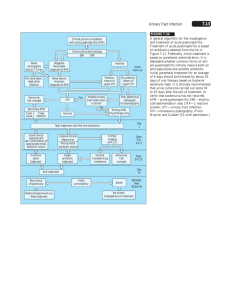
Kidney infections (Table 64
advertisement

Kidney infections: 2011-2010/ عبدالرزاق السلمان.د Aetiology Renal infections arise in the following ways. • Haematogenous infection from a primary site in the tonsils or carious teeth, or from cutaneous infections, particularly boils or a carbuncle. Renal tuberculosis occurs by blood-borne spread from lymph nodes in the neck, chest or abdomen. • Ascending infection in the urinary tract is the most common route, and it is most likely to occur when there is vesicoureteric reflux. Predisposing factors are- Urinary stasis and the presence of calculi. Bacteriology. Escherichia coli and other Gram-negative organisms are commonly responsible & Streptococcus faecalis , in which the urine is acid. while Proteus sp. and staphylococci split urea, forming ammonia which makes the urine alkaline and promotes the formation of calculi. Acute pyelonephritis Acute pyelonephritis is more common in females, especially during childhood, at puberty, soon after marriage (as a complication of ‘honeymoon cystitis’), during pregnancy and during menopause. Clinical features - Prodromal symptoms of headache, lassitude and nausea - Acute pain in the flank and hypochondrium ,often with a rigor and vomiting. - The temperature rises to 38.8 or 39.5 Co and is remitting. -The symptoms of cystitis set in soon after the onset with urgency, frequency and scalding dysuria. On examination, Tenderness in the hypochondrium and in the loin. Bacteriological examination of the urine A midstream urine , In early acute pyelonephritis there are usually a few pus cells and many bacteria. until the infection becomes established when the urine is cloudy and full of pus. 1 Culture and sensitivity testing of the causative organisms allows a rational choice of antibiotic, but parenteral treatment with a broad-spectrum antibiotic should be started before the results are available. Severe cases. There are repeated rigors and the temperature rises to 40Co or more, often without a corresponding rise in pulse rate. There is vomiting, sweating and thirst; the patient feels awful. The blood culture is usually positive, especially if the specimen has been taken during a rigor. Differential diagnosis When the symptoms and signs are typical the diagnosis is straightforward. In other circumstances it may be difficult to differentiated from 1- pneumonia, 2- acute cholecystitis. 3-acute appendicitis The urgent need is to distinguish acute pyelonephritis from appendicitis, and the site of pain and the presence of marked peritonism are usually helpful in identifying the latter. A plain abdominal radio-graph may show the outline of a swollen kidney and, if the infection is severe, a skilled ultrasonographer may be able to detect the typical appearances of pyelonephritis. Pyelonephritis of pregnancy Pyelonephritis of pregnancy usually occurs between the fourth and sixth month of gestation in women who have a past history of recurrent urinary infection. occasionally leads to abortion or premature birth. Urine infection in childhood Urine infection in childhood is important to recognise because it may endanger the function of the growing kidney. In young children, there may be few symptoms but the child passes cloudy or offensive urine, fails to thrive, fails to eat or suffers unexplained pyrexia. Pain or screaming on micturition may occur. The older child may complain of loin pain and may develop urinary frequency and nocturnal incontinence. Up to 50 per cent of children with urinary infection have an under-lying anatomical abnormality. Once the diagnosis has been confirmed by examination of a clean-catch specimen or by a specimen obtained by suprapubic needle puncture, a full urological investigation is essential. Vesicoureteric reflux of urine is detectable in about 35 per cent of children with recurrent urinary infection. 2 Once the diagnosis has been confirmed by micturating cystography, the urine should be cleared by means of an appropriate antibiotic. Treatment of acute pyelonephritis The treatment of acute pyelonephritis should be prompt, appropriate and prolonged. A full investigation to exclude underlying abnormalities in the urinary tract should be undertaken as soon as the attack is controlled. Urine for culture & sensitivity tests, Antimicrobial-an antimicrobial with a wide range of activity, such as amoxycillin or gentamicin, should be administered, parenterally if necessary Alkalinizing agents - If the urine is acid, as it is in the common coliform infections, alkalinisation of the urine by potassium citrate may help by inhibiting the growth of these organisms and relieving dysuria. Analgesia - Nonsteroidal anti-inflammatory agents -Morphine-like analgesic drug may be necessary if severe pain. The patient should be encouraged to drink copiously; if this is not possible because of nausea and vomiting, an intravenous infusion should be set up. Most urinary infections acquired outside hospital are sensitive to relatively cheap agents such as trimethoprim and amoxycillin. Hospital-acquired infections are much more likely to be resistant and more expensive second-line antibiotics may be needed. Gentamycin and carbenicillin are suitable for combating infections with more resistant strains of Pseudomonas pyocyanea, Proteus sp. and Klebsiella sp. Chronic pyelonephritis Chronic pyelonephritis is so often associated with vesico ureteric reflux that some feel that it is better named ‘reflux nephropathy’. It is an important cause of renal damage and death from end-stage renal failure. Pathology There is interstitial inflammation and scarring of the renal parenchyma with a patchy distribution. The renal tubules bear the brunt of the destruction they are atrophic and dilated. The glomeruli retain their normal structure until the final stages of the disease. Clinical features women to men 3:1. Two-thirds of affected females are under 40 years of age, whereas 60 per cent of the males are over 40. 3 Lumbar pain, dull and nonspecific in character, is present in 60 per cent of cases.Increased urinary frequency and dysuria are common. Hypertension is present in 40 per cent of cases and may be of the accelerated (‘malignant’) type. It develops slowly and is most in evidence in long-standing disease. Constitutional symptoms of lassitude, malaise, anorexia, nausea and headache Pyrexia. Attacks of low-grade fever. Anaemia. Normochromic anaemia due to unsuspected renal impairment is an occasional presenting feature. Investigations GUE/ As the glomeruli are relatively preserved, proteinuria is less marked than in glomerulonephritis (<3 g daily). Casts are not usually present but white cells are plentiful. Bacteriological examination of the urine commonly reveals the presence of E. coli, S. faecalis, Proteus sp. or Pseudomonas sp. Treatmen :Treatment may be difficult and is aimed at - eradicating predisposing contributory factors such as obstruction or stones - appropriate antibiotics, often as repeated courses of treatment. Unfortunately, once the parenchyma has been scarred it becomes vulnerable to blood-borne organisms and reinfection is likely, sometimes with a different and resistant organism. Consequently, antibiotics confer only temporary benefit and progressive renal damage is common. Surgical treatment is only indicated when the disease is confined to one kidney. This is unusual but in such cases nephrectomy or partial nephrectomy may stop the symptoms of infection and make hypertension easier to control. Some patients with end-stage renal failure require renal transplantation. 4