Patient Registration Form Part 1
advertisement

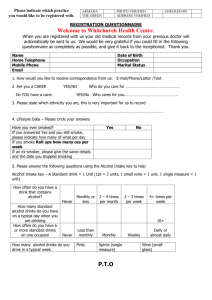
PATIENT REGISTRATION & MEDICAL HISTORY – Part 1 Patient’s Name________________________________________________ Date ____________________ Address __________________________________________________ City/State _____________________ Zip Code ___________ I currently take the following medications. Please include all prescriptions, non-prescription and over the counter (OTC) medicines, including inhalers, vitamins, herbs and supplements. NONE________ Medicine - Name How much? Strength or dose Why am I taking it? How often do I take Who ordered this medicine? this medicine? I am Allergic to the following medicines: I am not allergic to any medications_________ Mark Below if Allergic To This Type of Reaction Anaphylaxis Rash Itching Nausea Other / Describe Penicillin Codeine Sulfa Erythromycin Shellfish/Iodine/Dye Latex Tape Other: Please list Have you had a recent flu vaccine? _____ No ____ Yes – if yes, what month? __________________ If you are over 65 years old – have you had pneumonia vaccine? ______ No _____ Yes – if yes, what year? _______ Medical History- Please indicate if you have had any of the following problems (check all boxes that apply): I do not have any of the problems listed below_________ Disease/Problem I have this problem AIDS/HIV Positive Angina Asthma Bleeding Disorder Blood Clot Cancer Depression/Anxiety Diabetes Heart Attack Gout Heart Disease Hepatitis High Blood Pressure High Cholesterol Irregular Heart Rate Kidney Stones Kidney Disease Liver Disease Lung Disease Seizures Stroke Substance Abuse Tuberculosis Other : _________________________ Social History Smoking History: I have never smoked_____ I smoke a pipe or cigars____ I have quit ____ I smoke an e-cigarette____ I drink alcohol: Never_____ rarely _____ 7 or more drinks per day____ Yes I smoke_____ # of packs of cigs per day____ I chew tobacco_____ 1-2 drinks per day____ 3-4 drinks per day___ 5-6 drinks per day___ Past Medical History I have had the following surgical procedures performed: NONE__________ Year________ Operation_____________________________________ Which side? Right___ Left___ Does not apply___ Year________ Operation_____________________________________ Which side? Right___ Left___ Does not apply___ Year________ Operation_____________________________________ Which side? Right___ Left___ Does not apply___ Year________ Operation_____________________________________ Which side? Right___ Left___ Does not apply___ Family History: Please indicate if anyone in your family has had any of the following (check all boxes that apply): No one in my family has any of the problems listed below_________ Disease/Problem Father Mother Brother Sister Other Relative Indicate relationship AIDS/HIV Positive Angina Asthma Bleeding Disorder Blood Clot Cancer Depression/Anxiety Diabetes Heart Attack Gout Heart Disease Hepatitis High Blood Pressure High Cholesterol Irregular Heart Rate Kidney Stones Kidney Disease Liver Disease Lung Disease Seizures Stroke Substance Abuse Tuberculosis Other : _________________________ Review of Systems: Have you had any of the following during the past three months? Constitutional/ Paseo General Good Health Lately No Yes Musculoskeletal Joint Pain No Yes Recent Weight Change No Yes Joint stiffness or swelling No Yes Cardiovascular Irregular heart beat No Yes Weakness of muscles or joints No Yes Chest Pains No Yes Muscle pain or cramps No Yes Psychiatric / Psiquiátrico Memory Loss or confusion No Yes Back pain No Yes Nervousness No Yes Cold Extremities No Yes Depression No Yes Difficulty Walking No Yes No Yes Respiratory Asthma or wheezing No Yes Shortness of breath No Yes Sleep Problems