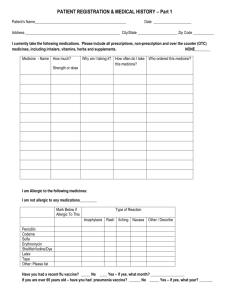
Adult Registration Questionnaire
advertisement

Please indicate which practice you would like to be registered with. ARMADA THE GREEN PHOTO VERIFIED ADDRESS VERIFIED CHECKED BY REGISTRATION QUESTIONNAIRE Welcome to Whitchurch Health Centre. When you are registered with us your old medical records from your previous doctor will automatically be sent to us. We would be very grateful if you could fill in the following questionnaire as completely as possible, and give it back to the receptionist. Thank you. Name Home Telephone Mobile Phone Email Date of Birth Occupation Marital Status 1. How would you like to receive correspondence from us: E-mail/Phone/Letter /Text 2. Are you a CARER YES/NO Do YOU have a carer Who do you care for …………………………………………… YES/No Who cares for you.…………………………………………. 3. Please state which ethnicity you are, this is very important for us to record ……………………………………………………………………………………………………………………………. 4. Lifestyle Data – Please circle your answers Have you ever smoked? If you answered Yes and you still smoke, please indicate how many of what per day If you smoke Roll ups how many ozs per week If an ex-smoker, please give the same details and the date you stopped smoking Yes No 5. Please answer the following questions using the Alcohol Intake key to help Alcohol Intake key – A Standard drink = 1 Unit (1pt = 2 units, 1 small wine = 1 unit, 1 single measure = 1 unit) How often do you have a drink that contains alcohol? How many standard alcohol drinks do you have on a typical day when you are drinking How often do you have 6 or more standard drinks on one occasion Never Monthly or less 2 – 4 times per month 2 – 3 times per week 4+ times per week 10+ Never How many alcohol drinks do you drink in a typical week. Less than monthly Pints Monthly Spirits (single measure) P.T.O Weekly Daily or almost daily Wine (small glass) 6. Exercise: How much exercise do you take in a week? ………………………………… 7. Please list any current medical problems 8. Past Medical History Please give details of any serious illnesses, operations or admissions to hospital. Please include any important medical condition for which you have received treatment 9. Allergies or severe side effects with Drugs and Tablets Please tick A, B or C below depending on whether you are allergic to or develop reactions to drugs or tablets and if so which drugs. A I am not allergic to any drugs [ ] B I am allergic to the following drugs [ Drug or tablet ] Description of side effects Date noticed C. I am allergic to some tablets but I cannot remember their name [ 10. Personal Data height…………… ] weight……………….. 11. Female patients only Are you currently pregnant, if yes please tell us your estimated date of delivery? ..................................................................................................................... 12. Family history Please list any serious illnesses that have occurred in your immediate family (i.e. Father/Mother/Brother/Sister), such as heart disease, stroke, high blood pressure, diabetes, asthma, cancer, Maternal hip fractures. NOTE: THIS ONLY APPLIES TO RELATIVES WHO WERE UNDER 70 YEARS OF AGE WHEN THE DISEASE STARTED. Relation Disease Approximate age at onset 13. Please tick this box if you would like us to invite you in for a new patient health check? Thank you for taking the time to complete this questionnaire. Please pass it to a Receptionist for processing.