EARLY DETECTION OF DVT BY NON-INVASIVE

SIM UNIVERSITY
SCHOOL OF SCIENCE AND TECHNOLOGY
EARLY DETECTION OF DVT BY NON-
INVASIVE ARTERIAL TONOMETERY
STUDENT
SUPERVISOR
PROJECT CODE
TECHNIQUE
: KHIN SANDA (PI NO.Q0805927)
: MR CHING CHI MAN RAYMOND
: JUL2010/BME/003
A project report submitted to SIM University
In partial fulfilment of the requirements for the degree of
Bachelor of Science in Biomedical Engineering
JULY 2010
TABLE OF CONTENTS
LISTS OF FIGURES
LIST OF TABLES
ACKNOWLEDGEMENT
ABSTRACT
CHAPTER ONE
Introduction
1.1 Background
1.1.1 Artery and Vein Comparison
1.1.2 DVT Symptoms
1.1.3 Vein Physiology
1.2 Objective
1.3 Scope and Limitation
1.4 Report Layout
CHAPTER TWO
Review of Theory
2.1 Invasive Blood Pressure Method
2.2 Non-invasive arterial tonometery technique
2.3 Non-invasive Measurement of Central Vascular Pressure
2.4 Cuffless and non-invasive tonometry mean arterial measurement
2.5 Pulse Sensing
2.6 Research on Sensor Principle
2.6.1Sensitivity
2.6.2 Sensitivity Error
2.6.3 Range
2.7 Piezoelectric Sensor
2.8 Fiber Optic Sensors
2.9 Strain Gauge
2.9.1Advantages of Strain Gauge Technology
Page
14
15
17
12
12
13
13
8
9
7
7
10
11
12
6
6
4
6
2
3
1
1 i
2.9.2 How arterial tonometry technique being used in strain gauge
CHAPTER THREE
Design Fundamental and Implementation of Prototype
3.1 Strain Gauge Selection
3.1.1 Specification
3.1.2 Gauge Factor
3.2 Strain Gauge Bonding
3.3 Soldering of the Strain Gauge
3.4 Circuit Design
3.4.1 Circuit Components List
3.4.2 Wheatstone Bridge (Quarter Bridge)
3.4.3 Amplifier Circuit
3.5 Mechanical Design
3.5.1 Material Selection
3.5.2 Size Selection
3.5.3 Shaft Mounting
3.6 Overall Prototype Design
3.6.1 Elaboration on the prototype
3.7 Result
CHAPTER FOUR
Summary
4.1 Conclusion
4.2 Difficulties
4.3 Recommendation
CHAPTER FIVE
Reflections
REFERENCES
18
36
36
37
39
27
28
30
30
31
31
32
33
33
21
23
24
26
19
20
20
20
40
42
List of Figure
Figure 1 Artery and Vein
Figure 2 Artery and Vein Top view
Figure 3 DVT symptom leg compared with normal leg
Figure 4 Veins in leg
Figure 5 Deep Vein
Figure 6 Invasive blood pressure measurement
Figure 7 Illustration of pressure pulse method
Figure 8 Applanation tonometery is performed by placing a pressure sensor
Figure 9 Reflection of the pulse wave during the systolic period
Figure 10 Piezoelectric sensor
Figure 11 Fiber optic sensor
Figure 12 Strain gauge performance steps
Figure 13 A typical strain gauge
Figure 14 Full Bridge Circuit
Figure 15 A thin film strain gauge
Figure 16 Thin metal feeler gauge
Figure 17 After the bonding process
Figure 18 Complete soldering
Figure 19 Connect to the circuit
Figure 20 Circuit design
Figure 21 Circuit on testing board
Figure 22 Flow chart
Figure 23 Quarter Bridge circuit
Figure 24 Strain gauge with Quarter Bridge circuit
Figure 25 LM358N
Figure 26 Pin number LM358N
Figure 27 aluminium shaft
Figure 28 Aluminium shaft mounted with bushing
Figure 29 Overall prototype design
Figure 30 Strain gauge testing method
Figure 31 Height Vs Vout
Figure 32 First proposed design
Figure 33 Unsuitable pump
Page
2
3
4
5
5
7
9
10
10
31
31
32
33
27
27
28
29
34
38
39
24
25
25
26
20
22
23
23
14
14
15
16
17
List of Table
Table 1Comparison between Artery and Vein
Table 2 Result data
2
34
Acknowledgement
I wish to express my sincere gratitude to my project supervisor, Mr. Ching Chi Man
Raymond who rendered guidance and encouragement during the period of my project work.
Special thanks also to my family and friends for their manual support and love, care and understanding.
Abstract
Deep vein thrombosis (DVT) is the formation of blood clot that forms in the deep veins in the body, this blood clot is also known as thrombus. This normally occurs in the lower part of the body, either in the lower leg or thigh. The formation of the thrombus may interfere with the blood circulation and may even break off and travel through the bloodstream and lodge in other parts of the body causing damage to the organ and eventually leading to death.
It is difficult for DVT patients to detect this problem early as there are no major symptoms for early stages of DVT. Early detection of DVT requires an accurate and sensitive sensor system which applies non-invasive arterial tonometery technique. The pressure exerting on the vessel wall can be determined whether a person has DVT. The arterial pressure will be reduced even more for DVT patients than healthy subjects
Strain gauge is designed to convert mechanical motion into an electrical signal whereby a change in resistance is proportional to the strain experienced by the sensor. The strain gauge is connected into a Wheatstone Bridge circuit with a combination of a single gauge Quarter
Bridge. In this project, the technique of this measurement is such that when pressure is exerted on the vessel wall, the bending of the vessel can trigger the voltage changes of strain gauge through the aluminium shaft which represents the contact stress sensor.
Strain gauge is bonded on the feeler gauge and tested with aluminium shaft to measure the sensitivity. With the application of this technique, the result voltage varied linearly with respect to the feeler gague height between 0.1mm to 0.2mm. This measurement illustrates the concept of pressure differences applied on the vessel wall that was detected non-invasively. i
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Chapter 1
Introduction
Deep vein thrombosis (DVT) occurs when blood clot forms in one of the large veins, usually occurring in the arm or more commonly in the leg leading to partially or completely blocked circulation. DVT blood clot has the potential to move in to the lungs creating a life threatening condition known as pulmonary embolism. It is estimated that in United States, venous thrombosis and pulmonary embolism are associated with 2 million Americans every year and up to 600,000 will develop pulmonary embolism. Each year, 60,000 Americans die from pulmonary embolism.
It is also a known fact that venous thrombosis and pulmonary embolism are often silent and among the most difficult to detect by clinical examinations. This is why early detection of
DVT is a very important aspect. An example of an early detection of DVT is using a noninvasive arterial tonometery technique, which will be introduced in this report.
1.1
Background
Deep Vein Thrombosis or more commonly known as DVT is basically a blood clot that occurs in a vein deep in the body, more prominently occurring in the lower leg or thigh.
There are many reasons why blood can form in the veins. These include prolonged immobility (after surgery), long airplane ride, trauma or fractures of the legs, injury to the veins, congestive heart failure, people who are very overweight and inherited blood disorder
.
[18]
Blood clots can occur in any arteries or veins, but only blood clots in deeper veins are of medical significance. We have to look into why blood clot occurs in veins is more critical compared to arteries.
KHIN SANDA Q0805927 Page 1
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
1.1.1 Artery and Vein Comparison
First of all, the comparison between arteries and veins are looked into.
ARTERY
Carry blood away from the heart
VEIN
Carry blood towards the heart
Blood is under great pressure in arteries, it flows fast and reflecting the rhythmic pumping action of the heart
Have thick and elastic muscular walls
Blood is not under great pressure in veins hence it flows more slowly and smoothly
Have no valves
Have relatively thin, slightly muscular walls
Have semi-lunar valves along their lengths to prevent back flow of blood
Carry red oxygenated blood Carry bluish-red deoxygenated blood
Table 3Comparison between Artery and Vein
KHIN SANDA Q0805927
Figure 8 Artery and Vein
Page 2
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 9 Artery and Vein Top view
1.1.2 DVT Symptoms
The symptom of the deep vein thrombosis depends on where the blood clot has formed. In most cases, it is the legs, especially the calf area. Some of the common symptoms are heaviness of the leg, tenderness in the calf area, swelling in the calf area, warmth near the calf. [18] However, at least 30% will not have any symptoms in early stage. [19] The blood flow decreases not only because a blood clot is blocking the blood flow, but the blockage damages the walls of the lung's blood vessels (pulmonary arteries). The damage releases chemicals that cause multiple blood vessels clamp down. As shown in Figure 3 there is inflammation and swelling below the blockage site.
KHIN SANDA Q0805927 Page 3
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 10 DVT symptom leg compared with normal leg
1.1.3 Vein Physiology
Naturally Veins are smaller than arteries. The mean diameter of vein is 1.8mm (range, 0.6 to
3.2mm). As mentioned in above table blood pressure in the veins are as low as 2mmHg to 5 mmHg. On the other hand, the blood pressure in arteries is 80mmHg to 100mmHg. The pressure in the veins and arteries represent the force applied to the side of the vessel wall indicating hydrostatic pressure. The majority of blood clots in the veins occur in the leg.
When clots occur in veins they have a tendency to break off and travel in the bloodstream, which is known as pulmonary embolism.
[18]
The clot which is known as an embolus travels to the lungs via the heart and causes shortness of breath and sharp pain the chest area.
Pulmonary embolism is a very serious condition, this is due to the fact that it causes damage to the lungs, other body organs and may even cause dearth if left untreated. Thus, if we can detect early clot in the vein it might be a life saving for some of the DVT patients.
A vein can range in size from 1 millimeter to 1-1.5 centimeters in diameter. The smallest veins in the body are called venules. There are two types of veins in the leg; superficial veins and deep veins. Superficial veins lie just below the skin and are easily seen on the surface.
Deep veins, as their name implies, are located deep within the muscles of the leg.
[20]
Blood
KHIN SANDA Q0805927 Page 4
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE flows from the superficial veins into the deep venous system through small perforator veins.
Superficial and perforator veins have one-way valves within them that allow blood to flow only in the direction of the heart when the veins are squeezed.
[20]
When it comes to the veins, only blood clots in the deeper veins are of medical significance.
Figure 11 Veins in leg
KHIN SANDA Q0805927
Figure 12 Deep Vein
Page 5
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
1.2
Objective
The objective of this project is to detect DVT at early stage with non-invasive arterial tonometery technique. The pressure pulse method is a non-invasive way to measure the pressure exerted on the vessel wall. The pressure in veins and arteries will slow down due to the clot occurs in deep veins. By detecting the low pressure in the veins or arteries at early stage can eliminate or cure DVT efficiently for DVT patients. Thus, to research the effect of DVT or pathogenesis of DVT to understand the formation of blood clot, to develop a concept to proof by building a prototype and analysis of data collected from prototype.
1.3
Scope and Limitation
In this project, the prototype which illustrates the concept of contact stress sensor was successfully built and the test result also agrees with theory and the related experiment result.
The strain gauge, mechanical pressure sensor is used to build the prototype. The strain gauge is connected to a Wheatstone Bridge (Quarter Bridge) circuit. As stress is applied to the bonded strain gauge, resistive changes take place and unbalance the Wheatstone Bridge.
Changes in resistance result the changes in voltage when the vessel bend during the measurement.
The prototype illustrates the contact stress sensing as it non-invasively detect DVT in the veins. However, the prototype is not applicable for calibration or back to zero method before another measurement. It is not clinically tested or a finish product as this is a conceptual prototype to demonstrate the concept.
1.4
Report Layout
The capstone project report is divided into 5 chapters. Chapter 1 is the introduction of the overall report which includes background, objective, scope and limitation, report layout.
Chapter 2 is the review of theory for better and deeper understanding. Chapter 3 is the design fundamental and implementation of the prototype. Chapter 4 is finally summary, conclusion and recommendation for future work. Chapter 5 is reflection on how to cope up with this project to get the basic concept in order to meet the objective.
KHIN SANDA Q0805927 Page 6
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Chapter 2
Review of Theory
The following topics were reviewed to enable a better understanding of background theories and facilitate in building the project.
Invasive arterial blood pressure measurement
Non-invasive arterial tonometery technique
Noninvasive Measurement of Central Vascular Pressures with Arterial Tonometry
Cuffless and non-invasive tonometery mean arterial pressure measurement
Pulse sensing
Research on sensors principle
Piezoresistive
Fiber optics
Strain gauge
2.1 Invasive blood pressure method
This technique involves direct measurement of arterial pressure by placing a cannula needle in an artery (usually radial, femoral, dorsalis pedis or brachial).
[1]
The cannula must be connected to a sterile, fluid-filled system, which is connected to an electronic patient monitor. The advantage of this system is that pressure is constantly monitored beat-by-beat, and a waveform (a graph of pressure against time) can be displayed .
KHIN SANDA Q0805927
Figure 13 Invasive blood pressure measurement
Page 7
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Patients with invasive arterial monitoring require very close supervision, as there is a danger of severe bleeding if the line becomes disconnected.
[1]
It is generally reserved for critically ill patients where rapid variations in blood pressure are anticipated.
There are a variety of monitors with invasive blood pressure monitoring for Trauma, critical care and operating room applications. These include single pressure, dual pressure, and multi-parameter (i.e. Pressure / temperature)
Invasive Blood Pressure monitors are pressure monitoring systems designed to acquire pressure information for display and processing. This can be used to monitor arterial, central venous, pulmonary arterial, left atrial, right atrial, femoral arterial, umbilical venous, umbilical arterial and intracranial pressures.
Blood pressure parameters are derived in the monitor's microcomputer system. Usually, systolic, diastolic and mean pressures are displayed simultaneously for pulsatile waveforms
(i.e. arterial and pulmonary arterial).
2.2 Non-invasive arterial tonometery technique
Arterial tonometery is a pressure pulse method that can non-invasively record calibrated pressure in superficial arteries with sufficient bony support, such as the radial artery.
A tonometery is applied by first centering a contact stress over the vessel. This is accomplishing by repositioning the device until the largest is pulse is detected. An array of sensors has been used to accomplish this electronically.
[7]
Then, the tonometery is depressed towards the vessel leads to applanation of the vessel wall. If the vessel is not flattened sufficiently, the tonometery measures forces due to arterial wall tension and bending of the vessel. As depression continues arterial wall is applanated further, but not so much as to occlude blood flow. [7] At this intermediate position wall tension becomes parallel to the tonometery sensing surface. Arterial pressure is then the remaining stress perpendicular to the surface and is measured by the sensor. This is termed the contact stress due to pressure.
Ideally, the sensor should not measure skin shear (frictional) stresses. The contact stress is equal in magnitude to the arterial pressure when these conditions are achieved. In addition,
KHIN SANDA Q0805927 Page 8
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE tonometery require that the contact stress sensor be flat, stiffer than the tissues, small relative to the vessel diameter calibration can be attained either by monitoring the contact stress distribution the maximum in measured pulse amplitude.
Figure 14 Illustration of pressure pulse method
2.3 Noninvasive Measurement of Central Vascular Pressures with Arterial
Tonometry
The arterial pulse has historically been an essential source of information in the clinical assessment of health. Only the peak and trough of the peripheral arterial pulse waveform are clinically used with current sphygmomanometric and oscillometric devices.
[22]
There are few limitations exist with peripheral blood pressure. Central aortic pressure is a better predictor of cardiovascular outcome than peripheral pressure. Peripherally obtained blood pressure does not accurately reflect central pressure due to pressure amplification.
Antihypertensive medications have differing effects on central pressures despite similar reductions in brachial blood pressure. Applanation tonometry can overcome the limitations of peripheral pressure by determining the shape of the aortic waveform from the radial artery.
[22]
Waveform analysis not only indicates central systolic and diastolic pressure but also determines the influence of pulse wave reflection on the central pressure waveform.
Radial artery applanation tonometry is a noninvasive, reproducible, and affordable technology that can be used in conjunction with peripherally obtained blood pressure to guide patient management. See Figure 8 for applanation tonometry performance.
KHIN SANDA Q0805927 Page 9
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 8 Applanation tonometry is performed by placing a pressure sensor over the radial artery
Figure 9 Reflection of the pulse wave during the systolic period
2.4 Cuffless and non-invasive tonometery mean arterial pressure measurement
In this study there is a new development of a cuffless and non-invasive measurement technique of blood pressure using tonometric pressure sensor. The maximum value of a pulse
KHIN SANDA Q0805927 Page 10
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE pressure is not obtained at mean arterial pressure (MAP).
[23]
MAP was figured out based on the physiological characteristic including the elasticity of wrist tissue, the depth of blood vessel. Through an analysis of 198 clinic data, have induced the regression equation of the
MAP.
The probability of the elasticity, depth and AP (M) to explain MAP was 92.1%.
[23]
The mean difference and the standard deviation between the MAP predicted from the regression equation and the MAP measured by commercial cuff type BP meter were Z-3.183 mmHg and 5.133 mmHg respectively. Comparing the results with the American national standard for electronic or automated sphygmomanometers, come to the conclusion that the results are reliable and accurate. Detecting only one part of the body and using only one device are very advantageous over other BP measurement technique.
2.5 Pulse Sensing
Pulse sensors attempt to measure the arterial pulse waveform from either the arterial wall deflection or force at the surface of the skin above a palpable.
[6]
Typically, these sensors are not directly calibrated in terms of pressure, but ideally respond proportionately to pressure.
Pulse Sensor System uses a conformable pressure sensor array to capture pulse waveform data. The sensor is uniquely designed for maximum durability and sensitivity which allows the user to feel the pulse through the active area.
[6]
This type of sensor measures stress due to arterial pressure transmitted through the skin above the pulse artery. The pressure pulse sensor requires surface deflections to be zero, as opposed to the volume sensor. Thus, the contact forces are proportionate to arterial pressure at the skin surface. Pressure pulse method was found to provide superior waveform accuracy, free of the effects of vascular nonlinear viscoelasticity.
Alternatively, the stiffness of the sensor can best characterize its pulse accuracy. High stiffness relative to the artery and surrounding tissue is required to best approximate the pressure pulse method. Arterial pulse recording is performed while the subject is stationary and refrains from moving the pulse location. But, it has become of interest to acquire ambulatory records. Without restraint, pulse recording is quite difficult due to motion artefact. For example, hand or finger motion can appear in recordings of the radial artery. A change in sensor positioning or acceleration can result in other types of artefact. The artefacts
KHIN SANDA Q0805927 Page 11
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE are often comparable in magnitude and frequency to the pulse, rendering simple filtering methods useless. Recently though, artefact cancellation techniques that employ sensor arrays have been applied with good success.
2.6 Research on sensor principle
A sensor is a device which receives and responds to a signal. Sensors need to be designed to have a small effect on what is measured; making the sensor smaller often improves this and may introduce other advantages. Sensors, like other areas of technology that must be understood before they can be properly applied. Some of the most common terms are considered into research for better understanding on sensor principle.
2.6.1 Sensitivity
The sensitivity of the sensor is defined as the slope of the output characteristic cure or, in general, the minimum input of physical parameter that will create a detectable output range.
In some sensors, the sensitivity is defined as the input parameter change required to produce a standardize output change.
[5]
In other words, it is defined as an output voltage change for a given change in input parameter. For example to explain further, a typical blood pressure transducer may have a sensitivity rating of 10µ V/V/mmHg; that is, there will be a 10- µV output voltage for each volt of excitation potential and each millimeter of mercury of applied pressure. In summary, A sensor's sensitivity indicates how much the sensor's output changes when the measured quantity changes or physical parameter changes.
2.6.2 Sensitivity error
The sensitivity may in practice differ from the value specified. This is called a sensitivity error, but the sensor is still linear.
[5]
In other words, the sensitivity error is a departure from the ideal slope of the characteristic curve. For example, the pressure transducer discussed above may have an actual sensitivity of 7.8 µV/V/mmHg instead of 10 µV/V/mmHg.
KHIN SANDA Q0805927 Page 12
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
2.6.3 Range
The range of the sensor is the maximum and minimum values of applied parameter that can be measured. For example, a given pressure sensor may have a range of -400 to +400 mmHg.
Alternatively, the positive and negative ranges often are unequal. Another example is a certain blood pressure transducer is specified to have a minimum (vacuum) limit of
+450mmHg. [5] This specification is common, incidentally, and is one reason doctors and nurses sometimes destroy blood pressure sensors when attempting to draw blood through arterial line without being mindful of the position of the fluid stopcocks in the system. A small syringe can exert a tremendous vacuum on a closed system.
2.7 Piezoelectric sensor
Piezoelectric sensors are used to sense movement or vibrations in many applications. A piezoelectric sensor comprises a piezoelectric crystal which is typically mechanically coupled to an object which produces a mechanical movement.
[5]
In piezoelectric materials, an applied electric field results in elongations or contractions of the material. Moreover, piezoelectric sensors for converting slight vibrations and stress of objects under measurement into electric signals with the piezoelectric effect of their materials find applications in various fields.
[10]
Piezoelectric sensors are used as transducers because potential difference is generated when the sensor is subject to a pressure change. A detection system is electrically coupled to the piezoelectric sensor and senses, for example that a vehicle has passed over the sensor. The single disadvantage of piezoelectric sensors is that they cannot be used for static measurement. Piezoelectric sensors can only be used for very fast applications. Refer to
Figure 10 for one of the piezoelectric sensors example.
KHIN SANDA Q0805927 Page 13
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 10 Piezoelectric sensor
2.8 Fiber Optic Sensors
Fiber optics for sensing applications are used to communicate with a sensor device or use the fibers as the sensor itself to conduct continuous monitoring of physical, chemical, and biological changes in the subject or object of study. In fiber optics sensors, information is primarily conveyed in all optical sensors by a change in either phase, polarization, frequency, intensity or a combination.
[12]
There are various types of fiber optic sensors as shown in
Figure 10.
KHIN SANDA Q0805927
Figure 11 Fiber optic sensors
Page 14
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
2.9 Strain gauge
A strain gauge is a device used to measure the strain of an object. Most strain gauges are smaller than a postage stamp.
[13]
The most common type of strain gauge consists of an insulating flexible backing which supports a metallic foil pattern. The gauge is attached to the object by a suitable adhesive, such as cyanoacrylate. As the object is deformed, the foil is deformed, causing its electrical resistance to change. This resistance change, usually measured using a Wheatstone bridge.
The ideal strain gauge would change resistance only due to the deformations of the surface to which the sensor is attached.
[13]
However, in real applications, temperature, material properties, the adhesive that bonds the gauge to the surface, and the stability of the metal all affect the detected resistance. Figure 12 shows the strain gauge performance steps.
Figure 12 Strain gauge performance steps
KHIN SANDA Q0805927 Page 15
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
The strain gauge has been utilized for many years and is the fundamental sensing element for many types of sensors, including pressure sensors, load cells, torque sensors, position sensors. Basically, all strain gauges are designed to convert mechanical motion into an electronic signal. A change in capacitance, inductance, or resistance is proportional to the strain experienced by the sensor. [13] The majority of strain gauges are foil types, available in a wide choice of shapes and sized to suit a variety of applications. A strain gauge consists of a pattern of resistive foil which is mounted on a backing material. In other words, a strain gauge operates on the principle that as the foil is subjected to stress, the resistance of the foil changes in a defined way.
Figure 13 A typical strain gauge
The strain gauge is connected into a Wheatstone bridge circuit with a combination of four active gauges (full bridge), two gauges (half bridge), or a single gauge (quarter bridge). The
Wheatstone bridge is an instrument used to measure electrical resistance by means of balancing a bridge circuit. Wheatstone bridge designs and selections are based on the application requirement. When stress is applied to the bonded strain gauge, a resistive change takes place and unbalances the Wheatstone bridge. The signal output is related to the stress value. As the signal output is too small to notice, require amplifier circuit to provide a suitable level of the signal output. The amplifier circuit is also based on the individual design or calculation. Figure 14 illustrates the Full Bridge Circuit.
KHIN SANDA Q0805927 Page 16
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 14 Full Bridge Circuit
2.9.1 Advantages of strain gauge technology
In today’s market, competitive medical device manufactures and engineering personnel are coming out with custom strain gauge sensing technologies into finished products. [14] This is to achieve the competitive business advantage. The accuracy, capability and extended service life of such technologies are proven with this strain gauge application. Strain gauge application medical devices increase overall performance and improved equipment diagnostics capabilities. Custom strain gauge technology is used in both critical and noncritical medical applications. The range is from high-precision robotic surgery and mammography system positioning to patient scale weight distribution and flow measurement. In addition, Noninvasive medical imaging and diagnostic equipment (CT
Scan), Mammography system, Medical Infusion Pumps, Applantion Tonometer used strain gauge technology.
In summary, the strain gauge offers high accuracy and repeatability for seamless integration into a variety of noninvasive and minimally invasive device designs. In terms of cost perspective, typically, strain gauge is better cost effective sensors compare to other sensors such as fiber optic sensor.
KHIN SANDA Q0805927 Page 17
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
2.9.2 How Arterial tonometry technique being used in strain gauge
Strain Gauge application is very sensitive to the object which being measured. As mentioned above in medical field strain gauge applications are widely used. Arterial tonometry technique is a contact stress sensing method as centering the contact stress over the vessel.
As mentioned in Section 2.2 Non-invasive arterial tonometery technique repositioning the device until the largest is pulse is detected. Then, the tonometery is depressed towards the vessel leads to applanation of the vessel wall. The assumption on strain gauge application will work if the strain gauge senses the movement of the contact stress sensor when it trigger, the respective output will be display as current reading of measurement object. This application is based on the idea of blood pressure in the vessel can be detected by how much pressure exerted on the vessel wall. The vessel wall diameter changes can be trigger with contact stress sensor. Then the contact stress sensor movement will trigger the strain gauge which will be sensitive by the movement and voltage output will be measured through strain gauge Wheatstone Bridge circuit. Based on the changes on the vessel wall diameters strain gauge output voltage will vary accordingly. The assumption is taking to the consideration that low pressure will contract the vessel wall with smaller diameter while high blood pressure cause the vessel wall to expand. Based on this assumption, the contact stress sensor will generate the simulated force to trigger strain gauge resistance unbalance which will eventually result as voltage differences.
KHIN SANDA Q0805927 Page 18
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Chapter 3
Design Fundamental and Implementation of Prototype
Among all the researches and theory (as review in chapter 2), come to the point that strain gauge thin film is the correct application to detect the low pressure changes in the vein due to its high sensitivity. Moreover strain gauge thin film technology enables accurate, stable, reliable and low cost sensors to be produced for fluid pressure measurement applications.
The strain gauge measures 1/10,000 micro strain, which can detect a 1-dB vibration across a
10-foot room. Thus, the measurement possibilities for various strain gauges, quite literally, have an infinite range. Using Strain Gauge result, together with advanced mirco processor will provide the most accurate, reliability and repeatability tonomerty result for the user.
To prove this further there is a need in prototype design analysis and measurement result. In this chapter design fundamental includes bonding of the strain gauge, amplifier circuit, and overall design.
Below are the lists to complete the overall prototype:
Strain gauge selection
Strain gauge bonding
Soldering of strain gauge
Circuit design
Mechanical design of prototype
Overall prototype design
KHIN SANDA Q0805927 Page 19
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
3.1 Strain Gauge Selection
Foil type strain gauge value of 120Ω selected for this application. It is applicable for both static and dynamic measurement. This is a thin film foil gauge and widely use in most of the applications due to its sensitivity and precision. A typical foil gauge consists of a foil made from a resistance alloy, such as (copper, aluminium) constantan bonded to an epoxy backing film. Moreover, both surfaces being completely laminated, the gauge grids are entirely protected. A thin film strain gauge is shown in Figure 15.
3.1.1 Specification
Gauge Factor
Gauge Length
Gauge Resistance
Measureable Strain
Operating Temperature Range
Width
2
2mm
120 Ω
3
4%
-30
180 °C
1.6(Gauge); 2.5(Base)mm
Figure 15 A thin film strain gauge
3.1.2 Gauge Factor
As mentioned in 3.1.1 specification section Gauge factor is 2. In this section further more explanation on gauge factor will be discussed to understanding more on strain gauge selection. Gauge factor is defined as the fractional change in resistance to the fractional change in length along the axis of a strain gauge. It is dimensionless quantity which applies to the changes in the strain gauge as a whole. Foil type gauge factor are close to 2.0. Other
KHIN SANDA Q0805927 Page 20
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE type of strain gauge factor can be significantly larger or even negative. The equation for gauge factor is:
Gf= (delta R/R)/(delta L/L) or delta R = R x Gf x strain
This implies that when micro strain is applied to a gauge with R=120 Ω and Gf=2.0, resistance will be changed by 0.0024 Ω.
Generally provided by the strain gauge manufacturer, the gauge factor (Gf) specification is valid only for a specific excitation voltage and ambient temperature. As a result, Gf cannot always be used directly to calibrate a measurement. A sensitivity factor is sometimes specified. The sensitivity factor equals the gauge factor multiplied by a correction based on current measurement conditions. If the current conditions are the same as those under which the gauge factor was specified, the sensitivity factor and the gauge factor are identical.
3.2 Strain Gauge Bonding
Strain gauge bonding is required in order to complete the strain gauge measurement. Feeler gauge is used for the strain gauge bonding in this application. Feeler Gauge is a precision plate widely used in industries to measure the thickness. It is made of stainless steel material with known thickness and its surface is even throughout the length. Thus, it is the most suitable mounting plate for this experiment. In addition, the other side of the Feeler gauge sits on the acrylic plastic material.
First of all, feeler gauge must be cleaned, cleared from all paint and rust. The area should not be degreased. To have a clean and clear surface of feeler gauge wet tissue is used, cleaning chemical detergent (IPA). Extra care must be taken not to touch with fingers to the surface area of feeler gauge. After drying of IPA, cover the feeler gauge with transparent insulated tape in order to prevent any electrical short between feeler gauge and strain gauge legs. See figure 16.
KHIN SANDA Q0805927 Page 21
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 16 Thin metal feeler gauge
The strain gauge should be installed flat on the feeler gauge. Below are the steps of bonding the strain gauge for this application:
Remove strain gauge from the package with extra care as it is a small and thing foil type strain gauge.
Used the tags to hold the strain gauge.
Applied an even, thin layer adhesive.
Hold the strain gauge with extra care and stick on the feeler gauge to make sure to get the desired position.
Applied thumb pressure for one minute, followed by few minutes waited before removing the tape and the tags.
Removed the tape by slowly and very carefully pulling it back over itself starting at the end furthermost from the tags.
Bond strength increased after 10 minutes.
Refer figure 17 for after bonding process of strain gauge and feeler gauge.
KHIN SANDA Q0805927 Page 22
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 17 After the bonding process
3.3 Soldering of the strain gauge
Strain gauge is fitted with short leads and it is a standard practice to wire these self adhesive terminal places adjacent to the gauge. This is a bridge completion point and a change-over point to the heavier wire require for the measurement and circuit configuration. The lead out wires from the gauge are very fragile, should be handled with care while soldering. It is important not to apply the high temperature and longer timing during soldering as the gauge wires are very tiny. See Figure 18. The yellow color wire is from the circuit.
KHIN SANDA Q0805927
Figure 18 Complete soldering
Page 23
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 19 Connect to the circuit
3.4 Circuit design
The circuit design is the combination of Wheatstone Bridge (Quarter Bridge) and sensor amplifier. Figure 20 is the circuit design combination of Wheatstone Bridge and Amplifier circuit.
KHIN SANDA Q0805927 Page 24
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 20 Circuit design
KHIN SANDA Q0805927
Figure 21 Circuit on testing board
Page 25
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 22 Flow chart
The flow chart in figure 22 provides the overall prototype working mechanism. There will be detail discussions in following sections.
3.4.1 Circuit Components List
Resistor (120 Ω) x 5
Resistor (1 k Ω) x 3
Resistor (470 Ω) x 2
Resistor (47 k Ω) x 1
Resistor (10 k Ω) x 1
Op-Amp LM358N IC x 1
9V Battery x 1
KHIN SANDA Q0805927 Page 26
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Breadboard x 1
Multi Meter x 1
3.4.2 Wheatstone Bridge (Quarter Bridge)
In quarter bridge diagram, typically, the rheostat arm of the bridge (R2 in the diagram) is set to a value equal to the strain gauge resistance with no force applied. The two ration arms of the bridge (R1 & R3) are set equal to each other. With no force applied to the strain gauge, the bridge will be symmetrically balance and the voltmeter will indicate zero volts which represent zero force applied to strain gauge. As the strain gauge is either compressed or tensed, its resistance will indicate decrease or increase respectively, thus unbalancing the bridge and producing the changes in the volt meter.
Figure 23 Quarter Bridge circuit
Figure 24 Strain gauge with Quarter Bridge circuit
To increase the ease of the experiment, same resistance of three resistors were chosen. Strain gauge resistance value 120 Ω connects to the Wheatstone Bridge (Quarter Bridge). The
KHIN SANDA Q0805927 Page 27
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE bridge connection is operated by 9V DC (+9V, 0V) Battery. Additional 1 K Ω resistor is connected as pull up resistor before the bridge in order to prevent any current surge.
3.4.3 Amplifier Circuit
As mentioned in section 3.2 strain gauge bonding, changes in work piece (feeler gauge) will cause the unbalancing of the Wheatstone bridge condition. This will result in producing a very small voltage changes. Typically, this change is very small in terms of micro-volts and is unable to produce the desired level of voltage to differentiate the various resolutions. Thus, amplifier circuit is required in order to amplify the output to desired level which can be useful for data collection.
As shown in circuit diagram figure 18, the output is being amplified by using Op-amp model
LM 358N. It is a Low Power Operation Amplifier and consists of two independent, high gain, internally frequency operated operational amplifier which were designed specifically to operate from a single power supply over a wide range of voltages. Operation from split amplifier is also possible and the low power supply current drain is independent of the magnitude of the power supply voltage. See figure 25 for LM358N operational amplifier.
KHIN SANDA Q0805927
Figure 25 LM358N
Page 28
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 26 Pin number LM358N
First, the output will be connected to the inputs of the 1 st
Op-amp of LM358N which is pin 2 and pin 3. Refer figure 26 for pin numbers. Assuming the changes from output voltage is 5 micron-volts. Increased the voltage gain to 392 by choosing the feedback resistor Rf = 47 k
Ω and Rin+, Rin- = 120 Ω. Calculation of output voltage is:
Vout = Vin * ((Rf/Rin) + 1),
Vout = 2mV,
Where Vin = V1 – V2 = 5 µ V,
Rf = 47 k Ω,
Rin = 120 Ω
The output of 1 st
Op-amp is able to amplify up to changes of 2 mV.
Second, the output is re-amplified again to provide more visible changes. Although the higher gain will result in higher voltage changes, there are extra calculations and testing needed to be done in order not to reach to the saturated state of the amplifier. Once the amplifier reaches to the saturated state, the result will be always shown as ~ 9V and jeopardize the whole experiment. Thus, the gain of 10 is chosen to amplify in 2 nd Op-amp.
KHIN SANDA Q0805927 Page 29
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
The output, pin 1 of 1 st
Op-amp is connected to non-inverting input of 2 nd
Op-Amp pin 6 through 1 k Ω resistor. As the chosen gain is ~10 times, 10 k Ω resistor is used as feedback resistor for preventing from reaching to the saturated state. In other words, the difference between inverting & non-inverting voltage can’t be too large. Hence, the voltage divider rule is applied to get the inverting input voltage. Inverting input Pin 5 of 2 nd Op-Amp is connected to 2 x 470 Ω by voltage divider rule.
The output voltage value of 2 nd Op-amp is calculated by:
Vout = Vin * ((Rf/Rin) + 1),
Vout = 20mV,
Where Vin = 2mV,
Rf = 10 k Ω,
Rin = 1 k Ω
The output change of 20mV is visible and measurable result for the data collection.
3.5 Mechanical Design
3.5.1 Material Selection
The shaft requires for demonstration of contact stress sensing method which is the key portion of this project. As stated in section 2.2 Non-invasive arterial tonometery technique, the contact stress sensor must be stiffer than tissue to achieve the low pressure detection in the arteries or veins. Thus, the shaft must be stiffer than the testing object. Moreover, the shaft must be light weight enough to push the feeler gauge which is bonded with strain gauge. The material selection for the shaft is important to achieve desire testing experiment.
Aluminium is used for the shaft material which is light weight, stiffer than testing object.
KHIN SANDA Q0805927 Page 30
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
3.5.2 Size Selection
The length of the shaft must not be too long to protect too much variation. After the few experiment the length finalized at 4 cm. The diameter of the shaft must be smaller than vein or the testing object which act as vein. As stated in section 1.1 backgrounds vein diameters range from 1 mm to 1-1.5 cm. According to research deep vein are larger than 1mm. Thus, the diameter chosen as 1mm. Filing of the shaft tip has been done to achieve 1mm diameter.
Figure 27 shows 4 cm aluminium shaft.
Figure 27 aluminium shaft
3.5.3 Shaft Mounting
The shaft mounting is another important factor for this project. Acrylic plastic material is used for the mounting. The Smooth and good movement is required to have the shaft to move evenly. First, two mountings was used for the shaft movement. There were some jerking movement were encountered during the testing. Hence, one shaft mounting is used for final design. Bushing was added with mounting in order to achieve the desired movement. See figure 28. The shaft is mounted with bushing.
KHIN SANDA Q0805927
Figure 28 Aluminium shaft mounted with bushing
Page 31
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
3.6 Overall Prototype Design
The overall prototype design is shown in figure 29. It includes Amplifier circuit, Strain
Gauge which is mounted on the feeler gauge, the feeler gauge which sit on the acrylic plastic material mounting, an aluminum shaft which sits on the acrylic plastic mounting with bushing.
Feeler Gauge
9V amplifier
Circuit
Strain gauge
Aluminium shaft
Figure 29 Overall prototype design
Below is the working principle for overall prototype:
First, trigger the shaft to touch the feeler gauge.
The strain gauge is bonded on the feeler gauge.
The feeler gauge deflection or the strain gauge movement will trigger very small in resistance change in Wheatstone Bridge circuit which voltage is too small to notice as well.
The output voltage from Wheatstone Bridge is amplified by amplifier circuit.
Finally, strain gauge output is significant for data collection which will discuss more in section 3.7 Result.
KHIN SANDA Q0805927 Page 32
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
3.6.1 Elaboration on the prototype Vs actual blood pressure measurement mechanism
The shaft acts as contact stress sensor which uses to measure the vessel wall diameters. First, place the contact stress sensor on the vessel. Low blood pressure causes the contraction of blood vessel which develop lesser force to move the contact stress sensor. On the other hand, high blood pressure causes opposite effects on vessel wall diameters which causes higher forces detection on the contact stress sensor. Either force causes the disposition of contact stress senor which triggers to have in-contact with the strain gauge bonded feeler gauge.
Afterwards, the strain gauge resistance unbalance will generate the voltage output which is measured by the volt meter.
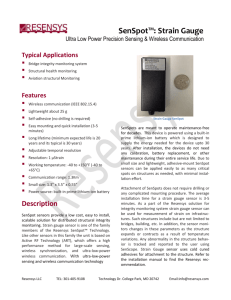
3.7 Result
Testing and measurement of strain gauge has been done before finalizing the prototype.
Figure 30 explains strain gauge testing and calculation method used in this application.
To calculate θ = tan -1 O/A
Figure 30 Strain gauge testing method
KHIN SANDA Q0805927 Page 33
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
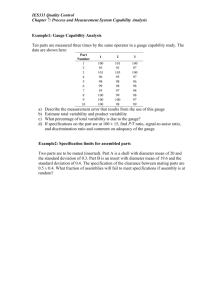
Height Rise UP
(mm)
0 (flat)
0.152
0.305
0.457
0.610
Vout Degree
2.45 0
2.47
2.49
0.01
0.03
2.51
2.53
Table 4 Result data
0.05
0.06
From table 2 it can be seen that different thickness of measuring gauge affect the strain gauge output voltage changes. The changes are 0.02V or 20mV.
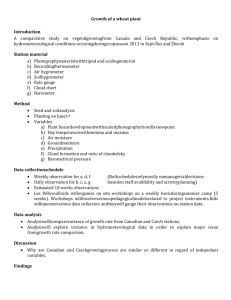
Figure 31 Height Vs Vout
The chart shows the linearity of Height (mm) Vs Vout. Vout increases when the height of the measuring gauge (mm) increases.
KHIN SANDA Q0805927 Page 34
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
The whole experiment was set up to prove that strain gauge application can be used for arterial tonometry technique. Based on Table 2 result it shows that strain gauge voltage output vary with different height measuring gauge or different angle. This is to simulate the voltage output variation which is developed by strain gauge height changes or angle elevated.
As shown in Figure 31 the result validate the voltage ranges depending on vessel diameters changes. Based on tested result, low blood pressure arise low output voltage while high blood pressure give higher voltage. However, the test was not done with actual human vessel to prove exact range.
The result shows that this model prototype detects the low/high blood pressure in the vessel.
As mentioned in Chapter 1 DVT patients have low pressure in veins. Using this proposed prototype method can be applied to early detection on DVT patients.
KHIN SANDA Q0805927 Page 35
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Chapter 4
Summary
In this chapter there are conclusion, difficulties that faced during building and testing of prototype, and last but not least recommendation for future work.
4.1 Conclusion
DVT patients are at a health risk as the early stage of this condition is not easily detected.
Therefore, the existence of this project proved to be a salvation for these patients. This project, early detection of DVT by non-invasive arterial tonometery technique allows the detection at an early stage. DVT patients have a much lower pressure in artery and in veins, especially in deep veins, which is situated in the legs. These facts have added on the complications of detecting such symptoms in DVT patients.
Early detection of DVT requires an accurate and sensitive sensor system in which this project is about. A strain gauge is a device used to measure the strain of an object. The most common type of strain gauge is made up of an insulating flexible backing which supports a metallic foil. Strain gauge sensor works in a way whereby a mechanical motion is converted into an electrical signal. The pressure changes in veins cause the bending of the vessel, which in turn trigger the voltage changes of strain gauge.
The prototype demonstrates that the pressure exerted on the vein wall, that causes the bending movement of the veins will trigger the movement of the shaft (contact stress sensor).
With the application of this technique, the result voltage varied linearly with respect to the feeler gague height between 0.1mm to 0.2mm. This measurement illustrate the concept of pressure differences applied on the vessel wall was detected non-invasively.
The design and structure of the prototype contributes to the results achieved. The cconceptual design and prototype proves that it can able to detect slight changes in pressure. The result proves that the changes in vein pressure provide the changes in output voltage. The result
KHIN SANDA Q0805927 Page 36
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE drives to the concept that shows the bending movement of the vessel wall will contribute to the aluminum shaft (contact stress sensor) movement. The output voltage varies depend on the movement of aluminum shaft.
Overall, the project prototype design proves that early detection of DVT can be achieved by non-invasive tonometery contact stress sensing method. In this project, learned about DVT and how it effects on people. DVT patients and normal people arteries and veins pressure differences are the focus points to learn and fundamental of the conceptual design. Low pressure in arteries and veins is observed in DVT patients. To detect the low pressure in arteries and veins require a sensitive sensor/transducer. It can be concluded that the project met most of the objectives. The conceptual design proves that it can be able to detect slight changes in pressure.
4.2 Difficulties
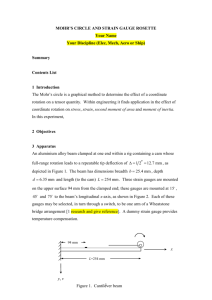
This project objective requires developing a hardware prototype. One of the difficulties is get all the hardware with the limited time frame. The first proposed (see figure 32) conceptual prototype includes the pump and the small diameter tubing to demonstrate as blood flow in the veins. Hence, it is another difficulty to get a pump which is adjustable and low pressure range due to low budget and limited time frame. However, the prototype was tested with a pump which is used for air con application. The testing was unsuccessful due to unsuitable pump for this prototype.
KHIN SANDA Q0805927 Page 37
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Pressure Pump
Figure 32 First proposed design
Pressure Gauge
Silicon Tube
KHIN SANDA Q0805927 Page 38
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Figure 33 Unsuitable pump
4.3 Recommendation
Nevertheless, there are areas for future work. Further testing is needed to become a clinically approved or commercially final product. As mentioned in conclusion, this conceptual design proves that pressure range varies the output voltage of the strain gauge. Future implementation shall add in the testing and data collection of pressure with respect to output voltage changes. This finding will determine whether one has potential risk of DVT which caused the low pressure in the veins.
On the other hand, the output voltages change 20mV is very useful and visible result for data collection. The analog result 20 mV difference can be used to convert to digital signal by PIC
Microcontroller. Analog data to digital data conversion would help to improve the prototype for future work.
KHIN SANDA Q0805927 Page 39
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
Chapter 5
Reflections
This project requires a good understanding of sensor theory, arteries vs. veins pressure, and other medical devices. As I am not well versed in this sensor theory, researches on books, journal papers and websites to search on more information on this project. At first I had difficulties understanding the sensor theory due to lack of hands on experiences. However, after countless in depth researches, I have thoroughly understood the whole idea on sensor theory and tasks I need to complete in order to achieve my objective.
First of all, the search for contact sensor application proved to be a great challenge for me.
Another dilemma that I faced during this period would be the choice between the different sensor type and application for prototype usage. To demonstrate the basic understanding of contact stress sensor prototype is required for my capstone project. But how to reach to that point is a challenge as mentioned above.
Apart from academic challenge in the area where research is concern, would be the budget given. The budget for this capstone project is S$100. Medical instruments and sensor systems are not at a comfortable price range; they cost more than a few thousand dollars. I am fine with topping up a few hundred dollars but a few thousand dollars will render impractical.
I have done researches on medical applications and devices as well and those are expensive as well. I am in the process of talking to my project supervisor Mr. Ching about the fact that I am unable to look for any sensor types which is suitable for my application prototype.
However, after few more weeks of research I have found that strain gauge suits best for my prototype which is suitable for my application, my idea, and my budget as well.
This is a hardware project, therefore there is more work needed as compared to software application where the only thing that needs to be done is to debug or test out. The basic prototype is required in order to demonstrate the basic understanding of contact stress sensor system. To get the components I have bought and collected one by one. Starting from a small
KHIN SANDA Q0805927 Page 40
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE wire to a strain gauge I have to look for it and find out the places which are selling those components. It is not easy to look for components due to my five days work commitment. I am a full time working and part-time student. Time is always an issue for me. It is hard to juggle between work and also spending time for this project due to work commitment.
I have demonstrated with a basic prototype despite of budget and time issue. This is all because of my strong commitment for my further education part time degree course. During this project period I hardly have time for my friends and family. Apart from my full time working hours I have spent most of my time for my project doing research to get the idea, getting components for the basic prototype, and building of the prototype. However, above all the difficulties and time constrain I have done a great job on my capstone project. Overall,
I’ve completed the task assign in my Gant Chart. The progress of this FYP is completed according to the Gantt Chart timeline which created and submitted in proposal report.
KHIN SANDA Q0805927 Page 41
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
References
[1] http://www.ebme.co.uk/arts/iabp/index.htm
[2] http://www.worldwidewounds.com/2000/sept/Michael-Lunt/Doppler-Imaging.html
(veins and arteries differences)
[3] http://www.faqs.org/patents/app/20090012411 (Patent)
[4] http://ieeexplore.ieee.org/xpl/freeabs_all.jsp?arnumber=4637985
[5] Joseph J.Carr and John M. Brown “Introduction to Biomedical Equipment Technology”
Fourth Edition (2001)
[6] Joseph D.Bronzino “Biomedical Engineering Handbook Medical Devices and System”
Third Edition (2006)
[7] Stanley E.Gunstream “Anatomy and Physiology with Integrated Study Guide” Third
Edition (2006)
[8] Jia-Jung Wang “Noninvasive Determination Of Arterial Pressure-Dependent Compliance
In Young Subjects Using An Arterial Tonometery” Vol.18 No.3 June 2006
[9] http://en.wikipedia.org/wiki/Sensor
[10]http://www.electronics-manufacturers.com/products/sensors-transducersdetectors/piezoelectric-sensor/
[11] http://www.sensorland.com
[12] http://zone.ni.com/devzone/cda/tut/p/id/3642
[13] http://www.emdt.co.uk/article/advantages-strain-gauge-technology
KHIN SANDA Q0805927 Page 42
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
[14] Foil Strain Gauge Data Sheet CAT No 3008, 5.1981
[15] http://www.astro-med.com/knowledge/dcbridgestrain.html
[16] LM358N data sheet
[17] http://www.webmd.com/dvt/deep-vein-thrombosis-dvt-symptoms-diagnosis
[18] http://en.wikipedia.org/wiki/Deep_vein_thrombosis
[19] http://www.innerbody.com/image/card05.html
[20] http://www.pathguy.com/histo/028.htm
[21] Matthew R. Nelson, MD, MS, Michael Cevette, PhD, Michael Covalciuc, MD, MPH, and R.Todd Hurst, MD, Noninvasive Measurement of Central Vascular Pressures With
Arterial Tonometry : Mayo Clinic Proceedings May 2010 vol. 85 no. 5 460-472
[22] Park M, Kang H, Huh Y, Kim KC, Cuffless and noninvasive tonometry mean arterial pressure measurement: Conf Proc IEEE Eng Med Biol Soc. 2006;1:6418-21
[23] HeffernaN KS, Karas RH, Patvardhan EA, Jafri H, Kuvin JT, Peripheral arterial tonometry for risk stratification in men with coronary artery disease : Clin Cardiol. 2010
Feb;33(2):94-8.
[24] Heffrnan KS, Karas RH, Mooney PJ, Patel AR, Kuvin JT, Pulse wave amplitude is associated brachial artery diameter:implications for gender difference in microvscular function : Vasc Med. 2010 Feb; 15(1):39-45.Epub 2009 Dec21
KHIN SANDA Q0805927 Page 43
EARLY DETECTION OF DVT BY NON-INVASIVE ARTERIAL TONOMETRY TECHNIQUE
[25] Bresler M, Sheffy K, Pillar G, Preiszler M, Differentiating between light and deep sleep stages using and ambulatory device based on peripheral arterial tonometry : Physiol Meas.
2008 May; 29(5):571-84. Epub 2008 May 7.
KHIN SANDA Q0805927 Page 44