role of the lungs in drug distribution
advertisement

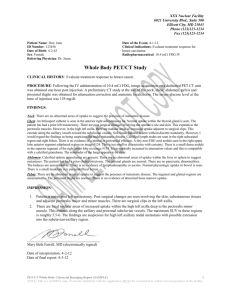
http://www.euroanesthesia.org/education/rc_amsterdam/09rc4.HTM The role of the lungs in drug distribution • 9 RC 4 Fred BOER MD PhD Leiden University Medical Centre Leiden, The Netherlands Monday 31 May 1999 Amsterdam The lungs are not usually considered important in the fate of drugs in the body since they contribute little to total body mass and usually have a small metabolic capacity. Because of their strategic location between the site of injection and the site of action, however, they can significantly influence drug concentrations immediately after acute drug injection. This is particularly true for basic amines, which includes many drugs used in anaesthesia, since first-pass lung uptake is large for these agents. First-pass lung uptake reduces arterial concentrations immediately after injection, and limits the amount of drug available for distribution to the effect site. Educational goals ________________________________________ To review the effects the lungs have on blood concentrations immediately after injection and during the mixing period; to discuss how these effects can be modelled, and explain the importance of uptake of drugs in the lungs; to review those drugs that are retained in the lungs; and discuss how lung uptake can be studied and how drug uptake in the lungs can be incorporated in pharmacological models. The mixing period ________________________________________ It is often thought that blood concentrations are highest immediately after intravenous injection of a drug. It is obvious that at some place in the body, near the site of injection, concentration must be high, but in the arterial circulation the drug concentration will be zero during the first seconds after injection. The speed with which the concentration will increase will depend on the cardiac output, the amount of blood between the site of injection and the arterial point where the concentration is measured and on the uptake of the drug into the lungs. Even in patients with a high cardiac output, central injection of the drug and no lung uptake, the drug concentration will increase over several seconds to a maximum, then decrease to a first minimum and again rise to a much smaller second peak (fig.1, open square symbols). After this, the concentration will follow the well-known course of the multi-exponential decay curve. This first period of rapid peaks and troughs of drug concentration is known as the mixing period. The effects of mixing are observed during seconds to minutes after drug injection. How important is this to the care of patients and how will an understanding of the phenomena affect patient treatment ? Mixing phenomena are most important in those patients in whom the mixing is least, resulting in prolonged high concentrations of anaesthetics, such as patients with a poor cardiac output, where greater drug concentration can lead to a more pronounced cardiac depression or other haemodynamic side effectss Better understanding of drug mixing could lead to an adaptation in the dosing of drugs, especially in those patients in whom a poor mixing is anticipated. The mixing period is affected by the blood volume of the central part of the circulation (the intrathoracic or central blood volume), the cardiac output, the distribution of the cardiac output in the lungs and peripheral tissues and lung uptake of drug. Several combinations of factors can lead to concentrations either greater or smaller than normal during the mixing period. In general a low cardiac output will be associated with large initial concentrations which will be maintained for longer (see fig.1). If the drug undergoes significant firstpass uptake this will reduce initial concentrations. On the other hand if the lung uptake is decreased (by competitive interaction by other drugs), the concentrations immediately after injection will be increased. Apparently the lungs can play an important role during the mixing period. Figure 1. The concentration-time curves after identical doses of indocyanine green (ICG) given during high cardiac output (dashed line) and during normal cardiac output (grey line) in a sheep. The concentration-time curve of propofol (black line), given simultaneously with ICG during normal cardiac output was corrected for differences in dose. The differences in the ICG and propofol concentrations are explained by lung uptake. Lung uptake ________________________________________ The lungs are important sites for uptake and metabolism of endogenous compounds, such as hormones and prostaglandins [1,2]. Many drugs used in anaesthesia are also bound to the lungs (table 1) [3]. Usually the binding is temporary, and drug is released from the lungs when pulmonary arterial concentrations decrease. Metabolism in the lungs is rare and is usually seen only for endogenous substances which are used therapeutically, such as n oradrenaline and dopamine. Table 1. Pulmonary uptake of drugs used in anaesthesia and other drugs ________________________________________ drug group pulmonary uptake local anaesthetics: ropivacaine bupivacaine, low - moderate mepivacaine, lidocaine induction agents: thiopentone, propofol low - high muscle relaxants: curare, pancuronium, none atracurium, rocuronium opioids: morphine, alfentanil, pethidine, moderate - high sufentanil, fentanyl vasoactive drugs: noradrenaline, dopamine moderate non-anaesthetic drugs: imipramine, chlorpromazine, quinidine, quinine, verapamil, propranolol, nitrofurantoin, captopril There may be significant competition for binding sites in the lungs. Lung uptake of fentanyl may be significantly less if the patient takes propranolol preoperatively [4]. Fentanyl on the other hand can under certain circumstances decrease the pulmonary uptake of propofol [5]. The uptake of imipramine is decreased by the anti-depressant clomipramine [6]. If there is competition for drug uptake in the lungs, this may cause significantly greater arterial concentrations immediately after injection. Drugs undergoing the highest pulmonary uptake share some characteristics: they are all highly lipophilic, basic and often amines. The pulmonary uptake for neutral and acidic drugs is usually limited, although for some of these drugs pulmonary uptake may be significant (e.g. propofol). Some speculate that the affinity of basic amines for lung tissue is caused by their affinity for lysosomes, where they are trapped by ionization in the acidic environment of the lysosome [7]. In addition, drugs can be bound to tissue elements, to proteins, or diffuse into lipid structures. Studies of accumulation and release of drugs in isolated lung models show that there are several depots in the lungs to which drugs bind, with different affinities and binding capacities [8]. Lung uptake has been studied both in vitro and in vivo. In vitro methods often involve the use of isolated lung models, in which the lungs of animals are included in a (re-circulatory) perfusion system. The isolated lung model has been used extensively and has greatly added to the understanding of lung uptake [9]. The results of these studies, however, should be extrapolated with caution to man, because important differences in lung uptake may exist between species. In vivo lung uptake can be studied by an indicator dilution method, in which the first-pass retention is calculated by comparison of the drug concentration curve to that of an indicator not undergoing pulmonary uptake. Clearly the double indicator dilution method is limited to the firstpass period. The period beyond first-pass can be studied by mass balance methods, compartmental analysis, system dynamics and recirculatory modelling. Most of these methods, except recirculatory modelling, require measurement of both arterial and pulmonary arterial concentrations, which limits their applicability. Modelling lung uptake ________________________________________ The mixing period, although highly relevant to anaesthesiologists, is poorly described by the compartmental models commonly used in research, and also used for controlling infusion pumps, such as the Diprifusor. Because lung uptake can have an important influence on the concentrations immediately after injection, it would be relevant to try to incorporate this phenomenon in pharmacological modelling. Lung uptake is difficult to incorporate into the compartmental models, since these models assume immediate and complete mixing. Moreover, in most studies of drug kinetics using compartmental models, sampling commences only after 1-2 minutes after injection, that is after the period of initial mixing. The concentration at time zero on which the calculation of some pharmacokinetic parameters is based is therefore not an observed concentration. The concentration is obtained by back-extrapolation to zero of the concentration-time relationship and is thus a calculated value. This leads to discrepancies with the actual concentrations immediately after injection and will affect in particular the calculated size of the central volume of distribution. Although speculative, it is likely that significant lung uptake will further affect the size of both the central volume of distribution of the drug and, to a lesser extend, the volume of the peripheral compartment (V2). If both arterial and pulmonary arterial samples are available, lung uptake may be modelled using a physiological model [10] or by system analysis [11]. These models can predict the arterial concentrations if pulmonary arterial concentrations are known, and provide information on the distribution volume in the lungs. However these models have not been integrated, into a complete model of the body and thus are of limited value to the clinician. Integrated modelling of pulmonary uptake is possible with physiological models and recirculatory models. Physiological models are frequently used for research in animals. The results may to some extent be scaled up to humans [12], but may have intrinsic weaknesses if the kinetic behaviour of the drug differs between species. Physiological models cannot be fully validated in patients and volunteers, since they need precise information on organ volumes, composition and blood flows. Pulmonary uptake can also be modelled by recirculatory models, together with the other phenomena taking place during the mixing phase [13-15]. The advantages of these models are that they describe lung uptake beyond the period of first-pass, that the mixing period can be fully modelled, and that only arterial samples are required. Using this model for the study of alfentanil in pigs, we estimated the pulmonary volume of distribution of alfentanil, which agreed with the volumes found with compartmental modelling and system dynamics analysis in similar pigs [16]. The model used in this study is shown in fig. 2 and is very similar to the models used by Henthorn and coworkers [13,14]. Conclusion ________________________________________ For many drugs used in anaesthesia the lung is a site of first-pass uptake when the drug is given intravenously. A significant first-pass uptake will decrease the arterial concentrations, in particular during the initial mixing period. This effect of lung uptake, together with effects of blood volume and cardiac output on the initial concentrations immediately after injection are not predicted by compartmental models. Physiological models and in particular recirculatory models are better capable of predicting the course of the concentrations in the mixing period. References ________________________________________ 1. Bend J, Serabjet-Singh C, Philpot RM. The pulmonary uptake, accumulation, and metabolism of xenobiotics. American Review of Pharmacology and Toxicology 1985;25:97-125. 2. Ryan US, Grantham CJ. Metabolism of endogenous and xenobiotic substances by pulmonary vascular endothelial cells. Pharmacology and Therapeutics 1989;42: 235-250. 3. Roerig DL, Ahlf SB, Dawson CA, Linehan JH, Kampine JP. First pass uptake in the human lung of drugs used during anaesthesia. Advances in Pharmacology 1994;31: 531-549. 4. Roerig DL, Kotrly KJ, Ahlf SB, Dawson CA, Kampine JP. Effect of propranolol on first pass uptake of fentanyl in the human and rat lung. Anesthesiology 1989;71: 62-68. 5. Matot I, Neely CF, Katz RY, Marshall BE. Fentanyl and propofol uptake by the lung: effect of time between injections. Acta Anaesthesiologica Scandinavica. 1994;38: 711-715. 6. Suhara T, Sudo Y, Yoshida K, et al. Lung as reservoir for antidepressants in pharmacokinetic drug interactions. Lancet 1998;351: 332-335. 7. MacIntyre AC, Cutler DJ. The potential role of lysosomes in tissue distribution of weak bases. Biopharmaceutics and Drug Disposition 1988;9: 513-526. 8. Philpot RM, Anderson MW, Eling TE. Uptake, accumulation, and metabolism of chemicals in the lung. In: Metabolic functions of the lungs. Bahkle YS, Vane JR. eds. Marcel Dekker, New York, 1977;123171. 9. Bend JR. Isolated perfused lungs in drug disposition studies. In: Topics in Pharmaceutical Sciences 1987. Breimer DD, Speiser P. eds. Elseviers Science Publishers, Amsterdam, 1987;235-246. 10. Boer F, Olofsen E, Bovill JG, Burm AGL, Hak A, Geerts M. Pulmonary uptake of sufentanil during and after constant rate infusion. British Journal of Anaesthesia 1996;76: 203-208. 11. Boer F, Hoeft A, Scholz M, Burm AGL, Bovill JG, Hak A. Pulmonary distribution of alfentanil and sufentanil studied with system dynamics analysis. Journal of Pharmacokinetics & Biopharmaceutics 1996; 24: 197-218. 12. Bjorkman S, Wada DR, Stanski DR, Ebling WF. Comparative physiological pharmacokinetics of fentanyl and alfentanil in rats and humans based on parametric single-tissue models. Journal of Pharmacokinetics & Biopharmaceutics 1994;22:381-410. 13. Krejcie TC, Avram MJ, Gentry WB, Niemann CU, Janowski MP, Henthorn TK. A recirculatory model of the pulmonary uptake and pharmacokinetics of lidocaine based on analysis of arterial and mixed venous data from dogs. Journal of Pharmacokinetics & Biopharmaceutics 1997;25: 169-190. 14. Krejcie TC, Henthorn TK, Shanks CA, Avram MJ. A recirculatory pharmacokinetic model describing the circulatory mixing, tissue distribution and elimination of antipyrine in dogs. Journal of Pharmacology and Experimental Therapeutics 1994;269: 609-616. 15. Henthorn TK, Avram MJ, Krejcie TC, Shanks CA, Asada A, Kaczynski DA. Minimal compartmental model of circulatory mixing of indocyanine green. American Journal of Physiology 1992;262: H903-H910. 16. Kuipers, JA, Boer F, Olofsen E, Oliemans W, Bovill JG, Burm, A G L. Recirculatory and compartmental pharmacokinetics of alfentanil in pigs: the influence of cardiac output. Anesthesiology, accepted for publication.