per 1000 neonates have autosomal recessive disorders, 2-10 per 1000 have autosomal dominant disorders, 1-2 per 1000 have X-linked recessive disorders, 6-7 per 1000 have chromosomal abnormalities and about 20 per 1000 have congenital malformations [2]. A recent publication on genetic disorders among Arab populations lists 115 new genetic syndromes reported over the past two decades. Of these, 100 syndromes are autosomal recessive, 10 are autosomal dominant and 5 possibly X-linked recessive or autosomal recessive [3]. Autosomal recessive disorders are generally severe; many inborn errors of metabolism and malformation syndromes are due to autosomal recessive genes and their recognition in the first affected individual in a family is of great importance as the recurrence risks are often high and the disorders are frequently untreatable [2]. Recessively inherited disorders account for a substantial proportion of mental and physical handicaps in some countries. Similarly, children of consanguineous parents may be overrepresented in patients with severe mental retardation, blindness, hearing impairment and deaf-mutism [3]. The aims of this work were to obtain baseline information on the frequency of genetic disorders among a group of patients attending the genetics clinic of the Medical Research Institute, Alexandria University, to classify and estimate the proportion of autosomal recessive disorders and to determine the relationship between the disorders diagnosed and the inbreeding coefficient. Patients and methods The study included all patients (660) attending the human genetics clinic of the Medical Research Institute, Alexandria University, during the two-year period, 1995 and 1996. They were referred from paediatric hospitals and private clinics and the reasons for the referrals are given in Table 1. Accurate diagnosis was made after the following had been carried out: taking of the complete genetic and family history, pedigree construction, clinical genetic examination and anthropometric measurements. Other investigations were carried out depending on the individual patient, such as skeletal survey, ultrasound, electroencephalogram, hearing tests and fundus examination. Laboratory studies were carried out as appropriate and included biochemical screening tests and thin-layer chromatography, determination of haemoglobin level and red cell morphology, absolute red cell indices, haemoglobin electrophoresis, chromosomal analysis, consanguinity and inbreeding coefficient evaluation. Results Genetic disorders Of the 660 patients, genetic disorders were detected in 298 (45.2%); of these 100 (33.6%) had autosomal recessive disorders, 40 (13.4%) had autosomal dominant disorders, 20 (6.7%) had X-linked disorders, 15 (5.0%) had multifactorial disorders, 55 (18.4%) had chromosomal abnormalities, 10 (3.4%) were due to teratogens and 58 (19.5%) were sporadic. The remaining 362 (54.8%) patients were found to have no disorder of genetic or known environmental cause (Tables 2 and 3). Autosomal recessive disorders Table 4 shows the classification of the 100 patients with autosomal recessive disorders. Group I consisted of 32 patients (4.8%) with metabolic defects. Among those, 22 patients (3.3%) had aminoacidopathies and 10 (1.5%) had mucopolysaccharidoses. Group II consisted of 18 patients (2.7%) with haemoglobinopathies. Of these, 10 (1.5%) had bthalassaemia major and 8 (1.2%) had sickle-cell anemia. Group III consisted of 50 patients (7.6%) with syndromes and single defects. Microcephaly, with or without spastic quadriplegia, congenital deafness and spinal muscle atrophy (infantile and juvenile) were the most common conditions in this group (Table 5). The rare specific syndromes are also shown in Table 5. Family history Affected siblings were found in 18 (56.3%) families with metabolic defects. Of those patients with haemoglobinopathies, 12 (66.7%) had affected siblings. In group III, affected siblings were found in one patient with xeroderma pigmentosa, one with ataxia-telangectasia, one with multiple pterygium syndrome, two cases with microcephaly and all cases with deafness. A positive family history was present in one case of ectodermal dysplasia and in all cases with spinal muscle atrophy and Robinow syndrome (Table 4). Consanguinity and inbreeding coefficient Table 6 shows that parental consanguinity was 60% among cases with autosomal recessive disorders (48% for first cousin). This value was significantly higher than that of the general population (28.9%) (c2 = 32.9, P < 0.01). Parental consanguinity was 68.8% among cases with metabolic defects, 66.7% among cases with haemoglobinopathies and 52% among syndromes and single defects. These values were significantly higher than those of the general population.(c2 = 22.4, 15.7 and 12.8 respectively, P < 0.01). The average inbreeding coefficient in the genetic disorders is shown in Table 7. Discussion A study similar to ours conducted in Kuwait amongst 1300 patients referred to general genetics clinics showed that 32% of the total referred cases were autosomal recessive, 30% had chromosomal abberations, 13% had known multifactorial and polygenic disorders, 8% had autosomal dominant disorders, 2% had X-linked disorders and 15% had unknown disorders [4]. In our study, 45.2% of the patients had genetic defects. This figure is higher than that reported in a similar study by Devi et al (15.5%) in India [5], but Arabs appear to have a high frequency of genetic disorders and in particular autosomal recessive traits [4]. The frequency of single gene disorders in this study was 53.7%. This value is lower than that reported by Devi et al (63.5%) [5] and Teebi (57%) [4]. However, it is higher than that reported by Hoodfar and Teebi (32.5% among cases of Middle Eastern origin) [6]. This might be due to differences in the level of consanguineous marriage and the geographical distribution among these populations. The frequency of autosomal recessive disorders in our study was 33.6%. This is lower than that reported by Devi and colleagues (38.1%) [5] and Teebi (45%) [4], but higher than that reported by Hoodfar and Teebi (14.5%) in a Middle Eastern population in a western city [6]. This is probably related to consanguinity. Metabolic disorders are individually rare but collectively numerous with wide variations in their frequencies among cases with mental retardation in different surveys. Wuu et al. reported 0.5% metabolic defects among 1248 cases with mental retardation in Taiwan [7]. Henderson et al. reported a frequency of 0.6% in a survey of 1087 cases with mental retardation in South Africa [8]. Tayel et al. found a frequency of 22% in children in Egypt [9]. In the present study the frequency was 4.8%. This value is lower than that reported by Devi and colleagues (6.4%) [5]. These variations could be due to the selection of the cases referred. Aminoacidopathies are one of the major causes for psychomotor retardation [2]. Their frequency among mentally retarded patients varies from 2.5% to 39% in different studies [912]. In the present study it was 2.7%. This value agrees with the result reported by Devi et al. (2.7%) [5]. Mucopolysaccharidoses (MPS) are a group of inherited disorders of metabolism with varying clinical manifestations [13]. There are wide variations in the frequency of MPS among mentally retarded children as reported by different researchers [14-16]. Piraud et al. studied 2000 patients in France and found MPS in 170 cases (8.5%) [14], Di Natale et al. evaluated 297 patients in Italy and found MPS in 147 cases (16.2%) [15] and Michelakakis et al. studied 2745 patients in Greece and found MPS in 36 cases (1.3%) [16]. In the present study, MPS was detected in 1.5% of cases while Devi et al. reported a frequency of 1% among 407 cases included in their study [5]. There is considerable ethnic and geographical variation in the incidence, frequency and distribution of haemoglobin disorders [17]. Thalassaemia, sickle-cell anaemia and glucose-6phosphate dehydrogenase (G6PD) deficiency are the commonest single gene disorders encountered in the Eastern Mediterranean Region. The epidemiology of these disorders shows marked intracountry as well as intercountry differences. The percentage of bthalassaemia trait ranges from 1% to 6% in the Eastern Mediterranean Region as assessed through neonatal screening [17]. Our study found 10 cases (1.5%) with b-thalassaemia major. The frequency of sickle-cell anaemia is reported to vary between 1.2% and 2.1% among neonates in the Libyan Arab Jamahiriya [18]. Only 1.2% of patients in our study had sicklecell anaemia. In the present study, syndromes and single defects constituted 50% of cases with autosomal recessive disorders. Reports from countries in the Eastern Mediterranean Region have pointed to higher frequencies of various autosomal recessive syndromes [3]. Microcephaly, with or without spastic quadriplegia, had a high frequency (12/50, 24%). Microcephaly without spasticity is the uncomplicated autosomal recessive type. Microcephaly with seizures and spasticity was the most common type of genetic microcephaly reported by Tolmie et al. in Scotland [19], which is what we found in our study. Congenital deafness was a relatively common condition found in this study (5/50; 10%). Deafness has a remarkable genetic heterogeneity [20]. The presence of consanguinity and more than one affected member in the family indicates an autosomal recessive type of congenital deafness. The age of onset is the main feature which distinguishes the infantile and juvenile types of spinal muscle atrophy. In this study, the infantile type (5/50, 10%) was more frequent than the juvenile (2/50, 4%). This could be due to the early onset of manifestations in the infantile type. All cases had a family history of the disease. Xeroderma pigmentosa (XP), Fanconi anaemia (FA) and ataxia-telangectasia (AT) are a group of autosomal recessive disorders (chromosomal breakage syndromes), characterized by defective DNA repair and increased chromosomal breaks [2]. XP is the commonest of these disorders and the most intensively studied [2]. In the present study, XP was more frequent (4/9, 44.4%) than other types of chromosomal breakage syndromes (FA: 3/9, 33.3% and AT: 2/9, 22.2%) and this concurs with previous reports [2, 21]. Although sex-linked inherited ectodermal dysplasia is the most common type, a rare autosomal recessive form of anhydrotic or hypohydrotic ectodermal dysplasia exists [20]. In this work two patients had the autosomal recessive type of ectodermal dysplasia. A recessive type of multiple pterygium syndrome was reported in the present study. Several cases have been reported and all had consanguineous parents [20,22], which was also found in our study. Retinitis pigmentosa unassociated with other abnormalities is inherited most frequently as an autosomal recessive disorder. In our study, two patients were diagnosed as autosomal recessive retinitis pigmentosa. Friedreich ataxia is one of the rare spinocerebellar degenerative disorders. We found two patients with this disorder. Two patients were diagnosed with optic atrophy. Autosomal recessive congenital optic atrophy is very rare. The profound bilateral vision loss is stable and usually associated with nystagmus [23]. Parental consanguinity has been found in 50% of the cases [23]. Our findings concur with this. Spastic paraplegia is a relatively non-specific manifestation. A recessively inherited spastic paraplegia is rare [20]. Two patients with spastic paraplegia were detected in the present study. Other syndromes and diseases were less frequent and represented by one patient (Table 5). Bardet-Biedl syndrome is differentiated from Laurence Moon syndrome by the presence of polydactyly, obesity and the absence of spastic paraplagia [20]. Carpenter syndrome is a rare autosomal recessive acrocephalopoly syndactyly [29]. Robinow syndrome is usually a dominant disease [20], but a rare recessive form is suggested by the reports of Saal et al. [24]. The patient in this study had a positive history, two siblings affected and the parents were consanguineous. SHORT syndrome is characterized by short stature, hyperextensibility of joints, ocular depression, Rieger anomaly and teething delay. It is inherited as an autosomal recessive disorder [20]. Diastrophic dysplasia is a form of dwarfism associated with clubbed feet, malformed pinna, calcification of cartilage and hitchhiker thumb [20]. These characteristics were found in the patient in our study. Consanguineous mating is genetically important as closely related individuals have a higher chance of carrying the same alleles than unrelated individuals; hence the offspring of consanguineous mating are more frequently homozygous for various alleles than those from other unions [1]. The rate of consanguinity among parents of patients with autosomal recessive disorders in the present study was higher (60%) than that of the general population in Egypt (28.9%) [25]. This concurs with Hoodfar and Teebi who found that autosomal recessive disorders were more than twice as common in inbred families than in non-inbred ones [6]. The rate of firstcousin marriages was high (48%) when compared with 14% in the general population [25]. This is in agreement with the findings of Roberts and Pembry in a Middle East sample [26] and Orioli et al. in a South American sample [27]. In addition, the consanguinity level was highest in the autosomal recessive group when compared with other genetic conditions in our study (Tables 6 and 7). Autosomal recessive disorders have a high risk of recurrence. This was evident in the present study as 49% of the patients had a positive family history (33% had positive consanguinity and 16% were non-consanguineous). This illustrates the role of consanguinity in increasing the incidence of autosomal recessive diseases in a population. The average coefficient of inbreeding in cases with autosomal recessive diseases was found to be high (0.03), which is almost triple that of the Egyptian population in general (0.01) [25]. Inbreeding in itself is not responsible for the appearance of unfavourable phenotypes. However, it tends to reveal deleterious recessive alleles present in heterozygous carriers and hence consanguinity will lead to increased frequencies of homozygotes for rare alleles [1]. Conclusion An understanding of the factors influencing the genetic disease profile of a population is important. Our study found that the frequency of genetic disorders among cases referred to our clinic was 45.2%. Autosomal recessive diseases accounted for 33.6% of these disorders. Consanguinity and the average inbreeding coefficient among parents of patients with autosomal recessive disorders were high (60% and 0.03 respectively). These findings are crucial for geneticists and genetic counsellors in their evaluation, diagnosis, counselling and management of patients. Acknowledgements We would like to thank all members of the Human Genetics Department for their cooperation and efforts. References 1. Mueller RF, Young ID. Polygenic and multifactorial inheritance In: Mueller RF, Young ID, eds. Emery's elements of medical genetics. Edinburgh, Churchill Livingstone, 1995. 2. Kingston MH. Clinical genetic services. In: Kingston MH, ed. ABC of clinical genetics. London, British Medical Journal Publishing Group, 1994. 3. Teebi A, Farag T. Genetic disorders among Arab populations. Oxford monographs on medical genetics No.30. Oxford, Oxford University Press, 1996. 4. Teebi AS. Autosomal recessive disorders among Arabs: an overview from Kuwait. Journal of medical genetics, 1994, 31:224-33. 5. Devi AR, Rao NA, Bittles AH. Inbreeding and the incidence of childhood genetic disorders in Karnataka, South India. Journal of medical genetics, 1987, 24:362-5. 6. Hoodfar E, Teebi AS. Genetic referrals of Middle Eastern origin in a western city: inbreeding and disease profile. Journal of medical genetics, 1996, 33:212-5. 7. Wuu KD et al. Chromosomal and biochemical screening of mentally retarded schoolchildren in Taiwan. Paper presented at the 8th International Congress of Human Genetics, Washington DC, USA, 6-11 October 1991. 8. Henderson HE et al. Biochemical screening for inherited metabolic disorders in the mentally retarded. South African medical journal, 1981, 60(19):731-3. 9. Tayel JD et al. Metabolic screening of mentally retarded children in Egypt. Paper presented at the 38th Annual Meeting of the American Society of Human Genetics, San Diego, California, 7-10 October, 1987. 10. Subba YR. Amino acid disorders in mentally retarded children. Paper presented at the 8th International Congress of Human Genetics, Washington DC, USA, 6-11 October, 1991. 11. Yadav G et al. Aminoacidopathies among institutionalised mentally retarded in Kuwait. Clinical genetics, 1992, 42(4):212. 12. Bibhas KR et al. Screening for aminoacidopathies in mentally retarded children. Paper presented at the 8th International Congress of Human Genetics, Washington DC, USA, 6-11 October, 1991. 13. Moores C et al. Anaesthesia for children with mucopolysaccharidoses. Anaesthesia and intensive care, 1996, 24(4):459-63. 14. Piraud M et al. Diagnosis of mucopolysaccharidoses in a clinically selected population by urinary glycosaminoglycan analysis: a study of 2000 urine samples. Clinica chimica acta, 1993, 221(1-2):171-81. 15. Di Natale P et al. Biochemical diagnosis of mucopolysaccharidoses: experience of 297 diagnoses in a 15-year period (1977-1991). Journal of inherited metabolic disease, 1993, 16(2):473-83. 16. Michelakakis H et al. Lysosomal storage diseases in Greece. Genetic counselling, 1995, 6(1):43-7. 17. Alwan A, Modell B. Community control of genetic and congenital disorders. Alexandria, World Health Organization Regional Office for the Eastern Mediterranean, 1997 (EMRO Technical Publications Series, No. 24). 18. Sheriff S et al. A profile of abnormal haemoglobins in eastern and southern Libya. Saudi medical journal, 1989, 10:138-40. 19. Tolmie JL et al. Microcephaly: genetic counselling and antenatal diagnosis after the birth of an affected child. American journal of medical genetics, 1987, 27:583-94. 20. McKusick VA. In: McKusick VA, ed. Mendelian inheritance in man. Baltimore, Johns Hopkins University Press, 1994. 21. Kraemer KH, Lee MM, Scotto J. Xeroderma pigmentosum. Cutaneous, ocular and neurologic abnormalities in 830 published cases. Archives of dermatology, 1987, 123:241-50. 22. Hall JG et al. Limb pterygeum syndromes: a review and report of eleven patients. American journal of medical genetics, 1982, 12:377-409. 23. Heckenlively JR, Daiger SP. Hereditary retinal and choroidal degenerations. In: Emery and Rimion's principles and practice of medical genetics, 3rd ed. Edinburgh, Churchill Livingstone, 1997:2555-76. 24. Saal HM et al. Autosomal recessive Robinow syndrome: evidence for genetic heterogeneity. Paper presented at the 36th Annual Meeting of the American Society of Human Genetics, Salt Lake City, Utah, 9-12 October, 1985. 25. Hafez M et al. Consanguineous matings in the Egyptian population. Journal of medical genetics, 1983, 20, 58-60. 26. Roberts JA, Pembery ME. An introduction to medical genetics, 7th ed. Oxford, Oxford University Press, 1979. 27. Orioli IM, Castilla EE, Carvalho WP. Inbreeding in a South American newborn series. Acta anthropogenetica, 1982, 6(1):