Management of Diabetes at North Bay Order Form This order is valid
advertisement

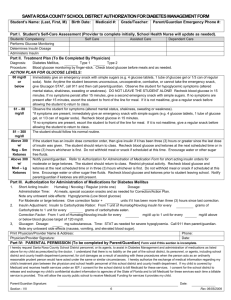
Management of Diabetes at North Bay Order Form This order is valid only for the dates the student is attending camp. Student: __________________________________________ DOB: ______________ School: __________________________________ Dates at camp: _______________________________ CONTACT INFORMATION: Parent/Guardian: __________________________ Home Phone: _______________ Work: _________________ Cell:___________________________ Other Emergency Contact: ________________________ Home Phone: ____________________Work: _________________Cell: __________________ INSULIN ORDERS: 1. Insulin administration via: � Syringe and vial � Insulin pen � Insulin pump � Other _______________________________ If on insulin pump indicate type of pump ______________________ and basal rates ____________________ *must also fill out insulin pump form 2. Insulin Before Meals and at Bedtime: Name of insulin: _____________________ � Routine dose: __________________________ � Per sliding scale as follows Blood Glucose ________ to ________ give _________ units Blood Glucose ________ to ________ give _________ units Blood Glucose ________ to ________ give _________ units Blood Glucose ________ to ________ give _________ units Blood Glucose ________ to ________ give _________ units Blood Glucose ________ to ________ give _________ units Blood Glucose ________ to ________ give _________ units Blood Glucose ________ to ________ give _________ units Blood Glucose ________ to ________ give _________ units Blood Glucose ________ to ________ give _________ units � Calculated insulin dose (add carbohydrate coverage and correction dose for total insulin does): Carbohydrate Coverage: Insulin to carbohydrate ratio o Give _______ units insulin per _______ grams carbohydrate o Correction: Give _______ units insulin per _______ mg/dl of glucose above _______ mg/dl Subtract _______ units insulin per _______ mg/dl of glucose below _______ mg/dl 3. Other times insulin may be given: � Snack: � Dose: ___________ � Calculated as above � Ketones: If ketones are __________ Give/Add __________ units If ketones are __________ Give/Add __________ units Health Care Provider Authorization for Management of Diabetes at North Bay Camp My signature below provides authorization for the above written orders. This authorization is for while the student is attending North Bay Camp. Health Care Provider Name: _________________________________ Signature: _______________________________ (original or stamped signature) *Sign both sides. Phone: _______________________ Fax: ___________________________Date: ___________ Parent Consent for Management of Diabetes at North Bay Camp I (We) request designated North Bay personnel to administer the medication and treatment orders as prescribed above. I agree: 1. To provide the necessary supplies and equipment 2. To notify the school nurse if there is a change in the student’s diabetes management or health care provider. I authorize the school nurse to communicate with the health care provider as necessary. Parent/Guardian Signature __________________________________________________ Date ____________________ *Sign both sides. Order reviewed and signed by Camp Nurse: ___________________________________________ Date: ______________ North Bay Management of Diabetes at Camp Order Form Student: ______________________________ School: _______________________ Dates attending: _______________ Blood Glucose Monitoring: Target range for blood glucose monitoring at school: ___________________________ � Before snacks � 2 hours or _______ hours after lunch � Before meals � 2 hours or ______ hours after a correction dose � As needed for symptoms of hypo/hyperglycemia � With signs and symptoms of illness � Other times: ______________________ Hypoglycemia – Blood glucose less than __________ � Self-treatment for mild lows. � Give ____ grams of fast-acting carbohydrate according to care plan. Recheck BG in 10-15 min. Repeat treatment if BG < ____ mg/dl � Provide extra protein & carbohydrate snack after treating low if next meal/snack is greater than ______ minutes away � Suspend pump for severe hypoglycemia for ______ minutes If student is unconscious, having a seizure or unable to swallow, presume student is having a low blood sugar Call 911 & notify parent and school point person. � Glucagon injection (1mg in 1cc) _______mg, SQ or IM � OK to use glucose gel inside cheek, even if unconscious or seizing � Other: _________________________________ Hyperglycemia – Blood glucose greater than ___________ � Check urine ketones, follow care plan, administer insulin as per orders. � For pumps, insulin may be given by syringe or pen if needed � Encourage sugar free fluids, at least ______ ounces per ______. � If student complains of nausea, vomiting or abdominal pain; check urine ketones and check insulin administration orders. � Other: _________________________________________ ** Transport to local ED may be needed with vomiting and large ketones. ** Meal Plan � AM snack time: _______ � PM snack time: ________ � Avoid snack of BGL is > ______ mg/dl. � Breakfast¨___________ � Lunch: ______________ � Dinner: ___________ � Extra food allowed: � Parent discretion � Student discretion Exercise (check and/or complete all that apply) Fast-acting carbohydrate source must be available before, during and after all exercise � With student � With teacher If most recent blood glucose is less than ________, exercise can occur when blood glucose is corrected and above _________ � Eat ______ grams of carbohydrate; � Before exercise � Every 30 minutes during � After vigorous exercise � Avoid exercise when blood glucose is greater than ________ or ketones are _________ Bus Transportation � Blood glucose monitoring not required prior to boarding bus � Check blood glucose 15 minutes prior to boarding bus � Allow student to eat on bus if having symptoms of low blood glucose � Provide care as follows: _________________________________________________________________________________________ Health Care Provider Assessment Student can self-perform the following procedures (school nurse and parent must verify competency): � Blood glucose monitoring � Measuring insulin � Injecting insulin � Determining insulin dose � Independently operating insulin pump � Other: _______________________________________________________________________________________________________ Disaster Plan (if needed for lockdown, 24hr shelter in place): � Follow insulin orders as on Management Form � Additional insulin orders as follows: ______________________________________________________ � Administer long acting insulin as follows: ________________________________________________________________ � Other: ______________________________________________________________________________________________________ Other Instructions: _______________________________________________________________________________________________________________ Health Care Provider Signature (required): ______________________________________ Phone: ______________ Date: __________ Parent Signature (required): __________________________________________________ Phone: _______________ Date: _________ Order reviewed by North Bay nurse: ___________________________________________________________ Date: _______________