Outpatient Referral Form - King Edward Memorial Hospital for Women
advertisement

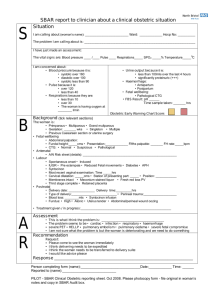
REQUEST for OUTPATIENT APPOINTMENT to King Edward Memorial Hospital Please make an appointment for this patient to attend: (please check) Obstetric Gynaecology Diagnostic Imaging/Ultrasound Only Menopause Fertility CVS/Amniocentesis only Oncology Genetic Other: Next of Kin/Guardian: Family name: Relationship: Family name: First Name (s): Has the patient previously been seen by this hospital? Maiden Name: Retained: First Name: Yes Yes No No Name Registered: Year of last attendance: Is an interpreter required? Address: Yes No If yes, language / dialect: Telephone No.: Home: Work: Postcode: Mobile Birth Date: / / Marital Status: Age: BMI (required for all referrals): M W D If BMI unknown, please include: weight (kg): Sep Defacto height (m): Country of Birth: Medicare Number.: Ref: S Expiry: Referring doctor stamp and signature (compulsory for Diagnostic Imaging requests) Name: Phone: Address: If other than Obstetric Patient PTO If Obstetric Patient: We would like to share antenatal care with you, both before and after the first clinic visit (usually at 19 weeks). I do not wish to be involved in shared care Gravida: Parity: LMP: EDD (by dates): EDD (by ultrasound) Please forward photocopies or arrange copies to be sent to KEMH of results of tests listed below. Check () beside the test if you have, or will, arrange the test. Full Blood Picture Pap (within 2 years) Group and atypical antibodies Midstream Sterile Urine Early dating ultrasound (if dates uncertain) HIV Rubella antibodies Hep B surface antigen Syphilis antibodies Fetal anatomy U/S (18 to 20 weeks) Chlamydia Glucose tolerance test routine at 24-28 weeks To be done at 1st visit to GP if high risk for GDM Hep C antibodies 1st trimester screen (11 to 13 weeks) or Other: maternal serum screening (15 to 17 weeks) Indicate specialist service/s that you believe need to see this patient at KEMH before 19 weeks, please state reason over page. Adolescent Ultrasound Drug and Alcohol Diabetes Dietician Genetic Medical Social Work Psychological Medicine Maternal Fetal Medicine (if high risk ) Other – Please specify D:\106754436.doc Referral Letter Please return this form to: King Edward Memorial Hospital, 374 Bagot Road, Subiaco WA 6008 or by fax to: 9340 1031 Please note: your patient may be referred to a health service closer to home if they do not require tertiary care. D:\106754436.doc


![Jiye Jin-2014[1].3.17](http://s2.studylib.net/store/data/005485437_1-38483f116d2f44a767f9ba4fa894c894-300x300.png)