Study Organization and Administration (Section 1
advertisement

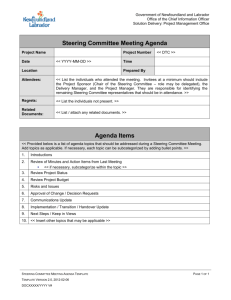
CHAPTER 2 STUDY ORGANIZATION, ADMINISTRATION, AND STAFFING 2.1. Overview The administrative structure of the MOTOR study is presented below. This structure includes a Data and Safety Monitoring Board, a Steering committee, an Executive Committee, a Statistical and Data Coordinating Center, a laboratory and 3 clinical performance sites. The NIDCR is the administrative head of the study and will be responsible for decisions regarding study continuation. DS MB NIDCR S teering Committee E xec utive Committee Data & S tatis tic al Coordinating Center L aboratory Clinic al F ield Centers UNC/Duke, UAB , UTHCS A Figure 1 2.2. Participating Units Project Office: Center for Oral and Systemic Diseases University of North Carolina at Chapel Hill UNC School of Dentistry Chapel Hill, NC Field Centers: Duke University Medical Center Department of Maternal and Fetal Medicine Durham, NC CHAPTER 2: Organization 10/09/06 Page 2 - 1 University of Alabama UAB School of Dentistry UAB School of Medicine Birmingham, AL University of Texas Health Science Center at San Antonio Department of Obstetrics and Gynecology Department of Periodontics San Antonio, TX Central Laboratory: Center for Oral and Systemic Diseases University of North Carolina at Chapel Hill UNC School of Dentistry Chapel Hill, NC Statistical and Data Coordinating Center: Collaborative Studies Coordinating Center University of North Carolina at Chapel Hill Chapel Hill, NC 2.3. The Data and Safety Monitoring Board The Data and Safety Monitoring Board (DSMB) is responsible for all aspects of safety and human subject’s protection for the study. The Board is an independent committee reporting to the NIDCR. The primary function of the DSMB is to review all issues pertinent to participant safety and study integrity. The primary role of the DSMB is to advise NIDCR on scientific, safety, ethical and other policy issues relating to the study. The DSMB will review and approve the study’s Manual of Procedures prior to study initiation and approve the progression from one phase of the trial to the next. During the execution of the study, the DSMB will monitor study progress and review interim analyses of accumulating study data. As appropriate, it will make recommendations to the Institute and Steering Committee concerning changes in study conduct. The DSMB will convene at least twice each year either in person or by teleconference depending on the nature of the workload and business to be conducted. For each DSMB meeting, the DSCC will provide reports on screening, recruitment and retention of participants in the study and on the number and type of adverse events. Although the potential is small for stopping the study as a result of interim analysis of treatment efficacy or adverse events, the DSMB is responsible for oversight of this activity, with appropriate data being supplied by the DSCC. CHAPTER 2: Organization 10/09/06 Page 2 - 2 2.4. The Steering Committee The Steering Committee is the policy making governing body for the study. The committee oversees all aspects of the design, execution, and publication of the study. The Steering Committee is composed of key Clinical Center and Coordinating Center Principal Investigators and the NIDRC Project Officer. The committee is chaired by Drs. Offenbacher and Beck. When a vote of the Steering Committee is necessary to make a decision, each member will have one vote. The Steering Committee will establish subcommittees to develop and monitor specific aspects of the study, such as decisions regarding publications, ancillary studies and stored biologicals. The subcommittees will submit recommendations for the Steering Committee’s approval; in turn, the Steering Committee will make recommendations for the Executive Committee to implement official changes in protocols and procedures. The Steering Committee will communicate though regularly scheduled meetings and conference calls to monitor the progress of the study. The Steering Committee will meet twice in the first year and once a year thereafter and the study coordinators will attend one of the two annual meetings. The Steering Committee will also have teleconference calls once a month for the first six months and twice a year thereafter, or as needed. 2.5. The Executive Committee The role of the Executive Committee (EC) is to conduct the day-to-day business for the Steering Committee. The Executive committee communicates with clinical center PIs and Study Coordinators to implement the policies and procedures as directed by the Steering Committee. The Executive Committee also serves as the liaison to bring issues from the investigators and staff to the Steering Committee for consideration of problem resolution, policy change and study modification or addendum. The Committee also develops the agendas and prepares recommendations for the Steering Committee meetings, and monitors interim progress of subcommittee tasks and participant recruitment. The Executive committee will be composed of either the periodontal or obstetric PI from each clinical center, Drs. Chambless and Couper from the Coordinating Center, and Drs. Offenbacher and Beck will chair this committee. The committee makes decisions consistent with policies set forth by the Steering committee regarding patient IRB issues, inclusion, exclusion criteria, protocol changes, data collection instruments, OB and dental examinations and sample collection methods. This committee will meet twice in person the first year and once a year thereafter as part of the Steering Committee. Teleconferences will be held twice a month for the first year and monthly thereafter. CHAPTER 2: Organization 10/09/06 Page 2 - 3 2.6. The Statistical and Data Coordinating Center The Statistical and Data Coordinating Center (DSCC) develops procedures for collecting, editing, storing, and analyzing data generated by the clinical centers. The coordinating center is responsible for developing the protocol manual, creating data collection instruments, training, calibrating and certifying the clinical centers, coordinating steering committee and executive committee meetings, and monitoring the study and reporting information to the DSMB and Steering Committee. The DSCC is located in the Collaborative Studies Coordinating Center (CSCC), a unit in the Department of Biostatistics at UNC. The Principal Investigator of the DSCC is a member of the Steering and Executive Committees. They report on DSCC activities to the Steering Committee and the DSMB. The DSCC, through a combination of written manuals and centralized and on-site training, will design and implement quality control programs for data collection, data transfer, sample transfer, eligibility determination, intervention delivery, and central laboratory determinations. The Coordinating Center will provide statistical expertise for the study design, perform data analyses, and participate in the preparation of scientific presentations and publications. The DSCC will plan and implement procedures to monitor adverse events and endpoints, including training clinic staff in the data collection needed. The DSCC will administer procedures for adjudication of endpoints such as the length of gestation. The DSCC will participate in on-site audits of the clinical centers to confirm that the protocol is being conducted as specified, that the reported data reported are accurate and complete, and that the human research requirements are appropriately satisfied. These audits will be conducted at least annually while participants are being enrolled and followed. The SDCC monitors the study and sends reports to the DSMB and the Steering Committee. The SDCC provides information to the DSMB on safety, adverse events, human subjects’ issues and other key aspects of the study. The SDCC also prepares periodic data quality monitoring reports to identify any patterns in the data that may be reflective of lack of standardization between clinical centers and/or study staff. These reports will be reviewed by the Steering Committee and be shared with the study agencies and their investigators. Corrective actions will be requested when necessary. 2.7. Subcommittees Subcommittees are established by the Steering Committee to develop and monitor various aspects of the study. Subcommittee members include both PIs and staff of the Clinical Centers and Coordinating Center, and representatives from the Project Office, as appropriate. The Subcommittee Chairs are elected by the subcommittees, subject to Steering Committee review and approval. Subcommittees develop recommendations and proposals for Steering Committee review and decision. The following subcommittees have been or will be established during the study: CHAPTER 2: Organization 10/09/06 Page 2 - 4 Periodontal Subcommittee Obstetrics Subcommittee Study/Project Coordinator Subcommittee Publications and Analysis Subcommittee Biologicals Subcommittee 2.8. Staffing and Training 2.8.1. Clinical Center Staffing and Responsibilities Each Clinical Centers Principal Investigator will have overall administrative, scientific and fiscal responsibility for that site. The Study Coordinator will be responsible for its day-to-day operation, coordinating all activities of the Principal Investigator and other study personnel and ensuring that data are collected in an accurate, timely and efficient manner. The on-site study coordinators will work closely with the Study Manager of the Data and Statistical Coordinating Center to ensure that all data forms are completed in an accurate and timely manner. Before screening and randomization can begin at any center, the center must have the following: (note that some of these tasks can be performed by the same person, as long as the masking to treatment assignment as specified in the MOTOR protocol is followed): At least one Study/Project Coordinator who has participated in a training session. At least one Obstetric examiner, properly trained and certified to conduct the study examination as described in the study MOP. At least one properly trained and calibrated Dental Examiner. At least one Dental Therapist, properly trained and certified to conduct the study therapy as described in the study MOP. At least one person trained and certified for use on MOTOR Data Management System, and the MOTOR Periodontal Data Entry System. IRB approval for the study and the consent form, and a copy of each on file with the Operations Center. Indication from the DSCCS that the MOTOR DMS is complete and ready for study start-up. Each individual center must be certified by fulfilling both the center-wide requirements and individual personnel requirements. The center-wide requirements consist of: 1. Receipt of the final version of the manual of operations, study protocol, and data forms. 2. IRB approval and a sample consent form on file at DSCC. If consent will be asked in a language other than English, a copy of the consent for in that language should also be sent to the DSCC. 3. Identification of the Study/Project Coordinator(s) to be certified for the study. 4. Identification of the all individual(s) responsible for data collection and treatment procedures. CHAPTER 2: Organization 10/09/06 Page 2 - 5 Certification of study personnel is an essential aspect of effective quality assurance. In order to minimize error and ensure continuous quality control and consistency in collection of data despite potential study personnel turnover over the long-term followup period, the Data Coordinating Center (DSCC) and the Project Office are jointly responsible for establishing and providing the requisite minimum criteria and training and ensuring continued adherence to study protocol and standards of clinical research. The complexity of the study design requires that the Study/Project Coordinators, Obstetric and Dental Examiners all be instructed and certified on specific tasks. To protect the quality of the study results, data are to be collected by certified personnel only. 2.8.2. Study/Project Coordinator Study/Project Coordinators are responsible for providing the thread of continuity from patient recruitment, evaluation and treatment through follow-up, and ultimately trial closeout. Coordinators routinely initiate recruitment, conduct interviews and administer questionnaires. Coordinators serve as the liaison with the Project Office, the DSCC, the Central Laboratories, and the clinical sites. They familiarize their Investigators with study procedures and implement operational modifications. The Study Coordinator is ultimately responsible for accurate collection of data and data entry at the clinical site and its transfer to the DSCC. The Coordinator is also responsible for overseeing the shipment of blood samples to the laboratory. Therefore, an in-depth knowledge of all aspects of the protocol is required. As such, Study/Project Coordinators attend a training session initially held before recruitment into MOTOR commences. Study Coordinators in MOTOR can be OB nurses, dental hygienists, or other staff who are appropriate for the responsibilities and are study trained. Study Coordinators can delegate the tasks listed below, but maintain the responsibility of assuring the tasks are completed per protocol. Specific responsibilities include the following: 1. Establishing a method to ensure that all patients who are 160—236 are evaluated for study eligibility. 2. Obtaining and reviewing the medical records of the participant’s current health and pregnancy and previous pregnancy records, if available, to determine eligibility. 3. Arranging a system for obtaining accurate gestational age information, including scheduling an ultrasound for dating and to rule out fetal anomalies and multi-fetal gestation before patient enrollment if one has not been performed previously. 4. Obtaining signed informed consents from prospective participants as indicated by the protocol. 5. Arranging for the ordering and storage (storing) of study supplies. 6. Collecting maternal and neonatal information necessary to complete all study forms. 7. Training and certifying staff in data collection, forms completion, and data entry. CHAPTER 2: Organization 10/09/06 Page 2 - 6 8. Coordinating data entry, including controlling access to the laptop computer and assuring that required backup security and confidentiality procedures are maintained. 9. Ensuring the timely collection of data required for hospital records abstraction and endpoint identification and resolution. 10. Responding to edit / audit messages and other communications from the Data & Statistical Coordinating Center. 11. Organizing and maintaining central records, including the protocol, manual, data forms, reports, correspondence, and study personnel and address lists. 12. Reporting possible adverse events to the DSCC. 2.8.2.1. Training and Certification of Project Coordinators Every Study Coordinator must be trained by the DSCC and PO. If a field site has more than one Study Coordinator, then the DSCC and the PO must train each study coordinator. A central training session for Project Coordinators will be held before recruitment starts. The purpose of the training workshop is to review the study design, objectives, procedures, and data collection forms. The coordinators, in turn, are responsible for training any additional staff assigned to this study. In general, attendance at the training session certifies the Project Coordinator in administration of questionnaires. Proficiency in all aspects of collection of data on paper forms and in the use of the computerized Data Management System (DMS) is required to ensure the accuracy and integrity of the collaborative database. At the central training, the Study Coordinator must demonstrate proficiency in the use of the study’s laptop computer system to be certified for data entry and participant randomization on the DMS. Once trained, a Study Coordinator can subsequently train additional personnel (auxiliary, back-up), provided each person passes certification requirements specific to the activity. In most clinical centers it is expected that the Study Coordinator will perform all duties relevant to screening and randomization. The Study Coordinators at each site are not blinded to the periodontal treatment assignment (group 1 or 2), unless they are involved in data collection procedures posttreatment. In the event that the Study Coordinator collects any post-treatment data, the Coordinator should assign randomization and prenatal treatment scheduling to another staff member who does not collect post-treatment data. The Coordinators are responsible for implementation of procedures at their site that assures appropriate blinding of all other staff members to the random assignment. In addition to central training at study launch, regular Coordinator conference calls (at least monthly) will be scheduled with the DSCC to continue any training and discuss protocol and procedural issues as they arise. Recertification may occasionally be necessary. The need for recertification on any of the study certification requirements may be triggered by monitoring visits. Or It may CHAPTER 2: Organization 10/09/06 Page 2 - 7 result from a recommendation by the Data and Safety Monitoring Board or Executive Committee upon review of the data. This recertification may be study-wide or clinicspecific. 2.8.3. Dental Examiners Dental Examiners are licensed dental hygienists and/or general dentists/periodontists, i.e., dental professionals with extensive experience in dental/oral examinations. The dental examiners will be responsible for conducting the dental screening during recruitment, for baseline and follow-up dental/periodontal evaluations and plaque sample collection, and for providing the study treatment for participants. Other data collection activities by the dental examiner can include collecting and recording of physical examination data (blood pressure, heart rate, and height and weight), collecting and recording changes in participant medical history and medication history, and recording adverse events. 2.8.3.1. Training and Certification of Dental Examiners All dental examiners are to be trained in study procedures and calibrated prior to their participation in the study. The Dental Examiners are calibrated on all periodontal measurements and indices to be utilized in the study to ensure adequate intra- and inter-examiner measurement reliability. Both chair-side and bedside calibration are to be performed. Dental examiners are also trained to the study standards necessary for treatment delivery. Only examiners who have been calibrated and reached the level of examiner agreement stipulated can take part in the MOTOR study. The training procedures to be followed for examiners’ training and calibration are described in detail in the Manual for Examiner Training and Calibration (Appendix 2). In addition to measurement procedures, the examiner must also be trained to enter the examination data into the MOTOR Dental Data Entry System (DDES). The DDES is an interactive program contained on a study laptop for entry of all periodontal scores and measures. The DDES is a program that is unfamiliar to most examiners. Though many are experienced with other periodontal examination data entry systems, the data field ordering, naming conventions, and nomenclature are not standardized. Data entry of a periodontal exam will require synchronization and communication between the examiner and the recorder in order to provide accurate data in a timely manner. Dental examiners or Project Coordinators will be responsible for training recorders on the use of the DDES. Practice sessions are integral to the training and certification process. They provide familiarization with the system, and allow piloting of the MOTOR forms and procedures prior to the start of the study. And they are a required part of the certification process for both examiners and recorders CHAPTER 2: Organization 10/09/06 Page 2 - 8 2.8.4. OB Records Abstractor Many of the OB forms require medical records review and abstraction. The records abstractor may be the Project Coordinator, OB nurse, dental hygienist, or other staff member appropriately trained and familiar with their site’s medical records. 2.8.4.1. Training and Certification for OB Abstractor Persons involved with abstraction onto MOTOR forms, must be trained and certified for data collection. Training either at the central Coordinator’s training, or by their Site’s Coordinator, should include a review of the study design, objectives, procedures, and data collection forms. In addition, each abstractor must be trained at their site on the use of their Clinic’s medical charts systems. 2.8.5. Additional Personnel, including Data Entry Personnel After the Study Coordinator, Dental Examiner, and OB nurse meet training and certification requirements, they (or the DSCC staff) may train additional personnel to perform tasks related to the MOTOR study, under certain conditions. As long as the study requirements are met, the additional personnel may perform one or all of the following tasks Local laboratory personnel may perform blood-processing activities. In this case, the Study Coordinator is still responsible for study protocol and must be certified in blood collection and processing. However, lab technicians do not need to become MOTOR certified; the laboratory technician’s name is entered on the phlebotomy form as the person processing the blood. Data entry personnel may enter data into the DMS from paper forms that have been completed by certified personnel. Prior to entering the data, they must be trained and certified by a DMS-certified Study Coordinator or by DSCC staff (e.g., during a monitoring visit). These technicians are certified for entering data into the DMS only. 2.8.6. Staff Turnover If the primary Study Coordinator leaves the study, certified and auxiliary back-up personnel can continue to function in their roles. For centers with auxiliary personnel, it is recommended that a new Coordinator be identified and certified as quickly as possible in the areas the previous Coordinator handled exclusively. If the center has someone certified in every aspect of the study (combination of new, auxiliary, and backup personnel), the center can continue study activities. A back-up Coordinator who has completed all certifications may be designated as the new Study Coordinator with no interruption of study activities. Or the fully certified backup Coordinator may continue all study activities until a new primary Coordinator is trained and certified. Situations where a new primary Study Coordinator is hired, and is new to the study and procedures, may require training by the DSCC/PO (decision to made by the DSCC). In CHAPTER 2: Organization 10/09/06 Page 2 - 9 that event, randomizations must cease until the new Study Coordinator is trained and certified by attending a central training or a study center on-site training and then completing his/her certifications. Effort will be made to complete the training within 30 days of loss of the primary study coordinator. CHAPTER 2: Organization 10/09/06 Page 2 - 10