4×6 Oral Hypoglycemic Agents – cards
advertisement

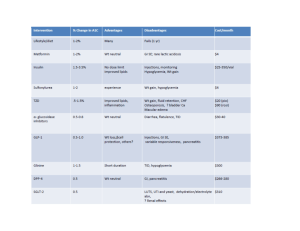
Drug Action – Target ADVERSE/se: st 1 generation Stimulates Hypoglycemia and weight gain, diarrhea, Take with sulfonylureas: secretion of constipation, dizziness, gas, anorexia, meals 100 – Chlorpropami insulin – headache, nausea, vomiting, abdominal 500 mg daily. de Pancreatic beta distress. Rare AD: resp difficulties in Adult 250mg/d (Diabinese) cells. Adjunct to cardiac and HF; sedation, muscle Ger 100-125 P = 2-4 diet & exercise to cramping, seizures; edema, comatose, Max 750mg/d D = 24-72 improve glycemic weakness, pruritus, jaundice, dark urine, control in T2DM light colored stools, increased fatigue, sore throat, increased temperature, increased bleeding or bruising. Nursing considerations: Increased risk of hypoglycemia in geriatric or malnourished patients. Take with first meal of the day. Nausea, Avoid alcohol. Long duration of action with potential for hypoglycemia avoid in older clients should not be used by women who are pregnant or nursing, or by individuals allergic to sulfa drugs; sulfonylura interacts with many other drugs. Drug Action – Target ADVERSE/se: 2nd Antidiabetic / Management of TYPE 2 APLASTIC ANEMIA PO (adult) 5 mg /day generation diabetes mellitus when diet therapy photosensitivity, (geriatric 2.5mg/day) sulfonylureas fails. Requires some pancreatic hypoglycemia observed 3-4 initially may be ↑ by 2.5 -5 glipizide function. Action: lower blood glucose hrs May increase or mg/day at weekly intervals (Glucatrol) by stimulating the release of insulin decrease appetite. Increased as needed (max 40 from the pancreas and increasing weight, dyspepsia, nausea, mg/day (immediateO = 15-30 the sensitivity to insulin at receptor constipation/diarrhea, avoid release), administered min sites. May also decrease hepatic alcohol. Possible glipizide 30 min before a P = 1-2 hr glucose production. hypoglycemia in geriatric or meal. D = 24 hr malnourished patients. Nursing considerations: Take 30 minutes before first meal of the day. Hyperglycemia w/high doses of nicotinic acid. observe for s/s of hypoglycemic reactions. Assess for allergy to sulfonamides. Patients on beta blocker therapy may have subtle signs of hypoglycemia. Lab Tests: serum glucose, glycosylated hemoglobin, May cause an in AST, LDH, BUN, and serum creatinine. CBC Report ↓ in blood counts promptly Toxicity: Overdose is manifested by s/s of hypoglycemia. Severe treated with IV D50W. High Alert: Accidental administration of oral hypoglycemic agents to non-diabetic adults and children has resulted in serious harm or death. Before administering, confirm that patient has T2DM. Drug Action – Target ADVERSE/se: Biguanides: Decrease hepatic LACTIC ACIDOSIS, nausea, PO: 500 mg once or Metformin glucose production vomiting, abdominal pain, twice daily w/increases (Glucophage) and intestinal malaise, loss of appetite q 2 weeks until glucose absorption; difficulty, may lose weight, adequate response or P = 2-3 improve insulin breathing, diarrhea, muscle max dose (2550mg) D = 12-24 sensitivity/ Target is weakness. Vit B12 deficiency Take with first main liver, small intestine, or reduced absorption and meal SLOW onset of and peripheral folic acid, anorexia, metallic action not noted for 14 tissues taste, rarely suitable for days of initial therapy adults > 80 yr of age. Nursing Implications: Take with meals to decrease GI distress. May cause anorexia. Avoid Alcohol. Avoid in renal failure because of risk of lactic acidosis. T2DM – contraindicated w/renal insufficiency or uncontrolled HF. Drug Action – Target ADVERSE/se: Thiazolidinediones Improves insulin Actos: edema, HF, headache, Once or twice (glitazones): sensitivity – target myalgia, sinusitis, upper resp daily Pioglitazone(Actos) activates genes infections. Avandia - PO 4 P= 2 involved with fat Avandia: CHF, LACTIC mg/daily or 2 D = 16-24 synthesis and ACIDOSIS, possible liver mg/twice daily. rosiglitazone(Avan carbohydrate damage, hepatotoxicity -rare. Peak in 1 hr. dia) metabolism mild anemia, fluid retention, Actos – PO 15 to P = 1 (Davis UKN) Only for T2DM who weight gain, altered lipid levels. 45 mg once daily. D = 12-24 can produce Peak 2 hrs. insulin. Nursing Implications: Take once a day without regard to food. Increased weight. monitor liver function, monitor for edema, weight gain, HF Fluids – HF requires careful monitoring. Blood testing for liver functions should be performed before start of therapy q 2 months during 1st year and periodically thereafter. Drug Meglitinides NonSulfonylureas: repaglinide (Prandin), P = 1 hr D = 4 hr neteglide (Starlix) P = 1 D= < 4hr Action – Target ADVERSE/se: Stimulates HYPOGLYCEMIA and Prandin: 0.5 – 4mg 3 times secretion of weight gain; Repaglinide daily before meals. Omit if insulin has a lightly increased risk client skips meals. Not to Targetfor cardiac events, exceed 16mg/day Pancreatic headache, resp tract Starlix: Dosed at 60 -120 mg beta cells infection, altered liver 3 times/daily immediately T2DM function tests. Cardiac before meals.pt approaching May be used effects – hypotension, chest glycemic control may be with pain, cardiac dysrhythmias. started at 60 mg 3times metformin, Starlix – back pain, flu like daily.Take with meals onset rosigliazone, symp. within 15-20 minutes RAPID pioglitazone. Nursing Implications: Take 15-30 min before meals. May increase weight, tooth disorders, nausea/vomiting. Diarrhea/constipation. Limit alcohol. May increase risk of hypoglycemia in malnutrition. Drug AlphaGlucosidase Inhibitor: acarbose (Precose) P = not absorbed D= 8 – 12 hrs. Action – Target ADVERSE/se: Delays absorption of glucose from flatulence, PO 25 mg 3xdaily. not to GI Tract / Target – Small intestine. diarrhea exceed 50 mg 3xdaily in antidiabetic/ Management of TYPE (particularly patients < 60 kg or 2 diabetes in conjunction with after high- 100 mg 3 x daily > 60 kg. dietary therapy, may be used with carb meal) Administer w/first bite of insulin or other hypoglycemic abdominal each meal agents. Lowers blood glucose by pain, may Must be taken with meals. inhibiting the enzyme alphainterfere Omit if skipped meal.50-100 glucosidase in GI tract. Delays and with iron mg 3 times daily. Initiate reduces glucose absorption absorption dose slowly to reduce GI adverse effects. Nursing Implications: observe patient for hypoglycemia – sweating, hunger, weakness, dizziness, tremor, tachycardia, anxiety. Lab Test Consider: serum glucose & glycosylated hemoglobin. Monitor AST and ALT q 3 mo for 1st year. Take with first bite of main meal. Limit alcohol. May decrease absorption of digoxin. Drug Action – Target ADVERSE/se: Glucogon Indicated for treatment HYPERSENSITI IM, IV SQ 0.5 to 1mg TO RAISE BLOOD SUGAR of severe VITY half-life 10 minutes. IM-O:10 min P: 30 hypoglycemia in REACTIONS, duration 1.5 hrs. minD:60-90/12-27min diabetes and adjunct ANAPHYLAXIS, repeated in 20 IV-O:1 min P:5 min D: for GI radiography. nausea, minutes when 9-17min Natural polypeptide vomiting, allergic necessary. SQ-O:10 min P: 30-45 min hormone secreted by reaction. no D:60-90 min pancreatic alpha cells significant drug in response to interactions. hypoglycemia. Drug Adjunctive Therapies Incretin mimetics Action – Target ADVERSE/se: Exenatide (Byetta) for patients Pramlintidide (Symlin) taking metformin, a sulfonylura, or a synthetic form of hormone combination of metformin and a amylin. (normally sulfonylura. produced by beta cells in Action: lowers blood glucose the pancrease) Works levels by increasing insulin with insulin and glucagon secretion in the presence of to maintain normal blood elevated blood glucose levels. glucose levels taken Good because it does not tend to w/meals. Improves HbA1c increase risk of hypoglycemia. levels by slowing gastric emptying rate.