Problem 77- Infertility and Sexual Dysfunction
advertisement

Infertility and Sexual Dysfunction
The Reproductive System
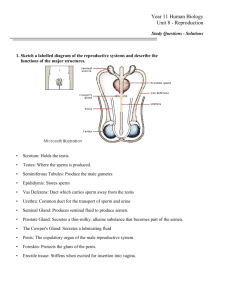
The uterus is characterized by the following regions:
The fundus is the upper region where the uterine ducts join the uterus.
The body is the major, central portion of the uterus.
The isthmus is the lower, narrow portion of the uterus.
The cervix is a narrow region at the bottom of the uterus that leads to the vagina. The inside
of the cervix, or cervical canal, opens to the uterus above through the internal os and to the
vagina below through the external os. Cervical mucus secreted by the mucosa layer of the
cervical canal serves to protect against bacteria entering the uterus from the vagina. If an
oocyte is available for fertilization, the mucus becomes thin and slightly alkaline. These are
attributes that promote the passage of sperm. At other times, the mucus is viscous and
impedes the passage of sperm.
The uterus is held in place by the following ligaments:
Broad ligaments
Uterosacral ligaments
Round ligaments
Cardinal (lateral cervical) ligaments
The wall of the uterus consists of the following three layers:
The perimetrium is a serous membrane that lines the outside of the uterus.
The myometrium consists of several layers of smooth muscle and imparts the bulk of the
uterine wall. Contractions of these muscles during childbirth help force the fetus out of the
uterus.
The endometrium is the highly vascularized mucosa that lines the inside of the uterus. If an
oocyte has been fertilized by a sperm, the zygote (the fertilized egg) implants on this tissue.
The endometrium itself consists of two layers. The stratum functionalis (functional layer) is
the innermost layer (facing the uterine lumen) and is shed during menstruation. The
outermost stratum basalis (basal layer) is permanent and generates each new stratum
functionalis
Infertility
Infertility is defined as an inability to conceive. The term subfertility may be preferable to infertility
as many of the bars to conception are relative rather than absolute (sterility)
In about 30% of cases no cause is found.
Some degree of difficulty conceiving is normal. Even with regular intercourse, 6% of women aged 35
years and 23% of those aged 38 years will not conceive after three years.
About 84% of all couples (in normal reproductive age range) will conceive within one year and 92%
within two years
Primary infertility: Diminished fertility throughout reproductive years
Secondary infertility: Failure to conceive after one or more successful pregnancies
Causes
Ovulatory (20%)
Tubal (14%)
Male (19%)
Unexplained (30%)
Endometriosis
Initial review in couple with infertility
Age
Occupation
Education
Number of years trying
Contraception history
Previous miscarriages and pregnancies- is this primary or secondary?
Coital history – dyspareunia, impotence, ejaculation disorders
Previous STI history
Past medical history (see later notes)
Female infertility
Primary amenorrhoea
Secondary sexual characteristics present:
Genitourinary malformation:
Imperforate hymen,
Absent uterus
Androgen insensitivity syndrome ('testicular feminization'):
46XY female (breast development present but reduced, and pubic/axillary hair absent)
Endocrine disease:
Hypothyroidism,
Hyperthyroidism,
Hyperprolactinaemia (prolactinoma or drugs),
Cushing's syndrome.
PCOS.
Absence of secondary sexual characteristics
Ovarian failure:
Gonadal dysgenesis (as in Turner's syndrome, 46XO)
Gonadal agenesis (46XX or 46XY)
Premature ovarian failure
Chemotherapy
Pelvic irradiation.
Hypothalamic dysfunction:
Chronic systemic illness (including uncontrolled diabetes, severe renal and cardiac Disorders,
coeliac disease, cancer, and infections such as tuberculosis),
Eating disorders,
Weight loss,
Excessive exercise,
Stress,
Depression.
Other causes of gonadotrophin deficiency:
Head injury,
Infection,
Cranial irradiation,
Tumours of the hypothalamus and pituitary,
Hydrocephalus,
Kallman's syndrome (congenital gonadotrophin deficiency characterized by anosmia and
other cranial anomalies),
Empty sella syndrome,
Präder–Willi syndrome.
Ambiguous genitalia
5-alpha-reductase deficiency. The external genitalia are female, but the internal genitalia are
male.
Androgen-secreting tumour. This is rare and results in extreme virilization characterized by
temporal balding, clitoral enlargement, deepening of the voice, and extreme hirsutism.
Congenital adrenal hyperplasia. As a result of an enzyme deficiency, the adrenal gland produces
too much androgen, resulting in female babies developing male characteristics. The degree of
virilization varies and can be of late onset.
Secondary amenorrhoea
Features of androgen excess
Iatrogenic
Contraceptive pill,
Radiotherapy,
Chemotherapy,
Surgery (oophorectomy, hysterectomy, endometrial resection);
Drugs causing hyperprolactinaemia (antipsychotics, metoclopramide, methyldopa,
cimetidine, opiates, cocaine).
Uterine causes:
Cervical stenosis,
Asherman's syndrome (intrauterine adhesions).
Ovarian causes:
premature ovarian failure,
resistant ovary syndrome,
chemotherapy or pelvic irradiation,
mosaic Turner's syndrome.
Hypothalamic dysfunction:
weight loss,
eating disorders,
excessive exercise,
stress, depression,
chronic systemic illness (severe cardiac, renal, or liver disease; inflammatory bowel disease;
coeliac disease; AIDS; or cancer),
idiopathic.
Pituitary causes
prolactinoma,
other hormone-secreting pituitary tumours,
head injury,
Sheehan's syndrome (pituitary infarction after major obstetric haemorrhage), sarcoidosis,
tuberculosis,
cranial irradiation.
Thyroid disease:
hypothyroidism,
hyperthyroidism.
No features of androgen excess
Endocrine causes:
Polycystic ovary syndrome,
Cushing's syndrome,
Late-onset congenital adrenal hyperplasia.
Tumour:
androgen-secreting tumours of the ovary or adrenal gland.
Most common pathological causes of
secondary ameonorrhoea
PCOS
Hypothalamic suppression (by weight
loss, excessive exercise, or chronic
systemic illness)
Premature ovarian failure,
Hyperprolactinaemia
Pelvic Inflammatory disease (PID)
Occlude fibriae end. Fluid=hydrosalpinx, pus=pyosalpinx
Acute salpingitis=STI (Chlamydia most common, or gonorrhea, e.coli, anaerobes, haemolytic strpe,
C.welchii)
Incidence of damage = 8% first episode
16% second episode
40% third episode
Uterine cavity lesions
Controversial
Fibroids do not interfere unless they distort uterine cavity
Asherman’s syndrome
o Damage to basal endothelium after dilation and curettage procedure, usually
following incomplete miscarriage, TOP or delivery. Leads to intrauterine scars and
adhesions causing secondary amenorrhoea, infertility and pain.
Congenital abnormalities of the uterus do not interfere with conception but can lead to
miscarriage
Investigations in the female
Detection of ovulation
o Temperature (rises 0.5C in luteal phase menstrual cycle
o Cervical mucus (increases in follicular phase and peaks at ovulationprofuse, clear
acellular mucus of low viscosity and high stretchability)
o Hormone tests (FSH&LH peak 20 hours before ovulation)
o Endometrial biopsy (secretory ohase endothelium =ovulation)
o USS ovaries, assess follicular growth
o Laparoscopy
Non-ovulatory causes
o Serum Prolactin
o FSH and LH (High GnRH and low LH?FSH suggests ovarian failure)
o TFT
o Radiography of skull if ?prolactinoma
o Hysterosalpingography/laparoscopy (if ?tubal)
Test
LH
FSH
Prl
Progesterone
Premenstrual
3-13 u/L
Follicular
Ovulatory
Luteal
peak
phase
3-12
20=80
3-16
0.5-5
8-15
2-8
Women<600: Men<450
<2 prior to ovulation, >5 after ovulation.
Rises to 100-200 at term in pregnancy
Post
menopausal
>30
>30
Male infertility
1.Pre-testicular
3. Post-testicular
2. Testicular
1. Pre testicular causes
Hypogonadotropic hypogonadism due to various causes
Obesity increases the risk of hypogonadotropic hypogonadism.
Drugs, alcohol
Strenuous bicycle riding (controversial)
Medications
affect spermatogenesis e.g. chemotherapy, anabolic
steroids, cimetidine, spironolactone
decrease FSH levels e.g. phenytoin;
sperm motility e.g. sulfasalazine and nitrofurantoin
Genetic abnormalities such as a Robertsonian translocation
SMOKING
Male smokers also have approximately 30% higher odds of infertility.
2. Testicular causes
Testicular factors refer to conditions where the testes produce semen of low quantity and/or poor
quality despite adequate hormonal support and include:
Age
Klinefelter syndrome
Neoplasm, e.g. seminoma
Idiopathic failure
Cryptorchidism
Varicocele (14% in one study)
Trauma
Hydrocele
Mumps
Malaria
Testicular cancer
Defects in USP26 in some cases
Acrosomal defects affecting egg penetration
Idiopathic oligospermia - unexplained sperm deficiencies account for 30% of male infertility
Radiation therapy to a testis decreases its function, but infertility can efficiently be avoided by
avoiding radiation to both testes.
3. Post-testicular causes
Post-testicular factors decrease male fertility due to conditions that affect the male genital system
after testicular sperm production and include defects of the genital tract as well as problems in
ejaculation:
Vas deferens obstruction
Lack of Vas deferens, often related to genetic markers for Cystic Fibrosis
Infection, e.g. prostatitis
Retrograde ejaculation
Ejaculatory duct obstruction
Hypospadias
Impotence
Investigations in the male
Sperm analysis
Volume 2-5 ml
Count >20x106
Motility >50%
Morphology >30% normal
Liquefaction within 30 mins
WCC < 106/ml
Oligospermia or Oligozoospermia - decreased number of spermatozoa in semen
Aspermia - complete lack of semen
Hypospermia - reduced seminal volume
Azoospermia - absence of sperm cells in semen
Teratospermia - increase in sperm with abnormal morphology
Asthenozoospermia - reduced sperm motility
Hormone studies
High FSH = testicular damage
Normal FSH= obstructive disease
Low FSH= hypopituitaryism
High LH and low testosterone in Kleinfelters
High prolactin= pituitary adenoma impotence and oligospermia
Cytogenic studies
Karyotype XXY/XYY
2% infertile males have abnormal karyotype
Testicular biopsy
Only when ?obstructive cause
Immunological tests
Autoimmunity to sperm antigens – neutralizing sperm decapacitation/block sperm receptors on egg.
Antibodies may be in male or female serum, cervical mucus or seminal plasma.
Look for IgG, IgA in seminal plasma
Erectile dysfunction
The inability to achieve or maintain an erection long enough to engage in sexual intercourse.
Psychological
Hormonal
Vascular
Neurological
Risk factors for ED
Smoking
Diabetes
Hypertension
Hyperlipidaemia
Depression
Obesity
Trauma/surgery to spine
Drugs:SSRI’s, antihypertensives (betablockers)
Endocrine: Hypothyroid
3x increased risk of ED in men with Diabetes. Tends to present earlier and more severe.
Complications
Treatment
Insufficient female arousal
Pain and dryness
Frustration/anger
Reduced desire
Anorgasmia
Investigate underlying cause
Referral to sexual medicine
Phosphodiesterase Type 5 (PED5) Inhibitors* (e.g. sildenafil)
CBT
Vibrators and sex aids
Education
Vacuum devices
Intraurethral dilators
Penile rings
* Part of the physiological process of erection involves the release of nitric oxide (NO) in vasculature
of the corpus cavernosum as a result of sexual stimulation. NO activates the enzyme guanylate
cyclase which results in increased levels of cyclic guanosine monophosphate (cGMP), leading
to smooth muscle relaxation in blood vessels supplying the corpus cavernosum, resulting in
increased blood flow and an erection.
PDE5 inhibitors inhibit the degradation of cGMP by phosphodiesterase type 5 (PDE5), increasing
bloodflow to the penis during sexual stimulation.
This mode of action means that PDE5 inhibitors are ineffective without sexual stimulation.
Factors affcting female sexual fucntion
Physiology
Neurological (e.g. MS)
Cardiovascular disease
Cancer
Urogenital
Drugs
Hormone
Menopause and sexual dysfunction
Vaginal atrophy
Psychology
Vaginal dryness
Depression/Anxiety
Prior sexual abuse
Previous difficult labour
Alcohol/drug abuse
Partner technique/performance
Poor quality relationship
Lack of privacy
Socio-cultual
Dyspareunia
Reduced sleep
Interpersonal
Loss of libido
Education
Religious/perosnal/family views
Emotional lability
Hot flushes
Ejaculation disorders
Premature ejaculation that consistently occurring either prior to, upon, or immediately after
penetration and before it is desired.
Inhibited ejaculation male orgasmic disorder.
Retrograde ejaculation ejaculation in which semen travels up the urethra towards the bladder
instead of to the outside of the body.
Premature ejaculation
Causes:
Over-excitation
Anxiety
DM
Low Testosterone
Adapted mastabatory technique
Urological problems
Complications:
Insufficient female arousal
Pain and dryness
Frustration/anger
Reduced desire
Anorgasmia
Treatment:
Start/stop technique
Squeeze technique
Refer psychosexual medicine
Personal growth programme
Pelvic floor exercises
Lignocaine gel
Desensitising condom.
Treatment of Infertility
Women trying to conceive Folic acid 0.4mg
Stop smoking, reduce alcohol
Weight loss (women aim for BMI<30)
Anovulation
(NB. Normal Gonadotrophin and Prl levels)
Clomiphene/tamoxifen = anti-oestrogens and stimulate FSH & LH Ovulation in
80%subjects
+/- mid cycle injection hCG
2nd line = Human menopausal gonadotrophin (human=pergonal or synthetic available)
(N.B Hyperstimulation and multiple pregnancy)
Hyperprloactinaemia
Exclude tumour!
Dopamine agonist (e.g. bromocriptine)
Hypogonadotrophic hypogonadism
Pulsatile GnRH injection s/c
Tubal pathology
Surgical intervention, e.g. ‘salpingostomy’ (10-15% success)
Increased risk ectopic pregnancy
IVF
o
o
o
o
o
o
o
Extracorporeal fertilization
Zygote implanted into uterine cavity
Hyperstimulation of ovaries and collection 36hrs after hCG (to mimic LH surge)
Embryos transferred at 4-8 cell stage
2-3 days after fertilization
20% success
2 mximum
Treating males
Biopsy in ?obstruction
Surgical anastomoses
GnRH drugs in hypogonadotrophic hypogonadism
Bromocriptine in hyperprolactinaemia
Microassissted fertilization eg. ICSI
(Intracytoplasmic sperm injection) in vitro fertilization procedure in which a
single sperm injected directly into an egg.
Donor insemination