INTERESTING IMAGE
advertisement

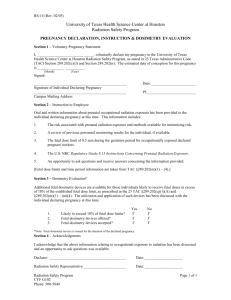
INTERESTING IMAGE Title: FDG PET/CT of a Late-term Pregnant Woman With Breast Cancer Authors: Te-Chun Hsieh, MD,*† Yu-Chin Wu, MD,‡ Shung-Shung Sun, MD,*† Lu-Yen Chu, MD,*§ Kuo-Yang Yen, BS,*† and Chia-Hung Kao, MD*¶ Abstract: A 38-year-old pregnant woman at 26-week gestation with left breast cancer requested an FDG PET/CT scan for more detailed staging of her breast cancer before treatment. After discussing the potential radiation-related risk and estimating possible absorbed dose to fetus, she consented for examination. By using a low-radiation-dose CT protocol and administration of routine 370-MBq FDG without diuresis, the resultant calculated (using existing models to predict fetal radiation exposure) fetal dose from CT and FDG would be 3.60 mGy and 6.29 mGy, respectively. In contrast to the existing few literatures, our case also demonstrated previously unreported uptake in the fetal kidneys. Key Words: breast cancer, pregnancy, fetus, FDG PET/CT, radiation exposure, kidney From the *Department of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan; †Department of Biomedical Imaging and Radiological Science, China Medical University, Taichung, Taiwan; ‡Departmentof Nuclear Medicine, National Taiwan University Hospital Hsin-Chu Branch, Hsinchu City, Taiwan; §China Medical University, Taichung, Taiwan; and ¶School of Medicine, China Medical University, Taichung, Taiwan. Y-C.W. and C-H.K. contributed equally to this work. Conflicts of interest and sources of funding: none declared. Reprints: Chia-Hung Kao, MD, Department of Nuclear Medicine and PET Center, China Medical University Hospital, No. 2, Yuh-Der Rd, Taichung 404, Taiwan. E-mail: d10040@mail.cmuh.org.tw. FIGURE 1. A 38-year-old pregnant woman at 26-week gestation with left breast cancer was demonstrated by PET/CT performed for staging (T2N0M0, stage IIA). The patient requested FDG PET/CT for her breast cancer. Because estimated fetal dose was unlikely over 50 mGy, deterministic effect of ionizing radiation would not happen with nearly negligible increases of incidence of childhood cancers.1–3 Therefore, interruption of pregnancy seemed unnecessary.4 After realizing these facts about ionizing radiation, she consented for examination. The patient received intravenous injection of 370-MBq FDG with 500-mL 0.9% saline. She was asked to void before scanning, 60 minutes after injection. Certain procedures, such as encouraging frequent voiding and use of diuretics that helped to decrease radiation burden,5 were not applied because of the concern of affecting image quality. PET/CT scanned from head to midthighs with low-radiation-dose CT protocol (0.8-second rotation time, 120 kVp, variable mA with AutomA technique, 3.75-mm slice thickness, and 1.75:1 pitch). Reconstructed images and transaxial slices were provided to demonstrate complex orientations between mother and fetus. Four representative obliquely sectioned images (C, left to right) were as follows: maximum intensity projection (MIP) of CT revealing skeleton of mother and fetus, thin-sectioned CT showing maternal breast cancer and fetus simultaneously, MIP of PET revealing FDG radioactivity in breast cancer and fetus, and fused MIP PET/CT. Consecutive transaxial slices (D) indicated FDG radioactivity in the fetal heart (white arrows) and kidneys (black arrows). Slight misregistration of PET/CT was observed, probably caused by intrauterine fetal movement. Inconspicuous fetal brain uptake (B, black arrowhead) was also noted. Nevertheless, there were also maternal breast cancer (A, white arrowhead), cold-activated brown adipose tissues in the neck, and absence of metastases. Estimated fetal dose from FDG was 6.29 mGy derived from conservative fetal dose conversion factor for 6-month gestation (1.7×10-2 mGy/MBq).6 CT dose was 3.60 mGy derived from CT dose index (CTDIvol) of uterus (3.0 mGy) and conservative conversion factor from the CTDIvol to fetal dose (1.2 mGy/mGy).7 Finally, a healthy male baby was delivered uneventfully after full-term pregnancy. Breast cancer during pregnancy is uncommon8 –13 and can cause difficulties in diagnosis and treatment with ionizing radiation and chemotherapy in consideration of fetal effect. To date, there are still debates about fetal doses from maternal FDG administration.5,6,14 Despite drawback of PET/CT increasing fetal dose from CT, simultaneous visualization of fetal anatomic and physiological details contributes to discover the previously never reported fetal renal accumulation of FDG in our case. Theoretically, such finding is expectable because fetal urine production begins between 8 and 10 weeks’ gestation.15 A threshold of 100 –200 mGy is needed to cause fetal mental retardation and organ malformations.16 Besides, stochastic effects causing cancer or germ cell mutation may increase above 50 mGy.2 Because average absorbed dose to fetus from single diagnostic study is much less than 50 mGy, fear of fetal radiation exposure should not hamper examinations’ benefit to maternal health.1,17–24 However, safety counseling is necessary before radiation exposure. Informed consent should also be obtained before examination. Nonionizing imaging procedures should always be considered in priority for pregnant patients.2 REFERENCES 1. Wieseler KM, Bhargava P, Kanal KM, et al. Imaging in pregnant patients: examination appropriateness. Radiographics. 2010;30:1215–1229; discussion 1230 –1233. 2. Williams PM, Fletcher S. Health effects of prenatal radiation exposure. Am Fam Physician. 2010;82:488–493. 3. Patel SJ, Reede DL, Katz DS, et al. Imaging the pregnant patient for nonobstetric conditions: algorithms and radiation dose considerations. Radio-graphics. 2007;27:1705–1722. 4. McCollough CH, Schueler BA, Atwell TD, et al. Radiation exposure and pregnancy: when should we be concerned? Radiographics. 2007;27:909– 917; discussion 917–918. 5. Takalkar AM, Khandelwal A, Lokitz S, et al. 18F-FDG PET in pregnancy and fetal radiation dose estimates. J Nucl Med. 2011;52:1035–1040. 6. Stabin MG. Proposed addendum to previously published fetal dose estimate tables for 18F-FDG. J Nucl Med. 2004;45:634–635. 7. Helmrot E, Pettersson H, Sandborg M, et al. Estimation of dose to the unborn child at diagnostic X-ray examinations based on data registered in RIS/PACS. Eur Radiol. 2007;17:205–209. 8. Guidroz JA, Scott-Conner CE, Weigel RJ. Management of pregnant women with breast cancer. J Surg Oncol. 2011;103:337–340. 9. Sanchez Martinez MC, Ruiz Simon A. Breast cancer during pregnancy. Breast Cancer Res Treat. 2010;123(suppl 1):55–58. 10. Navrozoglou I, Vrekoussis T, Kontostolis E, et al. Breast cancer during pregnancy: a mini-review. Eur J Surg Oncol. 2008;34:837– 843. 11. Ring AE, Smith IE, Jones A, et al. Chemotherapy for breast cancer during pregnancy: an 18-year experience from five London teaching hospitals. J Clin Oncol. 2005;23:4192– 4197. 12. Amant F, Deckers S, Van Calsteren K, et al. Breast cancer in pregnancy: recommendations of an international consensus meeting. Eur J Cancer. 2010;46:3158 –3168. 13. Loibl S, von Minckwitz G, Gwyn K, et al. Breast carcinoma during pregnancy. International recommendations from an expert meeting. Cancer. 2006;106:237–246. 14. Zanotti-Fregonara P, Jan S, Taieb D, et al. Absorbed 18F-FDG dose to the fetus during early pregnancy. J Nucl Med. 2010;51:803– 805. 15. Yiee J, Wilcox D. Abnormalities of the fetal bladder. Semin Fetal Neonatal Med. 2008;13:164 –170. 16. Kal HB, Struikmans H. Radiotherapy during pregnancy: fact and fiction. Lancet Oncol. 2005;6:328 –333. 17. Bural GG, Scheetz M, Laymon CM, et al. Tc-99m red blood cell bleeding scan in a pregnant woman presenting with hematemesis: a brief review of indications and guidelines for radionuclide scans during pregnancy. Clin Nucl Med. 2011;36:987–990. 18. Bagga S. A corpus luteal cyst masquerading as a lymph node mass on PET/CT scan in a pregnant woman with an anterior mediastinal lymphomatous mass. Clin Nucl Med. 2007;32:649–651. 19. Sood R, Story A, Rossleigh MA, et al. Superiority of F-18 FDG PET imaging for detection of a pheochromocytoma. Clin Nucl Med. 2006;31:13–15. 20. Sherigar RM, Slavin JD Jr, Hawkins HB, et al. Breast uptake of Tc-99m pertechnetate during perfusion lung scan in pregnancy. Clin Nucl Med. 1998;23:700 –701. 21. Griffith D, Alexander M, Gelman R, et al. Normal uptake in a gravid uterus on Tc-99m DTPA imaging. Clin Nucl Med. 1992;17:736 –737. 22. Baker J, Ali A, Groch MW, et al. Bone scanning in pregnant patients with breast carcinoma. Clin Nucl Med. 1987;12:519 –524. 23. Ponto JA. Fetal dosimetry from pulmonary imaging in pregnancy. Revised estimates. Clin Nucl Med. 1986;11:108 –109. 24. Marcus CS, Mason GR, Kuperus JH, et al. Pulmonary imaging in pregnancy. Maternal risk and fetal dosimetry. Clin Nucl Med. 1985;10:1– 4.