ventilation renal
advertisement

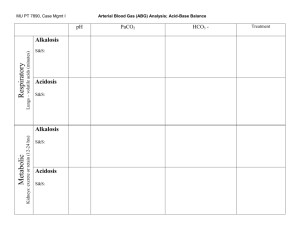
SSN SBPM Workshop~ Exam 4 Multiple Choice Questions **Last year’s handouts are available at http://cpmcnet.columbia.edu/student/ssn/sbpmd/block4.htm For Questions 1-4: Match the changes in volume of the intracellular and extracellular compartments with the associated change. Assume the starting osmolarity of both compartments is 290 mOsm/L. 1. 2. 3. 4. Diarrhea Profuse sweating Saline infusion High Salt Diet A) Decreased extracellular volume, no change in intracellular volume, and no change in osmolarity. B) Increased extracellular volume, decreased intracellular volume, and increased osmolarity. C) Increased extracellular volume, no change in intracellular volume, and no change in osmolarity. D) Decreased extracellular volume, decreased intracellular volume, and increased osmolarity. E) Decreased extracellular volume, increased intracellular volume, and decreased osmolarity. 5. A rat is fed a salt diet of 7 g/day for a period of two weeks. During this period his urinary salt excretion is measured. The rat is then switched to a low salt diet (1gm/day). What was the rat’s excretion of sodium likely to be on day 14 just prior to switching to the low salt diet, and then on day 16 two days after switching? A) On day 14 his urinary excretion is 5 g/day (positive salt balance), and on day 16 it will be approximately 1 g/day (salt equilibrium). B) On day 14 it was 7.0 g/day (salt equilibrium) and on day 16 it will be 1g/day (salt equilibrium). C) On day 14 it was 7.0 g/day (salt equilibrium) and on day 16 it will be reduced but greater than 1.0g/day (negative salt balance). D) On day 14 it was 7.0 g/day, but it is impossible to say where his salt excretion will be on day 16. E) None of the above. 6. Switching to the low salt diet caused a series of neurohormonal changes in the rat that were induced by the decrease in the extracellular fluid osmolarity. What answer choice best describes those changes? I. Increased sympathetic activity II. Increased ANP secretion III. Activation of the renin-angiotensin-aldosterone system IV. Change in starling forces to increase Na+ reabsorption in the proximal tubule A) B) C) D) 7. The effects of ADH on the Kidney include which of the following: I. Insertion of aquaporins in the outer medullary collecting ducts. II. Increased activity of the Na+/K+/2Cl- transporter in the thick ascending limb. III. Increased reabsorption of sodium in exchange for hydrogen in the proximal tubule. IV. Increased urea recycling. A) B) C) D) E) 8. I only I, III, IV only All of the above None of the above I only I and II only I, II and III only I, II and IV only All of the above Which one of the following will DECREASE in a person with V/Q abnormalities? A) Arterial pH B) Arterial carbon dioxide tension C) Alveolar-arterial (A-a) gradient for oxygen D) Alveolar ventilation 9. Which one of the following is higher at the apex of the lung than at the base when a person is standing? A) V/Q ratio B) Blood flow C) Ventilation D) PaCO2 E) Lung compliance 10. An increase in pulmonary blood flow during exercise A) Causes alveolar oxygen tension to decrease B) Causes the V/Q ratio at the top of the lung to increase C) Causes pulmonary arterial resistance to decrease D) Causes diffusion capacity to decrease E) Causes arterial oxygen saturation to decrease 11. Emphysema is associated with loss of elastic fibers in the lungs, leading to increased lung compliance. As a result, the FRC… A) Increases B) Decreases C) Stays the same For questions 12-16: You are given the following data for a patient breathing room air (FIO2 = 21%). Assume Patm = 760 mm Hg, PH2O = 47 mm Hg, and R = 0.8. Tidal volume Dead space volume Breathing frequency PaCO2 12. The patient’s alveolar oxygen tension PaO2 is approximately A) B) C) D) E) 13. 70 mm Hg 80 mm Hg 90 mm Hg 100 mm Hg 110 mm Hg The patient’s minute ventilation is A) B) C) D) E) 14. = 400 mL = 100 mL = 10 breaths/min = 50 mm Hg 3 L/min 4 L/min 5 L/min 6 L/min 7 L/min The patient’s alveolar ventilation is A) B) C) D) E) 3 L/min 4 L/min 5 L/min 6 L/min 7 L/min 15. If the patient doubles her alveolar ventilation without changing her CO2 production, then her PaCO2 will be approximately A) B) C) D) E) 15 mm Hg 20 mm Hg 25 mm Hg 35 mm Hg 40 mm Hg 16. If the patient doubles her tidal volume without changing her CO2 production, then her PaCO2 will be approximately A) B) C) D) E) 15 mm Hg 20 mm Hg 25 mm Hg 35 mm Hg 40 mm Hg 17. A women with a history of alcoholism presents to the ER complaining of blurred vision, dizziness and vomiting after having drank a bottle of what she assumed was EtOH. She is very tachypneic (breathing quickly)and has an increased serum anion gap (this means that she has an increased concentration of some anion besides chloride and bicarbonate in her blood). Which of the following pCO2/pH combinations would be most likely in her case? A) pCO2 30, pH 7.50 B) pCO2 30, pH 7.32 C) pCO2 50, pH 7.50 D) pCO2 50, pH 7.32 18. Which of the following can be measured by spirometry? A) FRC B) RV C) FVC D) TLC E) All of the above F) None of the above 19. Which of the following is/are true? I. A stroke in the dorsal medulla might require ventilatory support. II. An infarction of the apneustic center might require ventilatory support. III. Central chemoreceptors are most sensitive to changes in blood pH. IV. It is physiologically possible to have a negative alveolar-arterial gradient (eg higher pO2 in the blood as compared to the alveolus). A) I, II, III, IV B) I, III C) I only D) I, III, IV E) I, IV 20. A patient has an arterial blood gas shown below. Normal values in parentheses. pH = 7.29 (7.40) pCO2 = 70 mmHG (40 mmHg) [HCO3-] = 33 meq / L (24 meq / L) The patient’s acid-base status can best be described as: A) B) C) D) Respiratory Acidosis. Respiratory Alkalosis. Metabolic Acidosis. Metabolic Alkalosis 21. A patient takes an unusually large amount of aspirin (acetylsalicylic acid.) Which of the following statements about the patient is false? A) The patient’s acid-base status is best described as metabolic acidosis. B) The patient is excreting H+ bound to HPO42-, which is coupled to the new reabsorbtion of HCO3-. C) The patient reabsorbs filtered HCO3- in the proximal tubule, which is coupled to H+ excretion. E) The patient is excreting NH4 in the urine in a process involving the proximal tubules, thick ascending loop of henle, and the collecting duct. 22. A freely filterable substance that is neither secreted nor reabsorbed has a renal artery concentration of 15 mg/ml and a renal vein concentration of 5 mg/ml. What is the filtration fraction? A) B) C) D) 0.25 0.33 0.5 0.67 23. Both GFR and renal blood flow will increase if A) The efferent and afferent arterioles both dilate to the same degree B) The afferent constricts and the efferent dilates to the same degree C) The efferent and afferent arterioles both constrict to the same degree D) Only the efferent arteriole constricts SSN SBPM Workshop~ Exam 4 Answers to Multiple Choice Questions 1. A Diarrhea can be considered to be loss of isosmotic fluid from the extracellular space. As a result, there will be a decrease in extracellular volume, but because there is no change in osmolarity there will be no compensatory volume change in the intracellular compartment to offset the loss. 2. D Sweating can be considered loss of a hyposmotic fluid from the extracellular space. As a result, the osmolarity of the ECF will become transiently hyperosmotic (more concentrated) to the intracellular fluid. This results in water flow from the ICF to the ECF. The net change is to reduce the volume of both spaces, and to increase the osmolarity. 3. C Isosmotic infusion of fluid into the ECF. No change in osmolarity or fluid shifts result. 4. B Increased sodium in the ECF results in water flows into the ECF from the ICF. The net result is increased ECF volume, decreased ICF volume, and an increase in the overall osmolarity. 5. C The rat is at equilibrium after two weeks on the high salt diet. Switching to the low salt diet requires several days for the adjustment in neurohormonal activation to take place and for his urinary excretion to decrease to 1.0 g/day. During this period of adjustment, the rat is said to be in negative salt balance (excreting more than he can taken in). 6. B ANP is secreted in response to an increase in ECFV. Switching to a low salt diet would tend to cause a decrease in the ECF and thus decrease ANP secretion. 7. D Reabsorption of Na+ in the proximal tubule depends on angiotensin not ADH. ADH has all of the other effects listed. 8. B V/Q mismatches will cause arterial oxygen levels (Pao2) to decrease. Decreased Pao2 will stimulate the chemoreceptors which, in turn, will increase alveolar ventilation and decrease PaCO2. The decreased PaCO2 will cause respiratory alkalosis (increasing pH). The fall in PaO2 causes the A-a gradient to rise. 9. A The alveoli at the apex of the lung are larger than those at the base so their compliance is less. Because the compliance is reduced, less inspired gas goes to the apex than to the base. Also, because the apex is above the heart, less blood flows through the apex than through the base. However, the reduction in airflow is less than the reduction in blood flow, so that the V/Q ratio at the top of the lung is greater than it is at the bottom. The increased V/Q ratio at the apex makes PaCO2 lower and PaO2 higher at the apex than they are at the base. 10. C The increase in blood flow through the pulmonary circulation during exercise increases the diameter of the pulmonary vessels and therefore decreases their resistance. The increased blood flow to the lungs evens out the V/Q ratio, decreasing it at the top of the lung and increasing it at the bottom. Making the V/Q ratio more similar throughout the lung may decrease some of the shunting effect that normally occurs at the base where the V/Q ratio is quite low and may actually increase the O2 saturation of arterial blood. The increased blood flow will also increase the surface area for respiratory exchange and therefore increase the diffusing capacity. 11. A As a result of the increase in compliance, the collapsing (elastic recoil) force on the lungs is decreased at a given volume. At the original value for FRC, the tendency of the lungs to collapse is less than the tendency of the chest wall to expand, and these opposing forces will no longer be balanced. In order for the opposing forces to be balanced, volume must be added to the lungs to increase their collapsing force. Thus, the combined lung and chest-wall system seeks a new higher FRC, where the two opposing forces can be balanced; the new intersection point, where airway pressure is zero, is increased. 12. C Use the alveolar gas equation: PAO2 = FIO2 (Patm – PH2O) – (PACO2/R) = .21 (760 mm Hg – 47 mm Hg) – (50 mm Hg/0.8) = 149.75 mm Hg – 62.5 mm Hg = 87.5 mm Hg ~ 90 mm Hg 13. B Minute ventilation is equal to tidal volume VT times breathing frequency f, so Minute ventilation = VT × f = 0.4 L × 10 breaths/min = 4 L/min 14. A Alveolar ventilation is minute ventilation corrected for the physiologic dead space VD, so Alveolar ventilation = (VT – VD) × f = (0.4 L – 0.1 L) × 10 breaths/min = 3 L/min 15. C PaCO2 is inversely proportional to alveolar ventilation, so doubling the latter would halve the former, which would decrease from 50 mm Hg to 25 mm Hg. 16. B Again, PaCO2 is inversely proportional to alveolar ventilation, so: PaCO2 × alveolar ventilation = constant If the patient doubles her tidal volume to 800 mL (0.8 L), her alveolar ventilation will increase from 3 L/min to: Alveolar ventilation = (0.8 L – 0.1 L) × 10 breaths/min = 7 L/min Thus, because PaCO2 × alveolar ventilation = constant, we get: 50 mm Hg × 3 L / min = PaCO2 × 7 L /min PaCO2 = 21 mm Hg ~ 20 mm Hg 17. B This woman has methanol poisoning, which leads to severe metabolic acidosis. As pH decreases, the compensatory respiratory response is to blow off CO2 by hyperventilating (remember that alveolar ventilation is inversely proportional to PaCO2; also, peripheral chemoreceptors are going to be involved here because the problem is NOT increased PaCO2). For those who are interested, the treatment for methanol poisoning is to administer ethanol, which competes with MeOH for access to alcohol dehydrogenase. Choice A would be a situation of respiratory alkalosis, choice C would be metabolic alkalosis and choice D would be respiratory acidosis (try to think of clinical scenarios that would lead to each of these conditions). 18. C This is mostly just to familiarize you with the multiple abbreviations having to do with capacities and volumes and to reiterate that you CANNOT measure residual volume (a component of FRC and TLC) by spirometry. You can measure the forced vital capacity. 19. C The dorsal respiratory area in the medulla is needed for spontaneous inspiration without cortical control (central hypoventilatory syndrome). The apneustic center in the pons is not necessary for respiration. The central chemoreceptors do not directly see decreased blood pH; they are sensitive to changes in CSF pH. The last one is kind of tricky, but in general, if you see a negative A-a gradient, it probably means that some room air contaminated the blood sample to increase the PaO2. 20. A. The pH is low, therefore the patient is acidotic. The high PCO2 suggests a respiratory cause. A low pCO2 would suggest a metabolic cause. The high HCO3- suggests that the condition is chronic. 21. C It is false because HCO3-reabsorbtion isn’t associated with H+ excretion. [Note: H+ excretion is associated with new HCO3- reabsorbtion.] 22. D (FF = GFR/RBF = 10/15) 23. A SSN SBPM Workshop~ Exam 4 Short Answer Questions Note: These questions may not be similar to the on-line short answer questions for your exam. The purpose of these questions is to explain topics in more detail than is allowed by the Multiplechoice format. Also, these questions offer an opportunity to go over some topics that the SSN teachers do not have time to teach during the SSN session. 1. How does the kidney produce concentrated urine? Dilute urine? The production of concentrated urine depends on the presence of ADH, and of a concentration gradient within the medulla (maintained by the countercurrent multiplier and urea recycling). 1. Osmolarity of glomerular filtrate equals that of the blood (300 mOsm/L). 2. There is no change in osmolarity in the proximal tubule as water and salt are reabsorbed in proportion. 3. In the thick ascending limb of the loop of Henle the Na+/K+/2Cl- cotransporter reabsorbs NaCl from the lumen. These cells are impermeable to water, however, and the resulting fluid is diluted significantly (100mOsm/L). It is this co-transporter that is responsible for establishing the concentration gradient in the medulla (countercurrent multiplier). 4. In the early distal tubule the process continues with the reabsorption of salt by the Na/Cl co-transporter. This leads to further dilution of the fluid as the cells are still impermeable to water. 5. In the late distal tubule, the cells are now permeable to water in the presence of ADH (aquaporins). As a result, water flows down its gradient until it is isosmotic with the surrounding fluid (300mOsm/L again). 6. In the collecting ducts, the cells are again permeable to water in the presence of ADH. Fluid therefore flows out of the lumen and into the interstitium as it moves down the tubule through the medulla in the collecting duct (interstitial osmolarity is increasing in the inner medulla). As a result, it will equilibrate until it reaches a concentration equal to that of the surrounding environment (as much as 1200 mOsm/L). The production of dilute urine is much simpler. Without ADH present, water cannot be reabsorbed in the distal tubule or collecting duct. As a result, there is no opportunity to concentrate the urine as it flows down through the medulla. The result is a dilute Urine that may be as low as 75mOsm/L (even lower than the 100 mOsm/L in the early distal tubule due to further reabsorption of sodium in the late distal tubule and collecting duct). 2. The diagram below represents a spirometry tracing illustrating the changes in lung volume that occurred when a subject inhaled maximally and then rapidly exhaled as much gas as possible. If the patient’s total lung capacity is 6 L, calculate the following: A) FRC B) FEV1 C) Inspiratory capacity D) Inspiratory reserve volume E) Expiratory reserve volume a) FRC = 3 L. Functional residual capacity (FRC) is the volume of gas in the lung at the end of a normal expiration, when the muscles of inspiration and expiration are relaxed. At FRC, the elastic forces acting on the lungs are in equilibrium; that is, the tendency of the lungs to collapse is balanced by the tendency of the chest to expand. When the volume is at FRC, the spirometry trace reads 1 L; note from the trace that FRC is 3 liters less than total lung capacity. Therefore, FRC is 6 L – 3 L = 3 L. b) FEV1 = 3.5 L. The FEV1 is the amount of gas that can be expelled from the lungs in 1 s during a forced expiration from total lung capacity. Based on the tracing, FEV1 = 3.5 L (go from 4 L to 0.5 L in the first second of the forced expiration maneuver). c) Inspiratory capacity = 3 L. The inspiratory capacity is the maximum amount of gas than can be inhaled when the subject starts from FRC. In this subject, the inspiratory capacity is 3 L. d) Inspiratory reserve volume = 2.5 L. The inspiratory reserve volume is the maximum amount of gas that can be inhaled when the subject starts at the end of a normal inspiration. e) Expiratory reserve volume = 1 L. The expiratory reserve volume is the maximum amount of gas that can be exhaled when the subject starts from FRC. 3. A man comes to the ER complaining of difficulty breathing. His vitals are as follows: Pulse 90/min, Resp. rate 24 and BP 140/90. A blood gas is drawn and the following values are seen: pCO2 34 mmHg, pO2 54 mmHg. He is given 100% oxygen by nasal cannula at 6 L/min. When his blood gases are taken one hour later, they are as follows: pCO2 45 mmHg, pO2 85 mmHg. Describe a plausible mechanism to explain the increase in pCO2 (hint: think about breathing control mechanisms). One likely explanation is that originally, his rapid respiratory rate (nb: 24 breaths/min is rapid) was being driven by his low pO2 (hypoxemic peripheral drive). His pCO2 is low, becauseof his hyperventilation, so his central receptors are not driving respiration. After oxygenating him, his pO2 rises and, since his pCO2 is still low, his hypoxemic hyperventilation would resolve. This would cause his pCO2 to rise. 4. Fill in the chart below with “up” or “down” reflecting the appropriate changes. pH pCO2 HCO3-Respitory Acidosis Respitory Alkalosis Metabolic Acidosis Metabolic Alkalosis Respraitory Acidosis Respiratory Alkalosis Metabolic Acidosis Metabolic Alkalosis pH down up down up pCO2 up down down up HCO3up (more chronic than acute) down more chronic than acute) down up 5. The pKa of H2CO3 is 6.1 and the pKa of H2PO4- is 6.8. Based solely upon their pKa, which is the better buffer? Why? In the human body, which is the better buffer? Why? Based on pKa alone, H2PO4- is the better buffer because it’s pKa is closest to physiologic pH (7.4). That allows the steepest part of it’s titration curve to fall closer to physiologic pH. However, in the human body H2CO3 is the better buffer because it is present in a much higher concentration; also, because of carbonic anhydrase, the acid form of CO2 can be blown off by respiration. 6. How does the rate of glomerular plasma flow relate to the rate of glomerular filtration? The greater the glomerular blood flow, the greater the rate of glomerular filtration. The faster the plasma flows along the glomerular capillary, the less the oncotic pressure of the plasma in the glomerular capillary increases. Thus the pressure of ultrafiltration is greater, and the conditions for filtration are more favorable. 7. How does Angiotensin II affect the GFR? Angiotensin II constricts the efferent arteriole. This will increase the hydrostatic pressure in the glomerular capillary, which increases the GFR.