RA - PheKB
advertisement

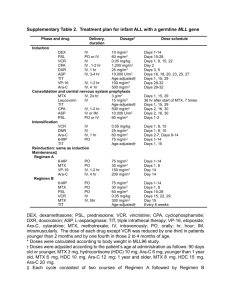
Identifying Clinical Predictors of MTX-Induced LFT abnormalities in Patients with Rheumatoid Arthritis (RA) in an EMR RA (i2b2) N=5903 No MTX N=1994 MTX (RPDR + NLP) N=4588 Normal LFTs in EMR N=4295 (?) Single elevated LFT > 2x ULN N=1130 Charts not reviewed (goal) N=650 Review random charts N=480 Review random charts N= 200 (controls) Include as Cases N=92 Exclude as Non-Cases N=388 i2b2 ALGORITHM TO IDENTIFY CASES (based on RA Prod2 Workbench query) RA defined by i2b2/Liao algorithm (RPDR + NLP at 97% specificity), N=5906 + MTX (RPDP medication code or + NLP mention) + Lab value + AST or ALT > 2x ULN (defined by different lab cutoffs at multiple labs) + MGH/BWH Rheumatologist + LMR Notes/Discharge Summaries CASE CRITERIA (based on detailed chart reviews -Cases coded as “0” and “1”) Must have a diagnosis of RA (documented in notes) Must have at least one instance of elevated liver function test (LFT): AST (SGOT) or ALT (SGPT) > 2 x the upper limit of normal (ULN) (documented in codified data) Must have evidence of concurrent MTX exposure on the same date as LFT abnormality, or up to 6 weeks after discontinuation (documented in notes) Note: Whether or not an action is taken on the part of the physician as a result of the LFT abnormality does not affect case status. However, cases are classified as “0” (MTX continued) or “1” (MTX dose decreased or discontinued) for subgroup analyses. Therefore, case = 0 and case = 1 can be combined into a single case group for NLP work, N=92 EXCLUSION CRITERIA: (Excluded subjects coded as “2”) No data: Not enough notes available around the time of the LFT abnormality to be able to confirm concurrent MTX exposure (+/- 3 months) No MTX: Patient was not taking MTX at the time of the LFT abnormality, or it had been discontinued for > 6 weeks. Error: LFT found in chart does not meet criteria for > 2X ULN (eg. error in coded data in RPDR) OR incorrect diagnosis eg. patient not diagnosed with RA (eg Crohn’s disease, Psoriatic arthritis) Arava/Leflunomide: Patients with concurrent use of MTX and Arava/Leflunomide are excluded because both medications can lead to LFT abnormalities. Prevalent: Prevalent LFT elevations prior to MTX use Comorbidity: Many of the comorbidities (listed in spreadsheet) are simply documented to assess clinical risk. The comorbidities listed below qualify as exclusions only in following clinical scenarios: Exclude if prevalent (ever diagnosed with): o Hepatitis B o Hepatitis C o Psoriasis o Psoriatic arthritis o Cirrhosis/Liver disease o Alcoholic cirrhosis o Autoimmune liver disease Exclude if concurrent hospital admission or clinic visit with an active issue listed below at the same time as the elevated LFT. Do not exclude if comorbidity if simply listed as a past medical problem. o Cardiac issues Congestive heart failure Myocardial infarction Arrhythmia (e.g. Atrial Fibrillation) o Elevated Creatinine (acute kidney injury, acute renal failure) o Lymphoma o Metastatic Cancer o Active Gallbladder disease o Pancreatitis o Inflammatory Bowel disease (eg. during a flare) o Sepsis (e.g. severe infection such as pneumonia complicated by hypotension) o Infections requiring hospitalization (eg. pneumonia, bronchitis) o Trauma (eg. s/p motor vehicle accident, s/p fall) o Surgery (invasive surgical procedure or instrumentation)