1002 Clinical Assessment (PIHP) (Handwritten).
advertisement
 (Handwritten).")
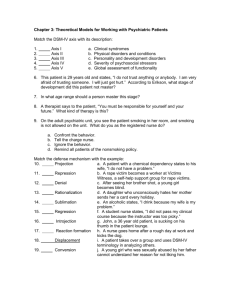
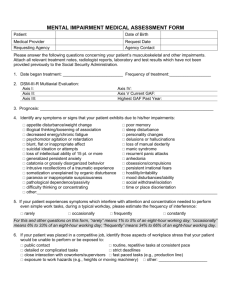
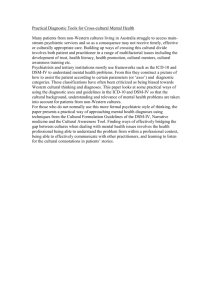
CLINICAL ASSESSMENT Consumer: Case #: Start Time: Stop Time: Date: Presenting Concerns/Historical Concerns: Potential Medical Complications Related to Mental Status: History of Substance Use: Yes No; (If Yes, update/complete SUD Chart): History of Mental Health/SUD Treatment: form): Yes No; (If Yes, update/complete History of Mental Health/SUD Treatment a. Prior Diagnosis: b. Prior Response to Treatment/Medication: Lethality/At Risk: a. Suicidal/homicidal thoughts, gestures, plan: Yes No; If Yes, complete Lethality Assessment b. Self Care Issues: Yes No; If Yes, see diagnostic formulation c. Duty to Warn: Yes No; If Yes, indicate who was notified, when, and by what method: Clinical Assessment Page 1 of 5 Form #1002 Rev: 1/14 Consumer Name: ______________________ Case Number: ________________ Mental Status Exam: Status – degree of distress/disturbance/dysfunction Appearance: Grooming Clothing Unusual Physical Characteristics Comments on Appearance: 1-Unremarkable 2-Minor 3-Moderate 4-Severe Status – degree of distress/disturbance/dysfunction Behavior: 1-Unremarkable 2-Minor 3-Moderate 4-Severe Posture Facial Expression General Body Movements Amplitude and Quality of Speech Provider – Consumer Relationship Comments on Behavior: Status – degree of distress/disturbance/dysfunction Affect/Mood: 1-Unremarkable Range Spontaneity Appropriateness Comments on Affect/Mood: Clinical Assessment Form #1002 Rev: 1/14 Page 2 of 5 D:\106741783.doc 2-Minor 3-Moderate 4-Severe Consumer Name: ______________________ Case Number: ________________ Status – degree of distress/disturbance/dysfunction Perception: 1-Unremarkable 2-Minor 3-Moderate 4-Severe Delusions Hallucinations Comments on Perception: Status – degree of distress/disturbance/dysfunction Thinking: 1-Unremarkable Intellectual Functioning Orientation Insight Judgment Memory Thought Content Stream of Thought Manifested in Speech Comments on Thinking: Mental Status Exam Summary: Clinical Assessment Form #1002 Rev: 1/14 Page 3 of 5 D:\106741783.doc 2-Minor 3-Moderate 4-Severe Consumer Name: ______________________ Case Number: ________________ Diagnostic Formulations; including as appropriate, differential diagnosis and diagnostic formulations of family functioning: DSM IV Diagnosis: Axis I: Primary Secondary Tertiary SA Primary SA Secondary DSM-IV / Description Axis II: Primary Secondary DSM-IV / Description Axis III (qualifying/state reported axis III information only): Primary Secondary Tertiary DSM-IV / Description Axis IV: Economic problems Problem with primary support group Problem accessing healthcare Problem related to social environment Educational problems housing problems Problem related to interaction with legal system Occupational problems Other psychological and environmental problems Housing problems Axis V: Current GAF Diagnostic Summary: Diagnosis made by: Prognosis: Good Clinical Assessment Form #1002 Rev: 1/14 Date: Fair Poor Last Update: Guarded Page 4 of 5 D:\106741783.doc Consumer Name: ______________________ Case Number: ________________ Specific Clinical Recommendations: Clinician Signature/Credentials Date Psychiatric Signature Date Supervisor Signature (optional) (Required for all BC/BS, Medicare cases within 10 days from date of assessment) Clinical Assessment Form #1002 Rev: 1/14 Page 5 of 5 D:\106741783.doc Date