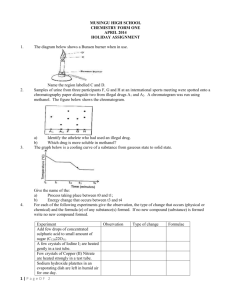
stearate prescription
advertisement

Ajman University of Science & Technology Faculty Of Pharmacy & Health Sciences .…………………. LABORATORY MANUAL FOR DOSAGE FORMS-II Central Committee Department of Pharmaceutics ………………….. 2000 - 2001 1 Dear Students, The central committee of department of pharmaceutics, Faculty of Pharmacy and Health Sciences, is pleased to introduce to you the Laboratory Manual of Dosage Forms II (700214). The manual covers experiments deal with the principles discussed in didactic lectures. These experiments employ fundamental principles of pharmaceutics required to design and prepare physically and chemically stable dosage forms and be acquainted with official quality assurance methods that ensure their therapeutic safety and efficacy. The central committee set this manual for all the branches to ensure the uniformity of student outcome. Best Regards Central Committee Department of pharmaceutics, Faculty of Pharmacy and Health Sciences 2 Table of Content PART No. PART 1 Exp.(1) Exp.(2) Exp. (3) PART 2 Exp.(4) Exp.(5) Exp.(6) Content EMULSIONS Preparation of Emulsion Using Hydrophilic Colloids as Emulsifying Agent Acacia Emulsion Preparation of Emulsions Using Finely Divided Particles as Emulsifying Agent Calamine Lotion B.P. Preparation of Emulsion using Anionic Surfactant White Liniment Vanishing Cream Preparation of Emulsion using Non-Ionic Surfactant OINTMENTS Preparation of Simple Ointment Preparation of Macrogol Ointment Preparation of Absorption Base Ointment Preparation of Emulsifying Wax Evaluation of Drug Release from Ointment Base Ophthalmic Preparations Introduction to Pharmaceutical Calculation Exp.(7) Preparation of Isotonic Buffer Solution Exp.(8) Compounding of Ophthalmic Liquids Buffers and buffer capacity Isotonicity and sterility Exp.(9) Isotonicity and pH adjustment PART 4 STERILE PREPARATIONS Exp.(10) IV Admixture Demonstration of TPN Preparation APPENDIX Guidelines, Equipment, and Supplies for Sterile Compounding Page No. 5 11 13 14 16 31 32 34 PART 3 3 38 43 48 56 58 59 75-118 PART 1 EMULSIONS 4 Introduction : Emulsification is the process of preparing emulsions, which are heterogeneous systems consisting of at least one immiscible liquid intimately dispersed in another in the form of droplets, whose diameters generally exceed 0.1µ. Emulsions are also defined as thermodynamically unstable mixtures of two essentially immiscible liquids and are characterized by a third phase, an emulsifying agent. The extemporaneous preparation of an emulsion depends on a number of considerations by the pharmacist. These include the purpose of the drug, internal or external use, concentration of the active drug, liquid vehicle, physicochemical stability of the drug, preservation, buffers, solubilizers, emulsifying agents, viscosity enhancers, colors and flavors. Definitions and Characteristics : In emulsions, one phase is dispersed throughout the second phase as "globules". An emulsion consists, then, of a dispersed phase (internal phase, discontinuous phase), a dispersion medium (external phase, continuous phase) and a third component known as an emulsifying agent. There are different types of emulsifying agents as will be discussed later. The diameter of the dispersed phase globules is generally in the range of about 0.1 to 10µ, though some as small as 0.01µ and as large as 100µ are not uncommon. Emulsions are used when two immiscible liquids must be dispensed in the same preparation for some designated reason. Ordinarily, this means there is a polar and a non polar component, each of which is a liquid. When the dispersed phase is non polar (oil) and the external phase is polar (water), the emulsion is known as an oilin-water emulsion. When the dispersed phase is water and the dispersion medium is oil, the emulsion is of the water-in-oil kind. Ordinarily, but not always, emulsions for internal use are of the oil-in-water type and emulsions for external use are of either type. Water-in-oil emulsions are insoluble in water, not water-washable, will absorb water, are occlusive, and may be "greasy". Oil-in-water emulsions are miscible with water, are water washable, will absorb water, are non occlusive, and are non greasy. 5 Uses and Applications Emulsions are widely used in the form of topical creams and lotions. Creams are opaque, soft solids or thick liquids intended for external application, consisting of medicaments dissolved or suspended in water removable (vanishing cream) or emollient bases. They are of the water-in-oil or oil-in-water type. The term "cream" is most frequently applied to soft, o/w, cosmetically acceptable types of preparations. These usually are applied to moist, weeping lesions as they have somewhat of a "drying" effect in that the fluids will be miscible with the aqueous external phase of the creams. Lotions are fluid emulsions or suspensions for external application. They generally are applied to intertriginous areas, i.e., where skin rubbing occurs as between fingers, thighs, under the arms, etc., as they have a lubricating effect. Emulsions are used internally to dispense oil and water drugs together, mask the taste of poorly tasting oily drugs and sometimes to enhance the absorption of selected drugs. Intravenously-administered emulsions are widely used to administer high calorie oil to severely debilitated patients. Composition Generally, emulsions contain three components: a lipid phase, an aqueous phase and the emulsifier. Of these, the compounding pharmacist generally has greatest flexibility in the choice of the emulsifier. The purpose of an emulsifying agent is to minimize the tendency of the globules to coalesce, or join together to form larger globules, with eventual separation of the two liquids. The stability of an emulsion is dependent upon the properties of the emulsifier and the film it forms at the interface between the two phases. The film at the interface must be both tough and elastic and should be rapidly formed during the preparation, or emulsification, process. Emulsifying agents can be divided into three different categories: 1. Surface-active agents 2. Hydrophilic colloids 3. Finely divided solid particles Surface-active agents are adsorbed at oil: water interfaces to form monomolecular films, resulting in a decrease in interfacial tension. Hydrophilic colloids form multimolecular films about the dispersed particles. Finely divided solid particles are adsorbed at the interface between the two liquid phases of the globules and form a film of particles around the dispersed globules. Common to each of these three categories is the formation of a "film" . 6 Emulsifiers that can be used are shown in Table 1. Table 1: Emulsifiers and Stabilizers for Emulsions Carbohydrates Acacia Agar Chondrus Pectin Tragacanth Proteins Casein Egg yolk Gelatin Surfactants Anionic Cationic Nonionic Solids Aluminum hydroxide Bentonite Magnesium hydroxide High Molecular Weight Alcohols Cetyl alcohol Glyceryl monostearate Stearyl alcohol Determination of Type of Emulsions It is important to know whether an emulsion is o/w or w/o in the event additional ingredients must be added. The type of emulsion can be determined by some simple tests, including the drop dilution test, dye solubility test electrical conductivity test, and the filter paper test. The drop dilution test is based on the principle chat an emulsion is miscible with its external phase and is simply performed by dropping a small quantity of the emulsion onto a surface of water. If the drop is miscible with the water, it will spread, indicating that water is the external phase (an o/w emulsion). The dye solubility test is based on the principle chat a dye disperses uniformly throughout an emulsion if it is soluble in the external phase and is conducted by adding a small quantity of a water soluble dye (powder or solution) to the emulsion. If it diffuses uniformly throughout the emulsion, water is the external phase (an o/w emulsion). The electrical conductivity test is based on the principle chat water conducts an electric current while oils do not. Generally, o/w emulsions have a tendency to conduct electricity better than w/o emulsions, if the required equipment is available. The filter paper test involves putting a drop of emulsion onto a clean piece of filter paper. If the drop spreads rapidly into the filter paper, it is an o/w emulsion as water (the external phase) tends to spread more rapidly throughout the filter paper than does oil. Multiple emulsions can be prepared by emulsifying an emulsion to add another external phase. An example would be the combination of a w/o emulsifier 7 (sorbitan mono oleate) with liquid petrolatum, addition to an aqueous phase to form a w/o emulsion, followed by dispersion in an aqueous solution of an o/w emulsifying agent (Tween 80) to form a final w/o/w emulsion. Similarly, an o/w/o emulsion can be prepared. Numerous applications suggested include detoxification, drug targeting/localizabon, prolonged acting dosage forms and potential application in cosmetics. If two immiscible liquids are in contact with each other, they will tend to maintain as small an interface as possible. Consequently, it is very difficult to mix the two liquids. When they are shaken together, spherical droplets will form, as the liquids tend to maintain as small a surface area as possible and an interfacial tension will be maintained between the two liquids. When a "surface-active" ingredient is added, its molecules will tend to be oriented between the two faces with the polar ends in the polar phase and the non polar ends in the non polar phase, which will lower interfacial tension. This will result in miscibility of the two liquids. There are three different general methods whereby emulsifying agents aid in the formation of emulsions. These include: 1. reduction of interfacial tension 2. formation of a rigid interfacial film 3. formation of an electrical double layer If the emulsifier concentration is sufficiently high, a rigid film can be formed between the immiscible phases which can act as a mechanical barrier to coalescence of the globules. An electrical double layer results in repulsive electrical forces between approaching droplets to minimize coalescence. Preparation Methods/Techniques of Emulsions Emulsions do not form spontaneously when liquids are mixed, but rather require energy input to break up the liquids, resulting in an increased surface area of the internal phase. This energy input can be in the form of mechanical agitation, ultrasonic vibration or heat. Emulsions generally can be prepared by manual and mechanical methods. Commonly used techniques involve the use of a mortar and pestle, electric mixer, hand homogenizer , shaking, sonifiers, and beakers. A mortar and pestle can be used with both the English and Continental methods described below. For best results, the mortar should have rough surfaces to aid in shearing the liquid into small globules. 8 The English Method , also called the ( Wet Gum Method ), relies on the use of mucilage or dissolved gums and generally involves the use of a mortar and pestle. The ratio of oil: water: emulsifier often ranges from 3-4:2:1 for forming the primary emulsion. The mucilage is made first by adding a small quantity of water to the hydrocolloid, e.g. acacia, with trituration until uniform. The oil is added in small quantities with rapid trituration. The mixture will become thick and viscous. Additional water is added very slowly with rapid trituration until complete. The Continental Method , also called the ( Dry Gum Method ), also generally uses the mortar and pestle. The ratio of oil: water emulsifier for preparing the primary emulsion is generally approximately 4:2:1. The dry gum method involves mixing the hydrocolloid with the oil with rapid mixing for only a very short time, followed by the addition of all the water at once with very rapid trituration until a snapping sound is heard, This indicates that the primary emulsion is formed. The required amount of additional water is added slowly with rapid trituraton until complete. The Bottle Method (shaking) can be used in the preparation of emulsions containing volatile oils and other non-viscous oils. It avoids the splashing problem sometimes encountered using the mortar and pestle. The bottle method is a variation of the dry gum method and involves mixing the powder (emulsifier) and oil in a bottle followed by rapid shaking with short strokes. The required quantity of water is added all at once and the mixture shaken rapidly to form the primary emulsion (4:2:1 ratio). The additional water, if required, is added in small quantities with shaking after each addition. It is very important NOT to allow the oil and the gum to be in contact too long as the gum may imbibe the oil and cause the powder to become somewhat waterproof. The Beaker Method is often used with synthetic emulsifying agents. The prescription ingredients generally are divided into two separate phases: oil and water. The two phases are heated individually to about 60-70oC, if needed. The internal phase is then added to the external phase with stirring. The product is removed from the heat and gently and periodically stirred, until cooled (congealed). 9 Incorporating materials into a water-in-oil emulsion: Oils and insoluble powders can be incorporated directly using a pill tile and spatula or mortar and pestle. If large amounts of insoluble powders are required, it may be necessary to use a levitating agent. In many water-in-oil emulsions, there is sufficient agent to emulsify an additional reasonable quantity of an aqueous solution of a drug which can be incorporated on a pill tile with a spatula, mortar and pestle, or by gentle heat using a water bath. If heat is used, the preparation should not be held at a high temperature very long as loss of some water may occur, resulting in a change in volume of the product. The addition of oily ingredients usually poses no problem. Some crystalline drugs may need to be dissolved in oil first, if possible. It may be necessary to use the base form and not the salt form of a drug in this case. It is difficult to add water to these emulsions unless an excess quantity of the emulsifier is present. Incorporating materials into an oil-in-water emulsion: Insoluble powders and aqueous solutions can be incorporated using a pill tile and spatula or mortar and pestle. It may be advisable to use a levitating agent such as glycerin or propylene glycol to aid mixing of the insoluble powder with the emulsion. Crystalline materials should be dissolved in a small quantity of water prior to adding to the emulsion. Water-soluble materials can be added by dissolving the powder in a small quantity of water and incorporating the solution into the base. A small quantity of an oil may be incorporated directly into the base as there is usually an excess of emulsifying agent, but if larger amounts of an oil must be added, it may be necessary to add a small quantity of an oil-in-water surfactant to assist in uniform dispersion of the oil in the vehicle. It generally is easy to add water-soluble ingredients. If heat is used while incorporating an ingredient into an oil-in-water vehicle, it is important to work quickly as water may be lost rather rapidly from the product. If this occurs, the product will change in volume and, if a semisolid, may tend to become stiff and "waxy." 10 EXPERIMENT 1 Preparation of Emulsion Using Hydrophilic Colloids as Emulsifying Agent . Acacia Emulsion: Unless otherwise specific , extemporaneously prepared emulsion for internal use are made with acacia gum . To prepare acacia emulsions using a pestle and mortar , thin ( primary ) emulsion must be made first . The quantities for primary emulsions have been determined by experience are given in Table –1 Table –1 Quantities for primary emulsions Quantities of primary emulsions ( parts ) Type of oil Example Oil Water Gum Fixed Almond oil A rachis oil Caster oil Cod – liver oil 4 2 1 Mineral Volatile Liquid paraffin Turpentine oil Cinnamon oil Peppermint oil Male fern extract 3 2 2 2 1 1 1 2 1 Oleo – resin Rx Caster oil 50 ml Double strength chloroform water 100 ml Water ad 200 ml Sent 100 ml HINT :- Double strength chloroform water is prepared by mixing 5 ml of chloroform in 1000 ml of water 11 Procedure 1- Caster oil is a fixed oil , therefore , the quantities for primary emulsion are ( oil : water : gum = 4 : 2 : 1 ) Caster oil Water Acacia 25 ml 12.5 ml 6.25 g 2- use the dry gum technique for Acacia Emulsion as follow a- Weigh the Acacia powder and place it in dry mortar b- Disperse the Acacia powder lightly with water c- Add 12.5 ml oil gradually and triturate until the primary emulsion is well established (by clicking sound) d- The primary emulsion is then diluted with the remaining ingredients and transfer to measuring cylinder to adjust the volume with water 3- Use amber dispensing bottle with a wide mouth 4- Write label & add (shake the bottle before use) use :- Demulcent and Purgative AUST DATE Acacia Emulsion 100 ml Use once daily before sleep Shake well before use 12 Preparation of Emulsion Using Finely Divided Solid Particles as Emulsifying Agent. Calamine Lotion B.P Rx Calamine Zinc Oxide Bentonite Sodium Citrate Liquid phenol Glycerin Purified Water 15 g 5g 3g 0.5 g 0.5 g 5 ml 100 ml Procedure 1) Dissolve Sodium Citrate in 35 ml Purified Water 2) Weigh Calamine, Zinc Oxide and Bentonite & triturate it with Sodium Citrate solution 3) Add Liquid phenol, the glycerin and sufficient quantity of water to make up the required volume. 4) Write the label as follow: AUST DATE Calamine Lotion B.P 100 ml Applied when necessary NAME Shake before use -- External use only Use: - Astringent & protective (soothing effect for itching ) 13 EXPERIMENT 2 Preparation of Emulsion Using Anionic Surfactants White liniment B.P Rx Ammonium chloride Diluted Ammonia solution Oleic acid Turpentine oil Purified water 12.5 g 42 ml 85 ml 225 ml 625 ml After calculation 0.625 g 2 .25 ml 4.25 ml 12.25 ml 31.25 ml Sent 50 ml Calculation factor = 50/1000 =0.05 procedure 1- Make emulsifier (Ammonium Oleate ) the reaction between dilute Ammonia and oleic acid as follow a) Take 4.25 ml of Oleic acid & 12.5 ml of Turpentine oil and 2.2 ml of Diluted Ammonia solution (2.5% ) and 10 ml of water. b) Shake vigorously to form Turpentine H2O emulsion 2- Dissolve 0.625g Ammonium chloride in the remaining water and mix it with to produce the preparation after adjusting the volume with H2O to 50 ml 3- Write label as follow : AUST White Liniment B.P DATE 50ml Rub the surface as directed NAME EXTERNAL USE ONLY - use :- Counter – irritant and rubefacient . 14 Vanishing Cream B.P Rx after calc. Stearic acid Oleic acid Glycerin Boric acid Potassium hydroxide Purified water Q. S 120 g 40 g 50 ml 10 g 8g 1000 g 6g 2g 2.5 ml 0.5 g 0.4 g ad. 50 g Sent 50 g Calculation factor = 50/1000 =0.05 Procedure: 1) 2) 3) 4) 5) 6) 7) 8) 9) Weigh all the ingredient accurately Mix oily substances (stearic & oleic acid) together and heat on water bath Dissolve Pot. Hydroxide in 20 ml water Dissolve Boric acid in 20 ml water Heat aqueous substances at the same water bath Add Pot. Hydroxide with stirring, then add glycerin Neutralize with boric acid solution and keep stirring until cooling. Dispense in container and shake well Make label as follow : AUST DATE Vanishing cream B.P Apply when necessary NAME External use only - Use :- As protective when necessary 15 EXPERIMENT 3 Preparation of Emulsions Using Non-Ionic Surfactant as Emulsifying Agent Utilizing HLB System. Introduction: The HLB (Hydrophile- Lipophile Balance) system is used for describing the characteristics of a surface-active agent. It consists of an arbitrary scale to which HLB values are experimentally determined and assigned. If the HLB value is low, there is a low number of hydrophilic groups on the surfactant and it is more lipophilic (oil soluble) than hydrophilic (water soluble). For example, Span 80 has an HLB value of 4.3, from Table 2, and is oil soluble. If the HLB value is high, there is a large number of hydrophilic groups on the surfactant and it is more hydrophilic (water soluble) than oil soluble. For example, Tween 20 has an HLB value of 16.7 and is water soluble. Some general applications of materials with various HLB values are as follows: Low 1-3 3-6 7-9 8-18 13-16 16-18 Antifoaming agents Emulsifying agents Wetting agents Emulsifying agents Detergents Solubilizing agents (w/o emulsions) (o/w emulsions) Wetting agents are surfactants with HLB values of 7 to 9. Wetting agents aid in attaining intimate contact between solid particles and liquids. Emulsifying agents are surfactants with HLB values of 3 to 6 or 8 to 18. Emulsifying agents reduce interfacial tension between oil and water resulting in minimizing surface energy through the formation of globules. Detergents are surfactants with HLB values of 13 to 16. Detergents will reduce the surface tension and aid in wetting the surface and the dirt. The soil will be emulsified, foaming may occur, and the dirt will wash away. Solubilizing agents have HLB values of 16 to 18. An HLB of 10 or greater is primarily hydrophilic and less than 10 would be lipophilic. Spans have HLB values ranging from 1.8 to 8.6, indicative of oil-soluble or oil-dispersible molecules. Consequently, the oil phase will predominate and the emulsion formed will be water-in-oil. Tweens have HLB values ranging from 9.6 to 16.7, indicative of water-soluble or water-dispersible molecules. Therefore, the water phase will predominate and oil-in-water emulsions will be formed. 16 Blending of Surfactants Often a blend of emulsifiers produces a more stable emulsion than the use of a single emulsifier with the correct, calculated HLB. Since the HLB numbers are additive, the HLB value of a blend can be calculated. For example, if 20 mL of an HLB of 9.65 are required, then two surfactants (with HLB values of 8.6 and 12.8) can be blended in a 3:1 ratio. The following quantities of each will be required: 3/4 x 8.6 = 6.45 (15 mL) 1/4 x 12.8 = 3.20 (5 mL) TOTAL HLB = 9.65 (20 mL) Table 2: HLB Values of Emulsifiers Commercial Name Chemical Name Acacia Glyceryl monostearate Methocel 15 cps PEG 400 Monoleate PEG 400 Monostearate PEG 400 Monolaurate Pharmagel B Potassium oleate Sodium lauryl sulfate Sodium oleate Span 20 Span 40 Span 60 Span 65 Span 80 Span 85 Tragacanth Triethanolamine oleate Tween 20 Tween 21 Tween 40 Tween 60 Tween 61 Tween 65 Tween 80 Tween 81 Tween 85 Acacia Glyceryl monostearate Methylcellulose Polyoxyethylene monooleate Polyoxyethylene monostearate Polyoxyethylene monolauratet Gelatin Potassium oleate Sodium lauryl sulfate Sodium oleate Sorbitan monolaurate Sorbitan monopalmitate Sorbitan monostearate Sorbitan tristearate Sorbitan monooleate Sorbitan trioleate Tragacanth Triethanolamine oleate Polyoxyethylene sorbitan monolaurate Polyoxyethylene sorbitan monolaurate Polyoxyethylene sorbitan monopalmitate Polyoxyethylene sorbitan monostearate Polyoxyethylene sorbitan monostearate Polyoxyethylene sorbitan tristearate Polyoxyethylene sorbitan monooleate Polyoxyethylene sorbitan monooleate Polyoxyethylene sorbitan trioleate 17 HLB Value 12.0 3.8 10.5 11.4 11.6 13.1 9.8 20.0 40.0 18.0 8.6 6.7 4.7 2.1 4.3 1.8 13.2 12.0 16.7 13.3 15.6 14.9 9.6 10.5 15.0 10.0 11.0 Preservation of Emulsions Emulsions will support microbiological growth. Contamination of the products can occur during the preparation of the emulsion as well as during its use. To minimize contamination, the work area and equipment should be clean and every attempt made to produce a "clean" product. However, if the product is to be stored for any length of time, consideration must be given to the addition of a preservative. Table 3: Required HLB Values for Some Common Lipid Material to Prepare o/w Emulsions Material Beeswax Cetyl alcohol Cottonseed oil Lanolin, anhydrous Mineral oil, light/heavy Paraffin wax Petrolatum Stearic acid Stearyl alcohol Required HLB 12 15 10 10 12 11 12 15 14 A preservative must be nontoxic, stable, compatible, inexpensive, and have an acceptable taste, odor and color. It should also be effective against a wide variety of bacteria, fungi and yeasts. Preservatives may partition into the oil phase and lose their effectiveness. Bacterial growth normally will occur in the aqueous phase. Consequently, the preservative should be concentrated in the aqueous phase. Additionally, since the un-ionized form of the preservative will be more effective against bacteria, the majority of the preservative should be present in the non-ionized state. The preservative must neither be bound nor adsorbed to any agent in the emulsion or the container in order to be effective. In summary, only the preservative in the aqueous phase in the free, unbound, unadsorbed, un-ionized state will be effective in emulsions. Example preservatives often used in emulsions are shown in Table 4. The parabens (methylparaben, propylparaben, butyl-paraben) are among the most satisfactory preservatives for emulsions. Antioxidants for Emulsions Oils and fats are subject to rancidification resulting in a product exhibiting an unpleasant odor, appearance and taste. In order to minimize this, antioxidants can be added to the preparation. Example antioxidants are listed in Table 5. 18 Flavoring Emulsions The selection of an appropriate flavoring agent must be made with consideration of the external phase of the emulsion. For example, if a flavoring oil is used and the majority partitions into the internal phase, the flavor strength will be reduced. Oils can be incorporated using small quantities of surfactants (usually surfactants with HLB values of 15-18 are used, often in conjunction with a surfactant with an HLB value in the range of 8 to 12). As a general rule, from three to five times as much surfactant as oil is required to insure solubilization. In order to accomplish this with best results, the oil should be mixed with the surfactants prior to addition into the aqueous phase. Since there is a loss of some of the potency of the flavor using this technique, an alternative is to use a cosolvent system rather than a surfactant system to incorporate the flavor. The use of ethanol, glycerin or some appropriate solvent often provides acceptable results. Table 4: Preservatives Used For Emulsions Alcohol Benzoic acid, sodium benzoate (pH< or = 1 4) Benzyl alcohol (pH 5) Chlorobutanol* Imidazolidinyl Urea (Imidurea) Mercurials Organic Mercurials Phenylmercuric Nitrate Phenylmercuric Acetate Thimerosal 15% 0.05-0.10% 1-4% 0.5% 0.05-0.5% 0.005% 0.002-0.004% 0.002-0.004% 0.005-0.02% Parabens** Methylparaben 0.05-0.3% Propylparaben 0.02-0.2% Butylparaben 0.02-0.2% Quaternary Ammonium Compounds Benzalkonium Chloride 0.002-0.1% Sorbic acid (pH<6) 0.1-0.2% *Chlorbutanol needs a pH<5. It will also sorb to plastic. **Usually used in pairs. Low water solubility. Poor taste. May degrade at a pH>8. Use at pH 4-8. 19 Emulsion Stability Emulsion stability can be enhanced by: 1. decreasing the globule size of the internal phase 2. obtaining an optimum ratio of oil to water 3. increasing the viscosity of the system. Since the oil-to-water ratio is frequently determined by the referring physician (concentration of active ingredient: oil), the compounding pharmacist can work with the first and third items listed above to enhance the emulsion's stability. TABLE 5: Antioxidants for Emulsions Ascorbic acid Ascorbyl palmitate Butylated hydroxyanisole Butylated hydroxytoluene Gallic acid 4-Hydroxymethyl-2, 6, -di-tert-buylphenol Propyl gallate Sulfites L-Tocopherol If the globule size is reduced to less than 5 microns, the stability and dispersion of the emulsion will increase. This can be accomplished with the shearing action of a mortar/pestle and an homogenizer. The optimum phase volume ratio generally is obtained when the internal phase is about 40-60% of the total quantity of the product. As the percentage of the internal phase increases, the viscosity of the product also increases. Enhancement of viscosity of the external phase also will tend to enhance the stability of the emulsion. This is accomplished by the addition of a substance which is soluble in or miscible with the external phase of the emulsion. For o/w emulsions, hydrocolloids can be used. For w/o emulsions, waxes and viscous oils as well as fatty alcohols and fatty acids can be used. Of obvious concern in the preparation of emulsions is their physical stability. This is characterized by an absence of creaming and coalescence and the maintenance of the original appearance, odor, color and other physical properties. Creaming occurs when the globules flocculate and concentrate in one specific part of the emulsion. This results in a lack of uniformity of drug distribution and unsightly product. Creaming is most often characterized in o/w emulsions by the oil globules gathering and rising to the top. This is due to a the fact that the oil generally is less dense than the water phase. Creaming is easily reversible and the product can be evenly redistributed by shaking. It is reversible because the dispersed globules 20 still have the protective film around them. Two methods of minimizing creaming include enhancing the viscosity of the external aqueous phase and reducing the globule size to a very fine state with an homogenizer. Another approach would be to adjust the densities of both the internal and external phase so that the densities are the same, which would result in no tendency for either phase to rise to the top or settle to the bottom. Coalescence, or breaking, is an irreversible process since the film surrounding the individual globules has been destroyed. Viscosity alterations may help to stabilize these and minimize a tendency to coalescence. An optimum viscosity can be experimentally determined. Another factor is the phase volume ratio, or the ratio of the internal volume to the total volume of the product. A maximum phase volume ratio that can be achieved, assuming perfectly spherical particles, is 74%. In general, a phase-volume ratio of about 50%, which approximates loose packing of spherical particles (i.e., a porosity of 48% of the total bulk volume of a powder), results in a reasonably stable emulsion. Phase Inversion Phase inversion can be viewed as both good and bad. It occurs when an emulsion inverts from one form to another, that is, o/w to w/o or w/o to o/w. Phase inversion can result in the formation of a better emulsion and is the basis for the Continental method of emulsion preparation. Monovalent cations tend to form o/w emulsions and divalent tend to form w/o emulsions. If sodium stearate is used initially to form an o/w emulsion, followed by the addition of a calcium salt to form calcium stearate, then the emulsion inverts from an o/w into a w/o emulsion. The Continental method of emulsion preparation involves the use of a small proportion of water in the presence of a large proportion of oil. The initial emulsion nucleus that is formed is of the w/o type. Further addition of water, in small quantities, eventually results in an inversion into an o/w emulsion. General Comments on Emulsions - The viscosity of emulsions generally increases upon aging. - The greater the volume of the internal phase, the greater the apparent viscosity. - There is a linear relationship between emulsion viscosity and the viscosity of the continuous phase. - It has been said that, under a given set of conditions, an oil-in-water emulsion is more easily produced with glass equipment and a water-in-oil emulsion is more easily produced with water-repellent plastic equipment. This could be related to the "wet ability" of the external phase in contact with the surface of the equipment 21 Rx Liquid paraffin Wool fat Cetyl alcohol Emulgent Water to 35 1 1 7 100 -Required HLB values of the first three ingredients are respectively 12, 10 and 15 for an o/w emulsion. The total percentage of oil is ( 35 + 1 + 1 = 37 % ) , and the proportions of the oil phases ingredients are :- Liquid paraffin 35 / 37 = 94.6 % - Wool fat 1 / 37 = 2.7 % - Cetyl alcohol 1 / 37 = 2.7 % The total required HLB value is obtained as follows : Liquid paraffin 94.6 % × 12 = 11.4 Wool fat 2.7 % Cetyl alcohol 2.7 % ( The total required HLB ) × 10 × 15 = 0.3 = 0.4 = 12.1 - Assume that a mixture of sorbitan monolaurate (Span 20 has HLB value = 8.6 ) and polysorbate 80 (HLB value = 15 )is to be used as the emulgent blend . The proportion of these two substance that will provide the required HLB value of 12.1 is calculated as follows: - Let x = the percentage of sorbitan monolaurate in the mixture Then 1 – x = the percentage of polysorbate - Contribution from sorbitan monolaurate = 8.6 × ( x) - Contribution from polysorbate 80 = 15 × [(1 – x)] - since the total contribution must = 12.1 , the expression for calculating ( x ) is , 8.6 × (x) + 15 × [(1 – x)] = 12.1 8.6 x + 15 - 15x = 12.1 2.90 = 6.4x x = 45.3 % 22 - Hence , the percentages of the emulsifying agents in the mixture are : Sorbitan monolaurate Polysorbate 80 45.3% 54.7% - Since the total percentage of the mixed emulgents in the formula is 7 , the percentages of the individual substances are Sorbitan mono-oleate Polysorbate 80 7 × 45.3% = 3.17 g 7 – 3.17 = 3.83 g Procedure: Weight 35g of liquid paraffin, 1 g of wool fat, 3.17 g of span 20 and 1 g cetyl alcohol. Place them in a beaker and try to dissolve with gentle heating. Dissolve 3.83 g of Tween 80 in 64 ml of water. Add Tween solution to the oily phase with stirring Write label 23 Part 2 OINTMENTS 24 Introduction : Ointments are used topically for several purposes, e.g., as protectants, antiseptics, emollients, antipruritics, kerotolytics, and astringents. The vehicle or base of an ointment is of prime importance if the finished product is expected to function as any one of the above categories. In the case of a protective ointment, it serves to protect the skin against moisture, air, sunrays and other external factors. It is necessary that the ointment neither penetrates the human skin barriers nor facilitates the absorption of substances through this barrier. An antiseptic ointment is used to destroy or inhibit the growth of bacteria. Frequently bacterial infections are deeply seated; a base that has the capacity to either penetrate or dissolve and release the medication effectively is therefore desired. Ointments used for their emollient effect should be easy to apply, be non-greasy and effectively penetrate the skin. Physical Characteristics of Ointment Bases There are five (5) classes or types of ointment bases that are differentiated on the basis of their physical composition. These are: Oleaginous bases Absorption bases Water in oil emulsion bases Oil in water emulsion bases Water soluble or water miscible bases Each ointment base type has different physical characteristics and therapeutic uses based upon the nature of its components. The following table summarizes the composition, properties, and common uses of each of the five types. For more information consult Remington's. 25 PROPERTIES OF OINTMENT BASES Oleaginous bases Composition Water Content Affinity for Water oleaginous compounds anhydrous Absorption Bases W/O Emulsion Bases O/W Emulsion Bases Water Miscible Bases oleaginous base oleaginous base + oleaginous base + water (> 45% Polyethylene water (< 45% w/w) + w/o w/w) + o/w Glycols + w/o surfactant surfactant surfactant (HLB (PEGs) (HLB <8) >9) anhydrous, anhydrous hydrous hydrous hydrous hydrophobic hydrophilic hydrophilic hydrophilic hydrophilic Spreadability difficult difficult moderate to easy easy moderate to easy Washability nonwashable nonwashable non- or poorly washable washable washable unstable, oils poor; unstable, especially especially alkali hydrocarbons alkali soaps and soaps and natural stable Stability better natural colloids colloids; nonionics better solids, oils, and solid and solids or oils solids, oils, and solid and Drug aqueous aqueous aqueous solutions aqueous Incorporation (oil solubles solutions (small solutions (small only) (small amounts) solutions Potential amounts) amounts) poor, but > Drug Release poor fair to good fair to good good oleaginous Potential* yes yes sometimes no no Occlusiveness protectants, emollients (+/protectants, emollients, emollients, ), vehicles for emollients (+/cleansing creams, vehicles for aqueous ), vehicles for vehicles for solid, solid, liquid, or drug vehicles Uses solutions, hydrolyzable liquid, or non- non-hydrolyzable solids, and nondrugs hydrolyzable drugs drugs hydrolyzable drugs Hydrophilic Cold Cream type, Petrolatum, Hydrophilic White Hydrous Lanolin, Anhydrous Ointment, PEG Petrolatum, Rose Water Lanolin, Dermabase™, Ointment, Examples White Ointment, Aquabase™, Velvachol®, Polybase™ Ointment Hydrocream™, Aquaphor®, Unibase® Eucerin®, Nivea® Polysorb® *Varies depending upon specific content of the ointment base and the relative polarity of the drug(s) incorporated. This table refers more generally to the release of a typical nonelectrolyte (primarily lipophilic) drug. 26 oils poor; hydrocarbons better Oleaginous Bases To incorporate an insoluble drug into these bases, pulverize the powder on the pill tile or with a mortar and pestle (above/right). Use a levigating agent to wet the powder and then incorporate the wetted powder into the ointment base. Generally, the amount of drug to be incorporated into the ointment will be much less than the amount of ointment. In other words, a small amount of drug will be incorporated into a large amount of ointment. The processes of geometric dilution will "diluted" the drug into the ointment. Geometric dilution involves a series of dilution steps. It begins by incorporating the drug into an amount of ointment of approximately the same size. Then a second amount of ointment approximately equal to the first mixture is added and mixed. This stepwise dilution process is continued all of the ointment has been used. A good levigating agent is mineral oil since it is compatible with oleaginous bases. Sometimes using a small quantity of the base itself as the levigating agent is sufficient. Soluble drugs can be incorporated into oleaginous bases by fusion. The base is liquefied over low heat (not to exceed 70°C) and then the drug is added to the molten base. The mixture is then allowed to cool with occasional stirring. Show how to incorporated a drug into an ointment using geometric dilution & 2 spatulas Absorption Bases An absorption base is an oleaginous base that contains a w/o emulsifying agent. When water is taken up into the base, it will form a w/o emulsion. Absorption bases typically can incorporate about 50% of their volume in water. Incorporating insoluble drugs into these bases can be done mechanically or by fusion. The final destination (internal or external phase of the emulsion) of the drug must be considered when selecting a levigating agent. If the drug will reside in the internal phase (water phase), then the levigating agent should be water soluble or miscible. Water, glycerin, alcohol, or propylene glycol would be suitable levigating agents. If the drug will reside in the external phase, then mineral oil should be used. Water soluble ingredients can be added to the water phase of the w/o emulsion. If the drug will dissolve in a small amount of water, the aqueous solution can be added directly to the base using a pill tile and spatula. If a larger quantity of water is needed to solubilize the drug or if an aqueous solution is being added to the base, heat may be needed to compound the formulation. It may be necessary to add additional emulsifier to the emulsion to accommodate the added water. Some commercial emulsions do have the necessary excess emulsifier. 27 W/O Emulsion Bases Oils and insoluble powders can be directly incorporated into the external phase using a pill tile and spatula. If a levigating agent is to be used with the insoluble powders, it should be miscible with the oil phase; mineral oil would be a suitable agent. Levigating agents may be needed with larger quantities of insoluble powders. If the insoluble powder has a different salt form that is oil soluble, consideration should be given to using that salt form. The same comments that apply to incorporating water-soluble ingredients into absorption bases also apply to w/o emulsion bases. O/W Emulsion Bases Water-soluble powders can be directly incorporated into the external phase using a pill tile and spatula. If the powder is insoluble, the levigating agent should be water miscible so glycerin, propylene glycol, polyethylene glycol (PEG) 300 or 400, or alcohol would be acceptable. If the insoluble substance has a different salt form that is aqueous soluble, consideration should be given to using that salt form. It may be more difficult to incorporate oil soluble ingredients into the o/w formulation. A small amount of oil can be incorporated into the base if there is excess emulsifier. Some commercial products do have the necessary excess emulsifier. If a larger portion of oil is to be added, the addition of more emulsifier may be necessary. If heat is used to incorporate the oil, it is important to work quickly so that water is not evaporated from the product. This will cause the product to become stiff and waxy. Water Miscible Bases Water soluble drugs can be dissolved in a small quantity of water and incorporated using a pill tile and spatula. Insoluble powders will require a water miscible levitating agent such as glycerin, propylene glycol, or polyethylene glycol 400. Oils can be added into these bases by first mixing the oil with glycerin or propylene glycol, and then incorporating the mixture into the base. Heat may be necessary if the quantity of liquid to add to the base is large. 28 GENERAL COMMENTS ABOUT COMPOUNDING OINTMENT BASES Between 2 and 4 grams of an ointment may be lost in the compounding process. The ointment is lost as it adheres to beakers, ointment tiles, or ointment pads. To compensate for this loss, make an excess of the ointment. Some general rules might be to add 10% or 3 grams excess to the prescribed amount. When heat is used to melt ingredients, use a water bath or special low temperature hotplate. Most ingredients used in ointment bases will liquefy around 70°C These two heating devices provide adequate control over the heating and will ensure that the ingredients are not over heated. A water bath will only heat to the boiling point of water which is 100°C. Special "low temperature" hotplates (full range is 25°C to 120°C) are not a standard laboratory type hotplate; those hotplates heat at 125°C to 150°C at their lowest setting. When both an oil and aqueous phase are being mixed together to make an ointment, it is helpful to heat the aqueous phase a few degrees higher than the oil phase prior to mixing. The aqueous phase tends to cool faster than the oil phase and may cause premature solidification of some ingredients. However, use the lowest temperature possible and keep the time of heating as short as possible. This will minimize the quantity of water lost through evaporation. When melting a number of ingredients, melt the ingredient with the highest melting point first. Then gradually reduce the heat to melt the ingredient with the next lowest melting point. Continue this process until all ingredients have been added. This will ensure that the ingredients were exposed to the lowest possible temperature and thus enhance the stability of the final product. The cooling step in an ointment's preparation is an important part of the compounding process. Do not accelerate the cooling process by putting the melt in water or ice. This will change the consistency of the final product making it more stiff than desired. 29 If adding volatile ingredients such as oils, flavors, or drugs, add them when the product is "cool to the back of the hand." The melt will still be fluid enough for adequate mixing but not hot enough to evaporate the ingredient. Ointments should be cooled until just a few degrees above solidification before they are poured into tubes or jars. They should be thick, viscous fluids. This will minimize "layering" of the ointment in the packaging container. However, this is not the preferred method of packing an ointment tube or jar. Most bases achieve their final consistency and texture several hours after they are compounded. 30 EXPERIMENT 4 Simple ointment Rx Hard paraffin White soft paraffin Send 20g 50g 950g Procedure : 1- The weighed amount of hard paraffin is placed in a dish and heated on a water bath until complete melting. 2- Then add the weighed amount of white soft paraffin to the dish content and mix complete melting. 3- Remove the dish from water bath and mixes well until complete congeal. 4- Transfer into a wide mouthed screw capped jars. Uses : Emollient and as vehicle for other preparation . Storage : In cool place in a wide mouth screw capped jar . Macrogol ointment BP. Rx Hard Macrogol Liquid Macrogol Send 20g 500g 500g Procedure: Melt the hard Macrogol, add the liquid Macrogol, and stir until cold. Note: Hard Macrogol is polyethylene glycol 4000and liquid Macrogol is polyethylene glycol 400.Store it in cool place in wide mouth screw capped jar. Uses: Emollient 31 EXPERIMENT 5 Absorption base ointment Rx Hard paraffin Wool fat White soft paraffin Send 20g 50g 50g 900g Label: to be applied as directed. Procedure: 1- The weighed amount of white soft paraffin, wool fat and hard paraffin are placed in a dish and heated on a water bath until complete melting. 2- Remove the dish from water bath and mixes well until complete congeal. 3- Transfer into a wide mouthed screw capped jars. Uses: Emollient and as a vehicle for other preparation. Storage: To be stored in cool place in a wide mouthed screw capped jars. Rx Emulsifying wax BP. Cetostearyl alcohol Sodium lauryl sulfate Purified water Send 20g 90g 10g 4ml Procedure: Melt the cetostearyl alcohol and heat to about 85 add the sodium lauryl sulfate, mix add the purified water, heat to 85, and maintain at this temperature , stirring vigorously , until frothing ceases and the product is translucent . Cool quickly. Storage: Store it in cool place in wide mouth screw capped jar. Uses: To prepare emulsifying ointment 32 Rx Emulsifying Ointment BP Emulsifying wax White soft paraffin Liquid paraffin Send 20g 300g 500g 200g Procedure: Melt emulsifying wax, white soft paraffin and liquid paraffin together in water bath and stir until cold. Note: Emulsifying ointment is used to prepare aqueous cream BP. which contains almost 70 percent of water. Storage: Store it in cool place in wide mouth screw capped jar. 33 EXPERIMENT 6 Evaluation of Drug Release from Ointment Bases Introduction: One of the most important functions of an ointment is the control it exerts over the release and therefore the therapeutic activity of the medication, which it carries. Although the vehicles, or base may not penetrate the skin to any extent , it is known that the clinical effectiveness of a drug may vary when it is incorporated in different vehicles . These variations in drug release and absorption are a function of the physical and chemical properties of both the vehicles and the drug. In the present experiment, you will evaluate the facility with which a number of vehicles, or ointment bases release salicylic acid. The ointment bases involved in this study include: Oleaginous base (white ointment USP) Water soluble base (polyethylene glycol ointment USP) Emulsion base: a. Hydrophilic ointment USP. b. Cold Cream. This study will involve determining the rate of drug release from ( one side of ) a layer of ointment in which the drug is initially dissolved , as well as to study the effect of the drug concentration and the presence of an inert filler on the drug release from that ointment ( review Higuchi’s equation ) . Procedure: 1. The students will be divided into seven groups . Each group will study salicylic acid release from one of the following preparations : A. B. C. D. E. F. G. 34 10% salicylic acid in white ointment (USP) 2% salicylic acid in PEG ointment (USP) 5% salicylic acid in Cold cream . 5% salicylic acid in hydrophilic ointment (USP) 10% salicylic acid in hydrophilic ointment (USP) 10% salicylic acid in hydrophilic ointment (USP) + 2% talc. 10% salicylic acid in hydrophilic ointment (USP) + 10% talc. 2. Each group will be provided to be studied , bottle-cap , rubber band , semi – permeable membrane (dialysis tubing 1¼ ) stand , magnetic stirrer , magnetic bar , 2-7 ml pipettes , two cuvetts , one 600 ml beaker and 600 ml of 1% Trinder’s reagent . 3. Place the ointment in the bottle cap and level the ointment with the edge of the cap . 4. Place the semi-permeable membrane over the ointment and use the rubberband to hold the membrane in place . 5. Use the camp to hold the bottle cap with the ointment surface downwards. 6. Measure 400 ml of 1% Trinder’s reagent and put it in 600 ml beaker . Put the magnetic bar in the beaker and then place it on the magnetic stirrer. Start the stirrer at its lowest speed . 7. Lower the clamp into the 1% Trinder’s reagent so that the ointment surface is just immersed in the reagent and note the time . 8. Take a 5 ml sample every 15 minutes, and replace it with fresh 5 ml of 1% Trinder’s reagent. Tabulate the result in the following sheet: Ointment used : -------------------------------------------------------------------Sample # Time (mins) 1 2 3 4 5 6 7 8 9 10 15 30 45 60 75 90 105 120 135 150 Absorbance Total amount released 9. Assay for salicylic acid in each sample. To assay your solutions two spectrophotometer cuvettes are needed, one for the blank and the second to be used for the solution to be assayed. I. 35 Fill the blank cuvette with 1% Trinder’s reagent solution, and wipe it free of the dust oil. Insert it in the holder of the Spectro 22RS, close top and adjust to 100 % Transmittance, Make sure you position the etched marking on the cuvette toward the front of the holder each time you insert it. II. Remove the blank from the holder of the Spectro 22RS and make sure the needle returns to zero transmittance , if not adjust it and repeat procedure again . II. Fill the second cuvette with the sample. Insert it in to the Spectro 22RS holder , close cover and read the absorbance value on the meter . Start with the most dilute sample and progress to the most concentrated. Raise the cuvette each time with a small amount of the sample being assayed. Repeat procedure with each sample and check to the 100 % reading with the blank solution between each sample reading. 10. At the end of the lab. , each student should have a set of data for each of the experiments . 11. Calculate the amount of Salicylic acid released from the ointment as a function of time using the following equation: n Amount released = An/a x (400) + (5/400) i Where (A) (a) (i) (n) Ai /a x (400) = the absorbance . = the absorptivity (i.e. slope of Beer’s plot = 12.25 mg/ml ) = Sample number = Integar (5/400) i Ai /a x (400) = the amount due to dilution effect upon replacing the sample with release medium . n-1 12.List the amount of salicylic acid released ( calculate in step 10 ) on the working sheet . 13.Calculate the surface area of the bottle cap. Data Analysis : 36 Using the working sheet for the seven experiments , calculate the amount released per unit area of ointment . Plot the amount released per unit area vs. time and draw a smooth curve through the data points for each ointment. Plot amount released per unit area vs. the square root of time and draw the best line through the data points for each ointment. Compare the release rate of salicylic acid from the different ointment bases Observe the effect of salicylic acid concentration on the release rate. Observe the effect of Talcum powder (and its concentration) on the release rate. Part 3 OPHTHALMIC AND PARENTRAL PERPARATIONS 37 Calculations required for Intravenous Admixture and TPN Prescription compounding is a rapidly growing component of pharmacy practice. This can be attributed to a number of factors, including individualized patient therapy, lack of commercially available products, home healthcare, intravenous admixture programs, total parenteral nutrition programs and "problem solving" for the physician and patient in enhancing compliance with a specific therapeutic regimen. Pharmacists are creative and should have the ability to formulate patient-specific preparations for providing pharmaceutical care. Most compounded prescriptions require a number of calculations as part of preparation, packaging and dispensing. These calculations include milliequivalents, millimoles, osmolality, concentration terms, and dilution of stock solutions. Experiment 7 Preparation of Solution with given milliequivalents, millimoles and milliosmoles: Equivalent weight is the molecular weight divided by the valence of the molecule and milliequivalent is one thousandth of the Equivalent. However, Moles are weight of solute in gm/formula weight [i.e (w2/M2 ) and millimoles are one thousandth of the moles [[(w2/1000*M2 )]. Where, w2= wt. of solute and M2 = molecular weight of solute. On the other hand, Osmolality = [number of moles * number of ions] and milliosmoles = [ # of moles /(1000* # of ions)] For Examples; 1. Preparation of one liter of 25 milliequivalents of sodium chloride. 1 equivalent NaCl = 58.5 gm, 1 milliequivalent = 58.5mg; Therefore, The quantity of NaCl required = 25 mEq x 58.5 mg/mEq = 1.463 g 2. Preparation of one liter of 10 mEq of Ca++ using a standard 10% CaCl2 . Ca++ = 40/2 = 20 mg/mEq Using proportionality. Then 1/10 mEq = 20 mg/ x and x = 200 mg of Ca++ required Since, CaCl2 = 40 + 71 = 111, Then 40/111 =200/ x mg and x = 555 mg CaCl2 required 38 10 /1000ml = 0.555 g / x and x = 55.5 mL of the 10% CaCl2 solution Millimoles: How many millimoles of NaCl are contained in 1 liter of 0.9% Sodium Chloride Solution? (Formula weights: Na=23, Cl=35.5, NaCl=58.5). 0.009 x 1000 mL = 9 g NaCl 1 mole NaCl weighs 58.5 g 1/58.5g = x /9g , x = 0.154 mole = 154 millimoles Osmolality: What is the osmolality (number of milliosmoles) of 1 liter of 0.9% sodium chloride solution? (Assume complete dissociation) Na=23, Cl=35.5, NaCl=58.5, NaCl --> Na+ + Cl # millimoles NaCl present per liter = 154 from previous problem 154 millimoles NaCl x 2 species (Na + Cl) = 308 mOsmol/liter What is the osmolality of 10% CaCl2 solution? (Assume complete dissociation) (Formula weights: Ca=40, Cl=35.5, CaCl2=111g/L) 10% CaCl2 = 100 g/1000 mL 100 / 111 g = x / 1 mole x = 0.9 moles/liter = 900 millimoles CaCl2 ----> Ca++ + 2 Cl = 3 species 900 millimoles CaCl2/L x 3 species = 2700 mOsmol/Lite Stock Solutions: A pharmacist is preparing an ophthalmic decongestant solution in batch form. Each of three bottles will contain 15 mL. The preservative to be incorporated is 0.01% benzalkonium chloride (BAK). The pharmacist has a stock solution containing 17% BAK. How much of this stock solution would be required for the three bottles? 15 x 3 = 45 mL 45 x .0001 = .0045 g 0045/ x =17/100 x = 0.026mL Specific Gravity in Weighing/Measuring: A pharmacist receives a prescription for 120 mL of a 3% w/v Hydrochloric Acid solution. The density of concentrated hydrochloric acid (37%) is 1.18 g/mL. How many milliliters of the concentrated acid would be required for the Rx? 3% = .03 .03 x 120 mL = 3.6 g required Volume =3.6 g/1.18 g/mL= 3.05 mL 37% = 0.37 , 3.05 mL /0.37= 8.24 mL 39 Mixing Products of Different Strengths: A pharmacist receives an order for 120 g of a 0.1% corticosteroid ointment. On hand are 1 oz of 0.1%, 2 oz of 0.15% and 2 ½ oz of 0.005%, all in the same ointment base. If these three ointments are mixed together, how much additional corticosteroid powder should be added to prepare the prescription? Assume the quantity of corticosteroid added will be negligible compared to the 120 g total weight. 120 x .001 = 120 mg needed 30 x 0.001 = 30 mg 15 x .0015 = 22.5 mg 75 x .00005 = 3.8 mg -----Total 56.3 mg 120 mg - 56.3 mg = 63.7 mg In what quantities could a 50% dextrose in water be mixed with a 5% dextrose in water to obtain 900 mL of 15% dextrose in water? 50 10 ÷ 5 = 2 15 5 35 ÷ 5 = 7 ------- Total: 9 parts (2/9)x 900 = 200 mL of D50W (7/9)x 900 = 700 mL of D5W ------------900 mL Total Volume Powders for Reconstitution: The directions to constitute an amoxicillin suspension 250 mg/5 mL, 150 mL, state that 111 mL of Purified Water are required. The physician has requested the product be constituted at a concentration of 500 mg/5mL. How much Purified Water would be required? 150 mL - 111 mL = 39 mL occupied by powder 250 mg/5 mL = 50 mg/mL 50 mg/mL x 150 mL = 7.5 g of powder 7.5/0.5 = 15 doses 15 doses x 5 mL = 75 mL volume 75 mL - 39 mL = 36 mL required 40 Units to Weight Conversions: A Rx order calls for 150,000 units of nystatin per gram of ointment with 60 grams to be dispensed. How much nystatin would be weighed? (4400 USP Nystatin units/mg) 150,000 u/g x 60 g = 9,000,000 units needed 9,000,000/4400 u/mg = 2.045 g required Shelf Life Estimates: Shelf life estimates can be made using the equation: t90 Orig t90New = -------3∆T/10 where ∆T = change in temperature 3 is a reasonable estimate for the "Q" value, based on energies of activation from the Arrhenius equation. An antibiotic solution has a shelf-life of 96 hours when in a refrigerator. If it is necessary that a patient use it in an ambulatory pump at approximate body temperature (30oC) over 6 hours, would it still retain at least 90% of its original potency during the entire period of administration? t90 =96 /325/10 = 6.16 hours Ans. = yes A prescription is received for an ophthalmic solution with a shelf-life of 4 hours at room temperature. The preparation is to be administered in a physicians office at 12:00 noon the next day. Can it be prepared the evening before at about 8:00 pm and still retain at least 90% of its shelf life if stored in a refrigerator? t90 = 4 / 3-20/10 = 4 / 3-2 = 36 hours Ans. Yes A reconstituted antibiotic has a shelf-life at room temperature of 3 days. How long would the preparation be good if stored in a refrigerator? (A reasonable estimate based on (t90). t90 = 3d / 3 2 = 3 X 9 = 27 days Ophthalmic and Nasal Solutions-Sodium Chloride Equivalents: How much sodium chloride is required to render the following Rx isotonic? Rx Lidocaine HCl 1% (NaCl equiv. = 0.22) Cocaine HCl 1% (NaCl equiv. = 0.16) 41 Epinephrine Bitartrate Sterile Water qs Sodium Chloride qs 50 x .01 = 0.5 x .22 = 50 x .01 = 0.5 x .16 = 50 x .001 = .05 x .18 = 0.1% (NaCl equiv. = 0.18) 50 mL 0.110 0.080 0.009 ----0.199 g The ingredients represent the equivalent of 0.199 g of NaCl. 50 x .009 = 0.45 g 0.45 - 0.199 = 0.251 g NaCl to make 50 mL water isotonic NaCl needed to add to this Rx to make it isotonic Ophthalmic and Nasal Solutions-Buffer Solutions & pH: Rx Optimycin NaCl Phosphate Buffer pH 6.5 qs 1% qs 100 mL (Sorensen Modified Phosphate Buffer ) Acid Stock Solution (1/15 M) Sodium Biphosphate, Anhy. 8.006 g Purified Water qs 1000 42 Alkaline Stock Solution (1/15 M) Sodium Phosphate, Anhy. 9.473 g Purified Water qs 1000 mL pH 5.9 6.2 6.5 6.6 6.8 7.0 7.2 7.4 7.7 8.0 mL of 1/15 M Sodium Biphosphate Solution 90 80 70 60 50 40 30 20 10 5 mL of 1/15 M Sodium Phosphate Solution 10 20 30 40 50 60 70 80 90 95 To prepare 100 mL of pH 6.5 phosphate buffer solution, use 70 mL of 1/15 Molar Solution Biphosphate Solution and 30 mL of 1/15 Molar Sodium Phosphate Solution. 43 EXPERIMENT 7 Preparation of Isotonic Buffered preserved Solution Introduction : Solutions having identical osmotic pressure are said to be isotonic . For fluids to be in the humans , an isotonic solution is one having the same osmotic pressure as the body fluids e.g. blood , tears , or other tissue fluids . Tonicity is dependent upon the number of particles of substance in solution regardless of the nature of the particles , whether they be ions , molecules or aggregates of molecules . Thus , some substances do not dissociate on going into solution but exist in solution as molecules . Examples of such un dissociated substances are dextrose and sucrose . Others , such as sodium chloride and similar salts , dissociate more or less completely into ions . It requires 0.9 g of Sodium Chloride ( M.W. 58.45 ) per 100 c.c. to make an isotonic solution . while 9.2 g of Sucrose ( M.W. 342.3 ) are needed to produce the same osmotic effect .It can be seen that the dissociation of a substance exerts a marked effect on the osmotic pressure produced while the molecular weight of the compound is relatively unimportant . Preparation of Isotonic Solutions : In order to calculate the osmotic pressure of the fluid to be prepared , we use one or more of the colligative properties of solutions . Of these , the direct determination of freezing point or the determination of the vapor pressure of solutions in relation to the vapor pressure of known solutions of sodium chloride are the most commonly employed because of their accuracy and relative ease of determination . When using the freezing point-depression , the problem is to obtain a solution which will have the same freezing point as blood or tears , or – 0.52 o C . Since , in dilute solutions , the lowering of the freezing point and the increase in osmotic pressure are directly proportional to the total number of particles in solution , it is obvious that solutions which have the same freezing point will have the same osmotic pressure . Thus when we wish to convert a hypotonic solution to an isotonic solution , we add sufficient particles , usually of sodium chloride or of dextrose , to lower the freezing point to that of blood or lacrimal fluid . 44 Methods of Calculations : Sodium Chloride Equivalent Method A sodium chloride equivalent ( E ) may be defined as a factor which converts a specific amount of solute to the amount of sodium chloride which will produce the same osmotic effect . For example , the sodium chloride equivalent of boric acid is 0.55 this means that 1 g of boric acid in solution produces the same number of particles as 0.55 g of sodium chloride , also that 10 gr. Of boric avid is equivalent to 5.5 grains of sodium chloride . The method is based on the fact that molar lowering of freezing point is proportional to the ratio of the freezing point depression produced by the solute to its molar concentration . L = ∆t / C Where L = Molar lowering of the freezing point ∆t = depression of freezing point produced by the solute ( o C ) C = Molar concentration of the solute To calculate the sodium chloride equivalent (E) of a substance the following equation is used : E = L/M ( 58.45/3.4 ) Where E is the sodium chloride equivalent of a substance having molecular weht M and molar freezing point depression L . 58.45 = M.W. of sodium chloride 3.5 = L value of chloride Table I shows the values of the molecular weights ( M ) the molar freezing point depression ( L) , and the sodium chloride equivalents ( E) of some substances of pharmaceutical importance . To calculate the sodium chloride the Sodium Chloride equivalent of Sodium Acid Phosphate ( NaH2PO4H2O ) L = 3.2 M= 138.0 E= L/M ( 58.45 / 3.4 ) = 3.2 / 138.0 ( 53.45 / 3.4 ) = 0.40 45 To calculate the sodium chloride equivalent of sodium phosphate ( anhydrous ) ( Na2HPO4) L= 4.4 M=141.98 E= L/M ( 58.45/3.4 ) = (4.4 / 141.98) (58.45/3.4 ) = 0.53 Table I Substance Alcohol ,dehydrated Antipyrine Barbital Sodium Benadryl hydrochloride Caffeine Dexrose.H2O Ephedrin hydrochloride Glycerine Pilocarpine nitrate Sodium acid phosphate (NaH2PO4.H2O) Sodium phosphate ,anhydrous Sodium phosphate ,7 H2O M L E 46.07 188.22 206.18 291.81 194.19 198.17 201.69 92.09 271.27 138.00 1.9 1.9 3.5 3.5 0.9 1.9 3.6 1.8 3.7 3.2 0.70 0.17 0.29 0.29 0.08 0.16 0.30 0.34 0.23 0.40 141.98 268.08 4.4 4.6 0.53 0.29 These values were taken from Martin’s “ Physical Pharmacy “ pg.255-256 . Sorenson Buffer System Stock solutions : Sodium Biphosphate (NaH2PO4.H2O ) : 9.208 g/1000 ml . Sodium phosphate (Na2HPO4 ) : 9.470 g/1000 ml . Sample calculation for case # 1 . ( Refer Table II ) Q . 90 ml of SODIUM BIPHAOSPHATE Sock Solution + 10 ml of SODIUM PHOSPHATE Stock Solution Result in pH of 5.91 What is the Sodium Chloride equivalent of the buffer ? 46 A . Amount of Sodium Biphosphate = ( 9.208 / 1000 ) x 90 = 0.8287 g Amount of Sodium phosphate = [( 9.470 x10 )/1000] = 0.0947 g Sodium Chloride equivalent (E) for Sodium Biphosphate = 0.40 ( from example 1 or Tables ) Sodium Chloride equivalent ( E) for Sodium Phosphate = 0.53 ( from example 2 or Tables ) 1 g Sodium Biphosphate = 0.40 g of Sodium Chloride 0.8287 g of Sodium Biphosphate = 0.40/1 x 0.8287 = 0.3315 g of Sodium Chloride 1 g Sodium Biphosphate = 0.53 g of Sodium Chloride 0.0947 g Sodium Phosphate = ( 0.53 x 0.0947 ) / 1 = 0.0502 g of Sodium Chloride Amount of Sodium Chloride required to make an isotonic solution = 0.90g / 100 ml Amount of Sodium Chloride required to make an isotonic buffered solution = 0.90 – ( 0.3315 + 0.0502 ) = 0.52 EXERCISES Fill in the blanks in the table below before you come to the lab. Show all the calculations. TABLE II # Sodium Biphosphate Solution ( ml ) 1 2 3 4 5 6 7 8 9 10 90 80 70 60 50 40 30 20 10 5 47 Sodium Phosphate Solution ( ml ) 10 20 30 40 50 60 70 80 90 95 Resulting pH 5.91 6.24 6.47 6.64 6.81 6.98 7.17 7.38 7.73 8.04 Sodium Chloride Required to make Isotonic Solution 0.52 Procedure In the following prescription: Rx Isotonic Pilocarpine Nitrate ( 0.5 % w/v ) Solution Buffered at pH 7.38 Prepare 50 ml Apply one drop to each eye as directed by the physician 1. Make 25 ml of Sorenson’s buffer (pH 7.38 ) by mixing the required amounts of sodium biphosphate stock solution and sodium phosphate solution . 2. Weigh out pilocarpine nitrate and sodium chloride .Sodium chloride is used to adjust isotonicity ; the sodium chloride equivalent ( E) of pilocarpine nitrate is 0.23 . 3. Dissolve the pilocarpine nitrate and sodium chloride in the buffer prepared in 1. 4. Adjust the volume to 50 ml with water . 5. Check the pH of the solution (pH paper or pH meter ). 6. Transfer to a 2 oz. Bottle and label . Calculations : 1. From Table II figure out the composition of Sodium Bicarbonate and Sodium Phosphate solutions which will provide the required pH . 2. Calculate the amount of sodium chloride equivalent of each ingredient . (This is done by multiplying the amount of each ingredient by its sodium chloride equivalent ) 3. Add the equivalent amounts of sodium chloride . 4. Subtract the equivalent amount of sodium chloride from the value of an isotonic sodium chloride solution ( 0.9 g /100 ml ) Quantities : required to fill the above prescription : Pilocarpine nitrate Sodium Bicarbonate Stock Solution Sodium Phosphate Stock Solution Sodium Chloride Sterile Purified Water Q.S. 48 -------------- g -------------- ml -------------- ml -------------- ml 50 ml EXPERIMENT 8 Compounding of Ophthalmic Liquids Introduction Ophthalmic solutions are sterile, free from foreign particles and especially prepared for instillation into the eye. Ophthalmic suspensions are sterile liquid preparations that contain solid particles in a suitable vehicle intended for instillation into the eye. Composition(s) In addition to the active drugs, ophthalmic preparations contain a number of excipients, including vehicles, buffers, preservatives, tonicity adjusting agents, antioxidants and viscosity enhances. Important in the formulation process is the use of ingredients that are nonirritating and compatible with the eyes. Preparation Methods/Techniques All work must be done in a clean-air environment, such as a laminar flow hood, by qualified aseptic compounding pharmacists. The source of all the ingredients must be the highest grade that can be reasonably obtained. Solutions: 1. Accurately weigh/measure each of the ingredients. 2. Dissolve the ingredients in about 3/4 of the quantity of Sterile Water for Injection and mix well. 3. Add sufficient Sterile Water for Injection to volume and mix well. 4. Determine the pH, clarity and other quality control factors from a sample of the solution. 5. Filter through a sterile 0.2 micron filter into a sterile ophthalmic container. 6. Package and label. 7. If a large number are to be prepared, select a random sample to be checked for sterility and to be assayed. Suspensions: 1. Accurately weigh/measure each of the ingredients. 2. Mix the ingredients in about 3/4 of the quantity of Sterile Water for Injection and mix well. 3. Add sufficient Sterile Water for Injection to volume and mix well. 4. Determine the pH, and other quality control factors from a sample of the suspension. 5. Package in a suitable container for autoclaving. 6. Autoclave, cool and label. 7. If a large number are to be prepared, select a random sample to be checked for sterility and to be assayed. 49 Or: 1. Accurately weigh/measure each of the ingredients. 2. Sterilize each of the ingredients by a suitable method. 3. Mix the ingredients in about 3/4 of the quantity of Sterile Water for Injection and mix well. 4. Add sufficient Sterile Water for Injection to volume and mix well. 5. Determine the pH, and other quality control factors from a sample of the suspension. 6. Package and label. 7. If a large number are to be prepared, select a random sample to be checked for sterility and to be assayed. Physicochemical Uniqueness of Common Ingredients Considerations in preparing ophthalmic solutions involve clarity, tonicity, pH/buffers, sterility, preservatives, antioxidants, viscosity enhancers, and proper packaging. Clarity-Ophthalmic solutions must be free from foreign particles, which is generally accomplished by filtration. The filtration process also helps to achieve clarity of the solution. Table 1 contains a list of usable clarifying agents. Tonicity-Lacrimal fluid has an isotonicity value equivalent to that of a 0.9% sodium chloride solution. However, the eye can tolerate a value as low as 0.6% and as high as 1.8% sodium chloride equivalency. Some ophthalmic solutions will be hypertonic by nature of the high concentration required of the drug substance. Others will be hypotonic and will require the addition of a substance to attain the proper tonicity range. Sodium chloride, boric acid and dextrose are commonly used. Three hundred mOsm/L is ideal with 200-600 mOsm/L acceptable. pH and Buffering-Ophthalmic solutions are ordinarily buffered at the pH of maximum stability for the drug(s) they contain. The buffers are included to minimize any change in pH during the storage life of the drug; this can result from absorbed CO2 from the air or from hydroxyl ions from a glass container. Changes in pH can affect the solubility and the stability of drugs, consequently, it is important to minimize fluctuations in pH. The buffer system should be designed sufficient to maintain the pH throughout the expected shelf-life of the product but with a low buffer capacity so as soon as the ophthalmic solution is dropped into the eye, the buffer system of the tears will rapidly bring the pH of the solution back to that of the tears. This is accomplished by using as low a concentration of the buffers salts as possible but still be effective. Generally a buffer capacity less than 0.05 is desired. pH generally in the range of 4-8 is considered optimum. 50 Sterility-Ophthalmic solutions must be sterile. Sterility is best achieved through sterile filtration using a sterile membrane filter of 0.45 or 0.2 micron pore size and filtering into a sterile container. Other methods of sterilizing ingredients or components of ophthalmics that can be used by compounding pharmacists include dry heat, steam under pressure (autoclaving) and gas sterilization (ethylene oxide). Preservation-Since most ophthalmic solutions/suspensions are prepared in multiple use containers, they must be preserved. The selected preservative must be compatible with the active drug as well as all the other excipients in the product. Common preservatives for ophthalmic products are shown in Table 2. Antioxidants may be required for selected active drug ingredients. Tables 3 contains antioxidants that can be used in ophthalmic preparations. Viscosity enhancers-An increase in the viscosity of ophthalmic products will result in a longer residence time in the eye, providing a longer time for drug absorption and effect. Numerous materials are used, among which methylcellulose is the most common, generally in a concentration of about 0.25% if the 4000 cps grade is used. If methylcellulose is autoclaved, it will come out of solution. However, it can be re dispersed after cooling, especially if placed in a refrigerator. Hydroxypropyl methylcellulose in the range of 0.5 to 1% is a good viscosity enhancer, while polyvinyl alcohol 0.5 to 1.5% w/v is an alternative. Solution viscosity in the range of 25-50 cps is common. It is important that solution clarity be maintained with the use of these viscosity enhancers. Suitable viscosity increasing additives are shown in Table 4. Packaging of ophthalmic solutions is appropriately done in sterile dropper bottles or individual doses can be placed in sterile syringes, without needles. Ophthalmic suspension particles must be of such a size that they do not irritate and/or scratch the cornea, therefore a micronized form of the drug is required. Ophthalmic suspensions must also be free from agglomeration or caking. Incompatibilities Zinc salts can form insoluble hydroxides at a pH above 6.4, so a Boric Acid Solution vehicle may be selected. It also has a lower pH (about pH 5) and slight buffering action. Nitrates or salicylates are incompatible with solutions of benzalkonium Chloride, therefore it should be replaced with 0.002% phenylmercuric nitrate. Sodium chloride cannot be used to adjust the tonicity of silver nitrate solutions since silver chloride would precipitate. Sodium nitrate should be used to adjust the tonicity and phenylmercuric nitrate can be used as the preservative in this situation. 51 Storage/Labeling Generally, ophthalmic preparations should be stored at either room or refrigerated temperatures and should not be frozen. Stability Beyond-use dates for water-containing formulations is not later than 14 days, when stored at refrigerated temperatures, for products prepared from ingredients in solid form. If non aqueous liquids, the beyond-use recommendation is not later than 25% of the time remaining until the products expiration date or 6 months, whichever is earlier. For all others, the recommended beyond-use recommendation is the intended duration of therapy or 30 days, whichever is earlier. These beyond-use recommendations can be extended if there is supporting valid scientific stability information, as explained in the General Compounding Chapter of the United States Pharmacopoeia 23/National Formulary 18. Example Vehicles Isotonic Sodium Chloride Solution: Sodium Chloride USP Benzalkonium Chloride Sterile Water for Injection 0.9 g 1:10,000 qs 100 mL Boric Acid Solution: Boric Acid USP Benzalkonium Chloride Sterile Water for Injection 1.9 g 1:10,000 qs 100 mL Rx Artificial Tears: Polyvinyl alcohol Povidone Chlorobutanol 0.9% Sodium chloride solution 1.5% 0.5% 0.5% qs Instructions: 1. Calculate the quantity of each ingredient for the total amount to be prepared. 2. Accurately weigh or measure each ingredient. 3. Dissolve all ingredients in the sterile 0.9% sodium chloride solution. 4. Filter through a 0.2 micron filter into a sterile ophthalmic container. 5. Package and label. 52 Table 1: Wetting/clarifying agents used for ophthalmic preparations. Agent Polysorbate 20 Polysorbate 80 Usual Concentration (%) 1% 1% Table 2: Common preservatives used in ophthalmic products. Preservative Name: Usual Concentration: Concentration Range: Chlorobutanol Maximum Concentr Incompatibilities: ation: 0.5% soaps anionic materials salicylates nitrates Quaternary Ammonium Compounds: Benzalkonium chloride Benzethonium chloride Organic Mercurials: Phenylmercuric acetate Phenylmercuric nitrate Thimerosal Parahydroxybenzoates 0.01% 0.004-0.02% 0.013% 0.01% Certain halides with phenylmercuric acetate. 0.001-0.01% 0.004% 0.004% 0.01% 0.1% Adsorption by macromolecules. The maximum levels are listed by the FDA Advisory Review Panel on OTC Ophthalmic Drug Products (1979) for direct contact with the eye tissues and not for ocular devices such as contact lens products. 53 Table 3: Antioxidants used for ophthalmic preparations. Antioxidant Ethylenediaminetetraacetic acid Sodium bisulfite Sodium metabisulfite Thiourea Usual Concentration (%) 0.1% 0.1% 0.1% 0.1% Table 4: Viscosity increasing agents for ophthalmic preparations. Agent Hydroxyethylcellulose Hydroxypropyl methylcellulose Methylcellulose Polyvinyl alcohol Polyvinylpyrrolidone 54 Usual Concentration (%) 0.8 1.0% 2.0% 1.4% 1.7% 1. Buffers and Buffer Capacity Using dibasic potassium phosphate (K2HPO4) and monobasic potassium phosphate (KH2PO4), prepare 500 ml of a buffer solution at pH 7.4 with a buffer capacity of 0.05. Using a pH meter, measure the pH of 100 ml of the solution. Titrate 100 ml of the solution with 1 N NaOH until the pH increases by one unit and determine whether the buffer capacity is as calculated. Note that the exact normality of the NaOH solution may vary with available stock solutions; note and record the exact normality of the reagent you use in the experiment. Calculate the buffer capacity as: ∆B= gram equivalent of strong acid/base to change pH of 1 liter of buffer solution ∆pH= the pH change caused by the addition of strong acid/base Calculations: MW K2HPO4 _________________ MW KH2PO4 _________________ Ka ________________ pKa _______________ K2HPO4 = __________ g KH2PO4 = __________ g Data and Results: Measured beginning pH _______ Volume of ____N NaOH added to 100 ml to change pH by 1 unit = _________ Eq NaOH added _______ Measured buffer capacity _______ 55 2. Isotonicity and Sterility Use the NaCl equivalent method and appropriate compounding techniques to prepare the following sterile, isotonic ophthalmic solution. Rx Procaine HCl 1.5 % Benzalkonium chloride 1:10,000 Boric Acid q.s. Aqua. dest. q.s. ad 60 ml M.Ft. Sterile, isotonic solution Sig. gtts ii o.u. t.i.d. Procaine HCl _______________________ g (E = ___________ ) Benzalkonium chloride _______________ g (E = ___________ ) Boric Acid _________________________ g (E = ___________ ) Benzalkonium chloride 1:1,000 solution needed __________________ ml Calculations: Compounding Procedure: Therapeutic use: ___________________________________ Measured osmolality ________________________________ (mmol/Kg) 56 EXPERIMENT 9 3. Isotonicity and pH Adjustment A. Prepare the following prescription. Rx Ampicillin Sodium Sodium chloride q.s. 30 mg/ml M.Ft. 15 ml of sterile, buffered, isotonic solution at pH 6.6 Sig. gtts ii o.u. t.i.d. Ampicillin sodium ______________________ g (E = _____________) Sodium chloride _______________________ g Monobasic sodium phosphate, anhydrous (NaH2PO4) 0.0667 M solution needed ____________ ml Dibasic sodium phosphate, anhydrous (Na2HPO4) 0.0667 M solution needed _______________ ml Calculations: Compounding Procedure: Therapeutic use: ___________________________ Measured osmolality _____________________ (mmol/Kg) B. Make calculations to prepare the following prescription as a buffered isotonic solution at pH = 5.9. Describe how you would prepare the solution using 500 mg/vial Vancomycin Sulfate powder for injection (when reconstituted with 9.7 ml sterile water for injection makes a 50 mg/ml solution), Sodium Chloride 30% (concentrate) for injection, and stock solutions of 0.0667 M NaH2PO4and 0.0667 M Na2HPO4. Do not prepare. Rx Vancomycin sulfate 30 mg/ml Sodium chloride q.s. Monobasic sodium phosphate q.s. Dibasic sodium phosphate q.s. M.Ft. 15 ml of sterile, buffered, isotonic solution at pH 5.9 Sig. gtts ii o.u. t.i.d. Vancomycin sulfate ________________________ mg (E = __________) 57 Monobasic sodium phosphate, anhydrous (NaH2PO4) 0.0667 M solution needed __________________ ml Dibasic sodium phosphate, anhydrous (Na2HPO4) 0.0667 M solution needed __________________ ml Sodium chloride (30%) concentrate needed _____________ ml Calculations: Compounding Procedure: Therapeutic use: ____________________________ Label _____________________________ 58 PART 4 IV ADMIXTURE 59 Introduction a. Attitude: Number one rule: always think of the patient. A well thought out training program for aseptic technique should focus on safety and accuracy. Safety: a.) The finished product should be free of contamination (particles, bacteria, extraneous material). b.) The solution should be clear -- all medications should be completely dissolved. c.) All compounding materials should be checked for expiration date, outer integrity, etc. Accuracy: Guidelines must be set up to ensure the right drug, right dose, and right concentration. This includes using the appropriate syringe size to measure out fluid volumes in order to minimize errors. Another example would be to require that all syringes be drawn back to the original amount of each individual dose and placed next to the admixture to facilitate checking by the pharmacist. If a filter needle was required, it should also be present. b. Dangers of poor aseptic technique: Patients who are receiving intravenous therapy tend to be the most critical. Every precaution must be taken to avoid contamination. The IV route is the most dangerous route of administration because it bypasses all of the body's natural barriers. An improperly prepared solution when administered can have very serious consequences: infections, emboli, occlusions and even......... Guidelines for Sterile Compounding Pharmacists have been providing sterile compounding services in institutions for decades. These services have provided parenteral therapies, infusion services, and complex infusion administration devices and supplies. However, in the past two decades, compounding sterile formulations and providing administration services has expanded beyond the institution. These additional areas include home care agencies, infusion service agencies, outpatient clinics, and community pharmacies. Pharmacists are also providing patient and caregiver assessments, education, and skills, and are taking the responsibility for coordinating patient care through an interdisciplinary team. Pharmacists will compound a wide variety of sterile formulations in these different settings. These formulations will include products administered by injection (IV, IM, SQ, ID, intrathecal, epidural) or via inhalation, intranasal, or ophthalmic routes of administration. Sterile formulations for either institutional or home care use have a number of special requirements such as: 60 sterility particulate material pyrogen-free stability pH osmotic pressure Sterility is the freedom from bacteria and other microorganisms. Formulations must be sterile, which is not a relative term; an item is either sterile or not sterile. If the sterile formulation is a solution, it must be free of all visible particulate material. Particulate materials refer to the mobile, undissolved substances unintentionally present in parenrtal products. Examples of such material are cellulose, glass, rubber cores from vials, cloth or cotton fibers, metal, plastic, rust, diatoms, and dandruff. Sterile suspensions and ointments may have particulate material, but these are usually the active drug or an ingredient, not contaminants. Particles measuring 50 microns or larger can be detected by visual inspection. Specialized equipment is needed to detect particles less than 50 microns in size. The USP 24/NF19 Section <788> sets limits on the number and size of particulate that are permissible in parentral formulations. For large volume parenterals, the limit is not more than 12 particles/ml that are equal to or larger than 10 microns, and not more than 2 particles/ml that are equal to or larger than 25 microns. For small volume parenterals, the limit is 3000 particles/container that are equal to or larger than 10 microns, and not more than 300/container that are equal to or larger than 25 microns. The potential sources of particular material are: 1. The product itself 2. Manufacturing and such variables as the environment, equipment, and personnel 3. The packaging components 4. The administration sets and devices used to administer the product 5. The manipulations and environment of the product at the time of administration. Sterile formulations must be pyrogen-free. Pyrogens are metabolic by-products of living microorganisms. So if pyrogens are detected in a sterile product, that means that bacteria have proliferated somewhere along during the formulation process. In humans, pyrogens cause significant discomfort but are rarely fatal. Symptoms include fever and chills, cutaneous vasoconstriction, increased arterial blood pressure, increased heart workload, pupillary dilation, piloerection, decreased respiration, nausea and malaise, severe diarrhea, or pain in the back and legs. 61 The stability of drugs in sterile formulations is an important consideration. In institutional settings, most admixtures are prepared hours in advance of when they are to be administered, and are generally utilized within a short period or time. In home health care settings, admixtures are prepared days in advance of when they are to be administered, and are generally utilized over longer periods of time compared to the clinical setting. Therefore, the stability of a particular drug in a particular sterile formulation must be known. Physiological pH is about 7.4, and an effort should be made to provide sterile formulations that do not vary significantly from that normal pH. Of course, there are situations in which this becomes a secondary consideration because acidic or alkaline solutions may be needed to solubilize drugs or used as a therapeutic treatment themselves. Osmotic pressure is a characteristic of any solution that results from the number of dissolved particles in the solution. Blood has an osmolarity of approximately 300 milliosmoles per litter (mOsmol/L), and ideally any sterile solution would be formulated to have the same osmolarity. The most commonly used large volume parenteral solutions have osmolarities similar to that of blood; for example, 0.9% sodium chloride solution (308 mOsmol/L) and 5% dextrose solution (252 mOsmol/L). Intravenous solutions that have larger osmolarity values (hypertonic) or smaller osmolarity values (hypotonic) may cause damage to red blood cells, pain, and tissue irritation. However, there are some therapeutic situations where it may be necessary to administer hypertonic or hypotonic solutions. In these cases, the solutions are usually given slowly through large veins to minimize the reactions. During the early 1990s, guidelines were issued by NABP, ASHP, and the USP regarding the compounding of sterile products. These recommendations were an effort to provide assistance to pharmacists and technicians responsible for preparing sterile products. However, none of these recommendations has been uniformly adopted and accepted which has resulted in inconsistent practice conditions. The NABP Model Rules for Sterile Pharmaceuticals are the most general guidelines and do not address some of the key features found in other guidelines. However, they enumerate the basic considerations in sterile compounding. Policy and procedure manuals for compounding, dispensing, and delivering sterile products should be established and periodically reviewed. These records should be part of a documented, ongoing quality assurance program. Pharmacists and supportive personnel should be trained and adhere to hygienic and aseptic techniques 62 Sufficient reference materials about sterile products should be available Drugs and supplies should be stored, labeled, and disposed of properly Sterile compounding should be done in an area separate from other activities Procedures should be established for assigning beyond-use dates that exceed the manufacturer labeled expiration dates Equipment, Supplies, and Devices: Laminar flow hoods (horizontal and vertical) Laminar flow hoods are used to control airborne contamination of sterile products during their extemporaneous preparation. Room air is filtered through a high efficiency particulate air (HEPA) filter removing 99.97% of all particles 0.3 microns or larger. Parallel air streams bathe the work area with a velocity sufficient to provide the area free of particles and microorganisms. The direction of airflow may be horizontal or vertical. Horizontal flow hoods are most commonly used, with the more costly vertical flow hoods being reserved for agents that may produce an environmental hazard (e.g. cytotoxic agents, radioactive agents, antimicrobial agents). Horizontal Flow Hood Vertical Flow Hood Laminar flow hoods used in sterile compounding must be Class 100 (less than 100 particles of 0.05 micron size per cubic foot). 63 Laminar flow hoods are effective only when properly used. Interruption of the air flow will interfere with the effectiveness of the hood. Downstream contamination occurs when any object comes between the HEPA filter and the sterile product, interrupting the parallel flow and creating dead space. Cross-stream contamination may occur due to rapid movements of the operator in the hood. Backward contamination may be caused by turbulence created by objects being placed in the hood, by fast traffic passing the hood, or by coughing, sneezing, etc. by the operator. It should be remembered that the hood does not produce sterilization, but merely prevents contaminants from settling onto the surface of the sterile product. Any movement of greater velocity and different direction than that of the hood's air flow will create a turbulence that reduces the hood's effectiveness. Working at a smooth, steady pace at least 6 inches into the hood may minimize contamination. Filtration and Filters: Filtration is used to remove particles from solutions. These particles might be particulate matter or they may be microorganisms. Filtration is not a "terminal sterilization" procedure as are steam (moist heat), dry heat, ionized radiation, or gas sterilization. Filtration will sterilize the product, but after filtration, the sterile product is then aseptically combined with its packaging. Filtration is used for materials that are chemically or physically unstable if sterilized by heat, gas, or radiation. There are two types of filters, depth filters and membrane filters. Depth filters are seldom used for sterilization. They are constructed of randomly oriented fibers or particles (e.g., diatomaceous earth, porcelain, asbestos) that have been pressed, wound, or otherwise bonded together to form a tortuous pathway for flow. The microorganisms are either entrapped in the path or adsorbed to the filter material. The random structure of material inside the filter creates fluid flow 64 pathways that can vary from extremely narrow to very wide. Filter materials can also break off or come loose during filtration and appear in the filtrate. Depth filters are rigid enough to filter a solution being pulled into a syringe. They can also be used to filter a solution being pushed out of a syringe. But the same filter cannot be used to draw up and then expel a solution. A new needle is required before pushing the solution out of the syringe. If the solution is expelled through the original filter needle, the solution will be re-contaminated. Screen filters have a continuous uniform structure that consists of fixed size pores. Particles that are larger than the pore openings cannot pass through the filter and are retained on the surface of the filter. The amount of material retained by a screen filter is limited by the surface area of the filter. Screen filter pore sizes can be predetermined and precisely controlled during manufacturing. The most common screen filter used in compounding is called a "membrane filter." In terms of structure, membrane filters are thin microporous sheets made from a variety of plastics. Membrane filters must have a nominal pore size of 0.22 microns or less if they are to be used for sterilization. However, membrane filters are available in a wide range of pore sizes from 0.11 to 10 microns. Membrane filters are intended to filter a solution only as it is expelled from a syringe. If a solution is to be drawn into a syringe and then filtered through a membrane filter, use the following procedure: 1. 2. 3. 4. 5. 6. 7. A regular needle (or a depth filter needle) is attached to the syringe. The solution is pulled into the syringe. Air bubbles are removed from the syringe. The needle is removed from the syringe. A membrane filter unit is then attached to the syringe. A regular needle is placed on the needle end of the filter. Air is eliminated from the filter chamber by holding the syringe in a vertical position so that the needle is pointing upward. Air must be expelled before the filter becomes wet; otherwise, the air will not pass through the filter. 8. Once air has been expelled, pressure should be slowly and continuously applied to push the solutions through the filter. Membrane filters also eliminate the risk of air embolism. Once a membrane filter is wet, air cannot pass through it unless the "bubble point pressure" of the filter is exceeded. "Bubble point pressure" for a 0.22 micron membrane filter is approximately 55 psi, a pressure that will not occur during parenteral administration. So any air that enters the administration set will be stopped at the filter surface and not allowed to enter the patient's body. 65 The same bubble point pressure is used in another way. After a filter is used, the integrity of the filter can be determined if the wetted filter is exposed to a high pressure. If the filter is intact, the appearance of bubbles on the filter surface should occur when the pressure is about 50 - 55 psi. However, if the filter integrity has been compromised, the bubble point pressure will be much lower. Membrane filters are often packaged in a round plastic holder which can easily be attached to the end of syringes. Some filters are attached to administration sets and serve as "final filters" and filter the solution immediately before it enter the patient's vein. Some administration sets have filters already built into the set. Filters can also be placed inside of needles; these are called "filter needles." Double ended filter needles which is a simple unit that has a filter between two needles. This allows solution transfer directly from one container to another container and eliminates the need of using a syringe to transfer the solution. Filters are also supplied as single membrane units to be used in specialized filtration apparatus. Several things must be considered when selecting a membrane filter: Hydrophilic filters are easily wetted and are used for aqueous solutions. Hydrophobic filters repel water but allow solvents such as alcohol and air to pass. So these filters would be used to sterilize solutions containing alcohol or isopropyl alcohol, or as air filters. Other considerations include the volume capacity of the filter, how much pressure can be applied to the filter without damaging its integrity, and what is the filter's compatibility or adsorption profile for the material being filtered. The material to be filtered also requires some considerations. Viscous oils can be filtered, but it is a time consuming process. Heating the oil will reduce its viscosity and make filtration easier. Some powders can also be filtration sterilized by first dissolving the powder in a solvent, filtering the resultant solution, and then evaporating the solvent under aseptic conditions. Consideration must also be given to the sterilization of containers, closures, and apparatus. A non-sterile surface that comes in contact with a sterilized product will render the product non-sterile. These contact surfaces must also be pyrogenfree. The temperatures and times necessary for depyrogenation are substantially greater than those for sterility. It will probably be necessary to depyrogenate containers, closures, and apparatus separately from the formulation and then aseptically combine them. 66 Types of Parentral Solution Large Volume Parenteral (LVP) Solutions Parenteral solutions are packaged as large volume parenteral (LVP) solutions and small volume parenteral (SVP) solutions. LVP solutions are typically bags or bottles containing larger volumes of intravenous solutions. Common uses of LVP solutions without additives include: 1) correction of electrolyte and fluid balance disturbances; 2) nutrition; and 3) vehicle for administering other drugs. Large volume parenteral solutions are packaged in containers holding 100 ml or more. There are three types of containers: glass bottle with an air vent tube, glass bottle without an air vent tube, and plastic bags. Plastic bags have advantages over glass bottles: they do not break; they weigh less; they take up less storage space, and they take up much less disposal space. However, some drugs adsorb to the plastic. Also, some drugs and solutions leach a plasticizer out of the plastic; the plasticizer is included to keep the plastic pliable. There are now newer plastics that minimize some of these problems. Plastic bags are available in different sizes. The most common sizes are 250, 500, and 1,000 ml. The top of the bag has a flap with a hole in it to hang the bag on an administration pole. Graduation marks are on the front of the bag to indicate the volume of solution used. They are marked at 25 ml to 100 ml intervals depending on the overall size of the bag. The plastic bag system collapses as the solution is administered so a vacuum is not created inside the bag. At one end of the bag are two ports of about the same length. One is the administration set port and the other is the medication port. The administration set port has a plastic cover on it to maintain the sterility of the bag; the cover is easily removed. Solution will not drip out of the bag through this port because of a plastic diaphragm about ½ inch inside the port. When the spike of the administration set is inserted into the port, the diaphragm is punctured, and the solution will flow out of the bag into the administration set. This inner diaphragm cannot be resealed once it is punctured. The medication port is also covered by a protective rubber tip. Drugs are added to the solution through this port using a needle and syringe. There is an inner plastic diaphragm about ½ inch inside the port, just like the administration set port. This inner diaphragm is also not self-sealing when punctured by a needle, but the protective rubber tip prevents solutions from leaking from the bag once the diaphragm is punctured. Because of the advantages of plastic bags, glass LVP solution bottles are not often used. The major advantage of glass bottles is to administer drugs that are incompatible with plastic bags. Glass intravenous bottles are packaged with a vacuum, sealed with a solid rubber closure, and the closure is held in place by an 67 aluminum band. Graduation marks are along the sides of the bottle and are usually spaced every 20 ml to 50 ml. The solution bottle is hung on an administration pole in an inverted position using the aluminum or plastic band on the bottom of the bottle. Solutions in either the plastic bag or glass bottle flow from the containers to the patient through an administration set. But for solutions to flow out of a glass container, air must be able to enter the container to relieve the vacuum as the solution leaves. Some bottles have air tubes built into the rubber closure for this purpose. Some bottles do not, in which case an administration set with a filtered airway in the spike must be used. Many different LVP solutions are commercially available. Four solutions are commonly used either as primary fluids (infused at 2 - 3 ml per minute) or as the base of an admixture solution. The solutions are sodium chloride solution, dextrose solution, Ringer's solution, and Lactated Ringer's solution. Various combinations of different strengths of sodium chloride and dextrose solutions are also available, i.e., 5% dextrose and 0.45% sodium chloride, or 5% dextrose and 0.2% sodium chloride. Small Volume Parenteral Solutions Small volume parenteral (SVP) solutions are usually 100 ml or less and are packaged in different ways depending on the intended use. If the SVP is a liquid that is used primarily to deliver medications, it is packaged in a small plastic bag called a minibag of 50 - 100 ml (minibags look like small plastic LVP bags). SVPs can also be packaged as ampules, vials, and prefilled syringes. Liquid drugs are supplied in prefilled syringes, heat-sealed ampules, or in vials sealed with a rubber closure. Powdered drugs are supplied in vials and must be constituted (dissolved in a suitable liquid) before being added to any solution. SVPs packaged as ampules, vials, or prefilled syringes are typically added to a minibag or a LVP but they may also serve as the final container. The term admixture is used to denote a solution where such an additive has been added to a minibag or LVP. Ready-to-mix systems consist of a specially designed minibag with an adapter for attaching a drug vial. The admixing akes place just prior to administration. The major advantages of ready-to-mix systems include a significant reduction in waste and lower potential for medication error because the drug vial remains attached to the minibag and can be rechecked as needed. However, the systems do cost more, and there is the potential that the system will not be properly activated so that the patient receives only the diluent or a partial dose of drug. 68 Administration Set The basic method to administer a LVP solution is to use an administration set. The set contains a spiked plastic device to pierce a port on the IV container. This connects to a sight or drip chamber that may be used to set the flow rate, the rate ordered by the physician at which the solution is to be administered to the patient (generally measured in ml/hour). A clamp pinching the tubing also regulates flow. The line then leads to a rubber injection port to which a needle may be attached or to an infusion pump which will control the flow rate. Heparin Lock In some instances, a patient may not have a primary LVP solution, yet must receive piggyback medications. This is done through a heparin lock, which is a short piece of tubing attached to a needle or intravenous catheter. When the tubing is not being used for the piggyback, heparin is used to fill the tubing. This drug prevents blood from clotting in the tube. 69 Other Devices Infusion pumps, syringe pumps, and ambulatory pumps are devices used to administer LVP solutions and control flow rates. Administration sets are threaded through infusion pumps, and the pumps control gravity flow. Syringe pumps expel solutions from a syringe into an administration set such as a heparin lock. An ambulatory pump is about the size of a hand. It allows patients to have some freedom of movement compared to being restricted to an infusion pump attached to an adminstration pole. Infusion pumps have made the infusion process much more accurate and easier to administer and have been a major factor in the growth of home infusion. PROCESS VALIDATION In a general sense, validation is any mechanism that will establish a high degree of assurance that specific processes are achieving their objective. Its ultimate goal is to produce products that consistently meet predetermined specifications and quality attributes. Consistent quality (and improvement if possible) is a "must" for the health and well-being of the patient and should be an on-going process. Several types of "quality control" can be developed for sterile compounding. Media Fills The Validation subsection of Section <1206> of the USP 24/NF19 describes an evaluation procedure commonly referred to as "media fills." The evaluation involves an operator manipulating microbial growth media (usually soybean casein digest medium) according to a prescribed validation procedure. The procedure requires multiple aseptic transfers to multiple containers. It is recommended that the validation procedure by done at peak periods of fatigue, stress, and pacing demands (e.g., immediately after normal production activity). The premise behind media fills is that the growth medium will support the growth of the contaminating microbe, and this growth can be detected. The other requirement of the validation is that the media must be manipulated using the same aseptic techniques actually being evaluated. It is important to note that this validation is not intended to be a one time evaluation. The USP 24/NF19 recommends that competent operators be challenged quarterly. Other references suggest that 40 validation sample should be prepared for each 800 admixtures prepared, or that 10 validation samples be prepared each month. Regardless of the frequency, a competent sterile compounder will need to be evaluated on a regular and on-going basis. 70 Other Methods A process validation might involve sending formulations to contract analytical laboratories for testing. Analysis of drug content, sterility, and pyrogenicity can be routinely done using randomly selected samples. Process validation could be observing and testing formulation variables such as color, clarity, uniformity of dispersion, odor, consistency, pH, specific gravity, etc. The validation could also be documenting adherence to formulation records, policies and procedures, SOPs using compounding records, or techniques or procedures. Some example forms for Home Infusion Pharmacies have been published. 71 PROCESS VALIDATION FOR TPN PREPARATION IN LOCAL HOSPITALS IN UAE Title of Policy and Procedure: General Cleaning of the I.V room Policy: The I.V Room must remain a clean room at all times, with routine cleanings and inspections. Procedure: 1. No one is to enter the I.V Room except the pharmacists who are preparing the formulae. 2. No one should open the door of the I.V Room during mixing in order not to disrupt the airflow. 3. No eating, drinking, smoking or any activities what so ever allowed in the I.V Room except intravenous medication preparation. 4. Garbage has to be removed from trash containers outside of the I.V room once it is full or at least daily. 5. Vacuuming or mopping of floor must be done daily when mixing is at a standstill. 6. Daily scrubbing of the sink, floors and shelves must be done with detergents. 7. The sink must remain dry at all times. 8. The temperature of the room must remain within standards of 22 degrees Celsius at all times. 9. The walls are to be scrubbed whenever necessary and on a periodical basis. 10. The environmental services staff daily must sign the daily cleaning log sheet. 11. The refrigerator must remain free of anything except sealed medications, and its temperature maintained between 2-8degree Celsius. 12. The refrig4erator temperature log sheet is to be completed weekly. 72 Title of Policy and Procedure: Personal hygiene in the I.V room Policy: Hygiene is absolutely essential for prevention and control of infections and is a procedure that must be practiced faithfully by all hospital personnel. For the I.V Room, it is mandatory to follow procedure to ensure the cleanest environment possible. Procedure: A. Attire in the I.V Room 1. The I.V Room pharmacist is to dress in theater scrubs if possible, otherwise a sterile gown is to be used on top of clothing and closed properly so street clothes are exposed. The hair must be covered with hair caps upon entry, and a mask must be used during the preparations in the hood. 2. After hand washing, sterile gloves should be used during preparations 3. Clean shoes should be used or shoe covers whenever possible. B. Hand washing 1. Hands must be washed before beginning any work in the sterile preparation area and upon each re-entry into the area. All jewelry and other accessories need to be removed from hands up the elbows. 2. Wet your hands with water. 3. Spread a film of bacteriostatic agent over the entire surface of the hand. 4. Wash thoroughly using a rotary motion and friction over the entire hands, between fingers and nails and well up the wrists for 30seconds to one minute. 5. Rinse Thoroughly 6. Dry hands well by patting or blotting with paper towel 7. Turn off the faucet with a paper towel when the faucet is hand controlled. 8. A bacteriostatic agent maybe used between hand washing. 9. Apply generous amounts of the bacteriostatic fluid to the hands rubbing between digits, Allow to dry, then continue mixing. 73 C. Maintaining Sterility 1. The Pharmacist preparing should not scratch their face or hand or any uncovered areas. 2. Talking, coughing, sneezing should be kept to a minimum. If that pharmacist is ill with an infection, another pharmacist should mix instead if possible; otherwise clean procedures are of even greater importance. 3. If a product is spilled on the gloves, they should be changed immediately. 4. If there is a wound, mixing is only possible if the wound is dry and fully covered. 74 Title of Policy and Procedure: Guidelines for working in the laminar flow hood Policy: While workings in the hood a set of points should be kept in mind in order to ensure that work is done under sterile conditions. Procedure: 1. Work well inside the hood at least six inches away from the outer edge. 2. Avoid nervous gestures and mannerisms (scratching etc). 3. Do not block the air stream to the exposed sterile needle with your hands or fingers. 4. Hands should not be placed between the Hepa filter and when transferring derices. 5. Plac4e the needle top facing the filter not away. 6. When drawing medicines, work horizontally holding the syringe in one hand and the bottle/vial/ampoule in the other. 7. Place the finished needle on the side of the bottle to the right. 8. Select the size and quantity of additives, diluents, syringes etc. to be used for the admixture. 9. Check them for expiration date or any discoloration that would render them unfit for use. 10. External surfaces of items need to be cleaned by an alcohol swab. 11. Place the syringes, ampoules, vials on either or both sides of your majo5r site of activity this will minimize movement. 12. A pharmacist other than the one preparing the mixture must check all preparations. The check should be through; looking for correct ingredients, concentrations, quantities, expiration dates, compatibility, techniques and the final solution. 75 Title of Policy and Procedure: Documentation of TPN formulae Policy: All TPN formulae must be prescribed on the approved forms, entered into the nurse’s kardex and then labeled accordingly. Procedure: 1.Any total Parenteral Nutrition formula needs to be prescribed on the approved prescription TPN form. 2. All the ingredients to be mixed must be written with concentrations and volumes. The prescribing doctor must sign and stamp the form. The nurse must also sign the prescription form. 3.A copy remains in the file and one copy for the I.V Room. The form is used for preparation and is then filed. 4.Any changes made to the original prescription should be initialed by the prescribing doctor. 5. A prescription for TPN to be given should be in the Kardex for the nurses to follow. 6.The Prepared TPN bag is labeled with the exact ingredients wadded to the bag, including volume, concentration or strength accordingly. 7.The bags are labeled with an expiration date, to be kept in the refrigerator label, and to be protected form light written on it. Title Of Policy Procedure: Sterilizing the Laminar Flow Hood Policy: The Laminar flow Hood provides a sterile air space for mixing the medications. Sterilization techniques must be used to ensure this sterile environment is maintained. Procedure: 1. The laminar flow hood is maintained and inspected according to its manual. Specific guidelines are available to ensure its safe and effective use. 2. The hospital engineer must inspect the hood filters monthly and sign the log sheet. If the filters do not meet standards, they must be changed. Both the hepa filter and pre-filters should be changed every 3-4months of use. 76 3. The hood must run for 30 minutes in order to ensure sterile airflow. After that it is sterilized and may be used for medication preparation. 4. The hood is wiped down with alcohol in order to prepare it for use. Gauze is used to wipe the hood with alcohol, starting closest to the filter and moving away. This wiping down effect is in the direction of the airflow from the hood, therefore not obstructing the sterile airflow. All 4 surfaces should be wiped down, as well as the rod. Do Not Wipe The Filter Panel. 5. This wipe down procedure is done every time the hood is switched on (30minutes later) and before the hood is switched off for the day. This wipe down is also performed periodically during preparations, and every time a product is spilled on the hood’s surface. 6. If the hood is left without use for some time or if it is found to be unusually dirty, it is to be cleaned with an appropriate soap using distilled water for dilution and gauze for the scrubbing. 77 Title of the Policy and Procedure: Storage Conditions of I.V room items Policy: The items needed for the preparation of total parenteral nutrition formulae are to be stored under hygienic conditions and at appropriate temperature and light control. The compounded formulae need to be stored under refrigeration until they are administered to be the patient, and protected from light at all times. Procedure: 1. The items needed for the preparation of total parenteral nutrition vary tremendously, and may require different storage conditions. Hence, each item needs to be inspected for storage requirements carefully. 2. All items need to be stored in a cool, dry place. 3. All items needs to be stored in a clean and dust free area, in order not to jeopardize their sterility. 4. Any item that needs to be protected from light or kept under refrigeration, should be stored as such at all times. 5. The compounded formulae are stored in the refrigerator until they are dispensed to the wards. 6. The compounded formulae should be stored for a maximum of 12 hours before being administered to the patient. Calculate the following for 5 prescriptions: 1.The volume of electrolytes to be added to the bag as prescribed 2.The maximum electrolyte concentration that can be used per patient weight 3.The maximum volume per patient weight and age. 4. The calories requirements based on the patient’s diagnosis 5. The calories provided by the prescription. 6. The ratio of calories from nonfat to fat source in the prescription. 7. The rate of infusion based on total volume so that it runs for 24 hours. mMoles= milliquivalents(mEq) Valence of the ion Na=1 valence K=1 Mg=2 Ca=2 PO4=3 Cl=1 78 SO4=2 Acetate=1 Gluconate=2 Meq. Wt= gm/valence 1000 1mEq Na=23mg 1mEq k=39mg 1mEq Ca=20mg 1mEgMg=12mg 1mEq Cl=35.5mg Normal Saline is 0.9% sodium chloride=0.9gm of NaCl/100ml of solution Concentration in mmol/liter = 10 x concentration in mg/ 100ml Molecular weight Calculations Workshop: Solve the following Calculation: 1. Doctor order 30gms of dextrose, we only have 50% dextrose in stock. How many mls of 50% dextrose will we need? 2. We have amino acids 5% order for 70gms total. How many mls of the aminoacid 5% are needed? 3. Convert these: 10mMoles KCl = --------------------mEq KCl 20m Moles Ca = ---------------------mEq Ca 30mEq Kphos = ---------mEq K and ----mEq Phos 20mEq Mg = ----------------------------mMoles Mg 4. If the doctor orders 10 mMoles/Liter of Na, How many mMoles will be in 2500ml bag? 5. Same order as above, how many mls of 30% (5mEq/1ml) NaCl will be needed for the 2500ml bag? 6. Doctor prescribes TPN total volume 1750ml, to be infused over 24 hours. What is the rate of infusion (ml/ Hour)? 7. Mg SO4 ordered to be added to TPN at 10mEq/Liter. The magnesium we have is an MgSO4 50% 4mEq/ml 10 ml vial. The total volume for the TPN bag is 2500ml. How many mls of MgSO4 should be added to the 2500ml bag? 79 8. If the TPN is ordered to run at 100ml/hour, and the total volume is 2000ml. How long will the TPN run for? If it is started at 1200 noon on Monday, what time will it finish? 9. Order for 50mEq of Kphos, 20mEq of NaCl to be added to the final volume of TPN. What is the final content in the TPN of Potassium, Phosphate, Sodium and Chloride? 10. Same order as above, can Ca Gluconate be added to this mixture? How much? 80 Examples of TPN Prescription Prepared For Adults : Example 1 Patient name—No Body-----------------------------File No. 1850xx Age----45------------------Diagnosis------head injury------------------------------Wt. Kg. Ideal Wt. 70 Date----7/5/01------------------------------------- Protein Amino Acid Volume Glucose Dextrose Volume Fat Lipid Volume Sodium Chloride Potassium Chloride Calcium Gluconate Magnesium Sulphate Potassium Phosphate Other Other Trace elements Water Soluble Vitamins Fat Soluble Vitamins Regular Insulin Iron Heparin Total Volume Rate of infusion Duration of Infusion Central Line or Peripheral Line Doctor’s Signature Nurse’s Signature Time Received Time Infusion Started Medications:81 10 500 25 1000 20 500 150 40 10 10 10 2000 80 24 G % ml G % ml G % ml mM/24hrs mM/24hrs mM/24hrs mM/24hrs mM/24hrs ml ml ml U mg U ml ml/hour hour Example 2 Patient name—No Bady-----------------------------File No. 1850xx Age----50------------------Diagnosis-----# Facial Bone------------------------------Wt. Kg. Ideal Wt. 70 Date----7/5/01------------------------------------- Protein Amino Acid Volume Glucose Dextrose Volume Fat Lipid Volume Sodium Chloride Potassium Chloride Calcium Gluconate Magnesium Sulphate Potassium Phosphate Other Other Trace elements Water Soluble Vitamins Fat Soluble Vitamins Regular Insulin Iron Heparin Total Volume Rate of infusion Duration of Infusion Central Line or Peripheral Line Doctor’s Signature Nurse’s Signature Time Received Time Infusion Started Medications:- 82 10 50 25 1000 20 500 50 20 19 20 10 10 10 200 80 24 G % ml G % ml G % ml mM/24hrs mM/24hrs mM/24hrs mM/24hrs mM/24hrs ml ml ml U mg U ml ml/hour hour Example 3 Patient name—No Bady-----------------------------File No. 1850xx Age----45------------------Diagnosis------CRF------------------------------Wt. Kg. Ideal Wt. 75 Date----8/5/01------------------------------------- Protein Amino Acid Volume Glucose Dextrose Volume Fat Lipid Volume Sodium Chloride Potassium Chloride Calcium Gluconate Magnesium Sulphate Potassium Phosphate Other Other Trace elements Water Soluble Vitamins Fat Soluble Vitamins Regular Insulin Iron Heparin Total Volume Rate of infusion Duration of Infusion Central Line or Peripheral Line Doctor’s Signature Nurse’s Signature Time Received Time Infusion Started Medications:- 83 10 500 50 500 20 500 100 30 1 amp. 1 amp. 1 amp. 1650 24 Central G % ml G % ml G % ml mM/24hrs mM/24hrs mM/24hrs mM/24hrs mM/24hrs ml ml ml U mg U ml ml/hour hour Example 4 Patient name—No Bady-----------------------------File No. 1850xx Age----36------------------Diagnosis------Pancreatitis------------------------------Wt. Kg. Ideal Wt. 70 Date----8/5/01------------------------------------- Protein Amino Acid Volume Glucose Dextrose Volume Fat Lipid Volume Sodium Chloride Potassium Chloride Calcium Gluconate Magnesium Sulphate Potassium Phosphate Other Other Trace elements Water Soluble Vitamins Fat Soluble Vitamins Regular Insulin Iron Heparin Total Volume Rate of infusion Duration of Infusion Central Line or Peripheral Line Doctor’s Signature Nurse’s Signature Time Received Time Infusion Started Medications:- 84 10 500 25 1000 20 500 100 40 10 10 10 80 24 Central G % ml G % ml G % ml mM/24hrs mM/24hrs mM/24hrs mM/24hrs mM/24hrs ml ml ml U mg U ml ml/hour hour Example 5 Patient name—No Bady-----------------------------File No. 1850xx Age----47------------------Diagnosis------Pancreatitis------------------------------Wt. Kg. Ideal Wt. 65 Date----9/5/01------------------------------------- Protein Amino Acid Volume Glucose Dextrose Volume Fat Lipid Volume Sodium Chloride Potassium Chloride Calcium Gluconate Magnesium Sulphate Potassium Phosphate Other Other Trace elements Water Soluble Vitamins Fat Soluble Vitamins Regular Insulin Iron Heparin Total Volume Rate of infusion Duration of Infusion Central Line or Peripheral Line Doctor’s Signature Nurse’s Signature Time Received Time Infusion Started Medications:- 85 10 750 25 1250 2000 80 24 Peripheral G % ml G % ml G % ml mM/24hrs mM/24hrs mM/24hrs mM/24hrs mM/24hrs ml ml ml U mg U ml ml/hour hour Example 6 Patient name—No Bady-----------------------------File No. 1850xx Age----39------------------Diagnosis------Pancreatitis------------------------------Wt. Kg. Ideal Wt. 70 Date----7/5/01------------------------------------- Protein Amino Acid Volume Glucose Dextrose Volume Fat Lipid Volume Sodium Chloride Potassium Chloride Calcium Gluconate Magnesium Sulphate Potassium Phosphate Other Other Trace elements Water Soluble Vitamins Fat Soluble Vitamins Regular Insulin Iron Heparin Total Volume Rate of infusion Duration of Infusion Central Line or Peripheral Line Doctor’s Signature Nurse’s Signature Time Received Time Infusion Started Medications:- 86 3 5 500 10 1000 80 10 10 1500 60 24 Peripheral G % ml G % ml G % ml mM/24hrs mM/24hrs mM/24hrs mM/24hrs mM/24hrs ml ml ml U mg U ml ml/hour hour APPENDIX Goal: To familiarize students with the differences in nutritional requirements between adults and children with respect to fluids, electrolytes, calories, carbohydrates, proteins, fats and trace elements. Introduction: Adequate nutrition for the proper growth and development of a child requires individualization. The amount and type of fluid, calories, electrolytes, and trace elements are all based on age, weight, nutritional status, and disease state. I. The total daily fluid requirement of any patient is equal to the normal daily maintenance fluids plus replacement of any fluid deficit plus replacement of any significant abnormal ongoing losses. Two methods to calculate normal maintenance fluids are described below. Normal maintenance fluids provide replacement for normal body functions and for normal losses (for example, insensible water loss, urine output and stool losses). Other factors that may increase the patient's total daily fluid requirements need to be replaced in addition to the normal daily maintenance fluids. Total daily fluid requirement = Normal Maintenance Fluids + Deficit + Ongoing Abnormal Losses Total daily fluid requirements may be increased by: 1) increases in insensible water losses due to such factors as fever, hyperventilation, phototherapy, radiant warming, skin breakdown, burns, etc. 2) initial deficits of fluid i.e., dehydration 3) significant ongoing abnormal losses such as diarrhea, vomiting, nasogastric tube losses, high output renal failure, etc. A. Daily maintenance fluid requirements (i.e., normal maintenance fluids) are those required to maintain normal homeostasis for a 24 hour period. Surface area and body weight are two common methods used for the calculation of maintenance fluids in pediatric patients. NOTE: Premature infants will have greater daily maintenance fluid requirements then those shown here due to their larger surface area to body weight ratio and thinner skin, both of which significantly increase their insensible water losses from the skin. In fact, preterm infants < 750 grams often require 200 - 250 ml/kg/day to prevent dehydration. Due to their highly specialized needs, calculation of fluid 87 requirements for premature neonates will be considered beyond the scope of this lecture. 1. Daily maintenance fluid requirements calculated by body surface area: For pediatric patients, the amount of daily maintenance fluid required is in the range of 1500 - 1800 ml/m2/day. Usually 1500 ml/m2/day is used. The surface area method is usually used in children > 10 kilograms because a precise measurement of surface area is often difficult in smaller infants. 2. Daily maintenance fluid requirements calculated by body weight Weight < 2.5 kg 2.5 - 10 kg 11 - 20 kg > 20 kg Daily maintenance fluid requirements 120 ml/kg/day. 100 ml/kg/day. 1000 ml plus 50 ml/kg for every kg over 10 kg. 1500 ml plus 20 ml/kg for every kg over 20 kg. EXAMPLES: Weight: 8 kg : 15 kg : 27 kg : Maintenance fluid 100 ml/kg/day = 800 ml/day 1000 ml + (50 ml/kg * 5) = 1000 + 250 = 1250 ml/day 1500 ml + (20 ml/kg * 7) = 1500 + 140 = 1640 ml/day 3. Factors which may increase insensible water loss will increase daily fluid requirements. a. Estimates of additional insensible water loss (e.g., fever) can be calculated as a percent increase of normal maintenance fluids (e.g. for fever, increase daily fluid by 12% of normal maintenance for every degree Centigrade over 37 degrees). b. Neonates who receive phototherapy require 20 ml/kg/day additional fluid due to increased insensible water loss. B. Fluid deficit is calculated by clinical assessment of dehydration. Clinical Signs Thirst Mild slight alert, Behavior restless Mucous membrane normal Tears present 88 Degree of dehydration Moderate moderate irritable to touch, may be lethargic dry +/- Severe intense hyperirritable to lethargic, may be comatose very dry absent Eyes Skin elasticity (pinch retracts) Skin color Anterior fontanelle Weight loss Fluid deficit normal immedi ately normal normal 3-5% 30-50 ml/kg sunken grossly sunken slowly very slowly > 2 seconds pale sunken 8 - 10 % mottled or gray very sunken 12 - 15 % 80-100 ml/kg 120-150 ml/kg NOTE: If the pediatric patient is hemodynamically stable, 1/2 of the fluid deficit is replaced over the first 8 hours, and the second 1/2 of the fluid deficit is replaced over the next 16 hours. C. Ongoing losses also need to be replaced. Estimates of sensible fluid losses can usually be easily measured (e.g., NG tube losses, vomiting, etc). D. Fluid restriction: As in adults, the amount of daily fluids administered to a pediatric patient may need to be restricted. Situations which require fluid restriction include patients with cerebral edema, congestive heart failure, renal failure, SIADH, patent ductus arteriosus, and certain pulmonary disorders. Fluid restriction may be calculated 1) as a percent of maintenance fluids (e.g., 2/3 or 3/4 maintenance) or 2) as insensible loss (300 - 400 ml/m2) plus urine output. II. Pediatric Total Parenteral Nutrition (TPN) A. The indications for TPN in children are similar to the indications in adults, i.e., if the G.I. tract cannot be used as a route of administration for nutrition, then parenteral nutrition may be indicated. One big difference vs adults is that due to fewer body stores and a higher caloric daily requirement, children are started on hyperalimentation sooner than adults. Generally, the smaller or younger the child is, the sooner (s)he needs appropriate nutritional intake. Indications: 1. Congenital or acquired anomalies if the G.I. tract: gastroschisis, bowel fistulas, intestinal obstruction, atresias, short gut syndrome. NOTE: "Short gut syndrome" or "short bowel syndrome" is a condition which is present after a significant amount of intestine has been surgically removed. Often these patients are dependent upon lifetime parenteral nutrition. 2. Chronic or recurrent diarrhea: malabsorption syndrome, inflammatory bowel disease. 89 3. Malnutrition (i.e. TPN as a supplement in certain diseases in which adequate caloric intake is not being achieved via the oral route: cystic fibrosis, cancer, anorexia nervosa, hypermetabolic states, e.g., burns). 4. Patient who are NPO (or who will be NPO) for sufficient periods of time to cause a significant decrease in caloric intake (e.g., post-operative patients). B. Pediatric Parenteral Nutrition Practice Guidelines (from the American Society for Parenteral and Enteral Nutrition1): 1. Patients who are candidates for parenteral nutrition support are those requiring nonvolitional feeding who are either already malnourished or are at risk of developing malnutrition. 2. Peripheral parenteral nutrition should be used to provide partial or total nutrition for up to 2 weeks in patients who cannot ingest or absorb oral or enterally delivered nutrients, or when central vein parenteral nutrition is not feasible. 3. Peripheral parenteral nutrition may be used for short-term (less than 2 weeks) maintenance, supplemental nutrition, or repletion nutrition support in some older infants and children who are not fluid restricted. 4. Central intravenous nutrition support should be used in patients who do not tolerate enteral nutrition support or in whom peripheral access is limited, parenteral support will last longer than 2 weeks, nutrient needs cannot be met by peripheral parenteral nutrition, or fluid restriction is required. C. Monitoring: In order to assure that TPN is meeting the nutritional goals, growth parameters (i.e., weight, height, head circumference) need to be assessed periodically. Monitoring of specific laboratory parameters assures adequate intake and decreases the complications of TPN. (See required reading: Table 108.11, Suggested monitoring schedule during pediatric TPN) D. Fluid Calculations 1. Initial: The actual volume of TPN (hyperalimentation plus intralipid) to be given is calculated by subtracting the volume of the patient's other necessary fluids (e.g., continuous dopamine infusions, arterial lines, etc.) from the total daily fluid requirement. In patients who are not fluid restricted, who do not 90 have fluid deficits or ongoing abnormal losses, and who do not receive other fluids, TPN is usually started at normal daily maintenance fluids. 2. Advancement of TPN fluid: In order to provide an adequate amount of calories for normal growth and development, the daily total fluid volume will need to exceed the daily normal maintenance fluid requirements. a. Precautions: Congestive heart failure can easily be produced in a pediatric patient, if fluids are advanced too rapidly or too much fluid is given per day. Daily fluids should be increased according to the following guidelines and patients need to be monitored for signs/symptoms of fluid overload, edema, and CHF. b. For infants < 10 kg the initial daily fluid volume may be increased (if tolerated) by 10 ml/kg/day until the desired caloric intake is achieved. The maximum amount of fluid (if tolerated) is 200 ml/kg/day. c. For infants > 10 kg, the initial daily fluid volume may be increased by 10% of the initial volume per day (if tolerated) until the desired caloric intake is achieved. The maximum amount of fluid (if tolerated) is 4000 ml/m2/day). E. Caloric Requirements: The goal of TPN is to provide adequate calories and nutrients for proper growth and development of the child. Proper growth of the child is determined by maintenance of the child's respective growth percentile for age and gender. For example, if an infant is 75th percentile for height and weight at age 3 months, then the goal is to maintain the 75th percentile for height and weight at older ages (i.e. as the child gets older, (s)he should be following the 75th percentile growth curves). 1. Caloric requirements per kg are greater in infants compared to children and adults. Children also require more calories per Kg than adults. These increases in caloric requirements are due to increases in cellular growth and physical activity, as well as an increased heat loss (due to the larger surface area per body weight seen in infants and children vs adults). TPN caloric requirements2 91 AGE (yrs) Kcal/kg/day 0-1 1-7 7 - 12 90 - 120 75 - 90 60 - 75 2. Factors that increase caloric requirements: Similar to adults, certain factors will increase daily caloric requirements in children. FACTOR INCREASE IN CALORIC NEED2 Fever 10 - 12 % for each degree > 37o C Cardiac failure Major surgery Burns Severe sepsis Long term growth failure 15 - 25 % 20 - 30 % up to 100 % 40 - 50 % 50 - 100 % NOTE: Infants with protein calorie malnutrition may require 150 - 175 Kcal/kg/day for growth. F. Carbohydrates: As in adults, pediatric patients are NOT started on TPN with the highest amount of dextrose required to give adequate calories. Carbohydrates are started at a lower amount and advanced in a stepwise fashion to allow an appropriate response of the pancreas. This stepwise advancement allows the pancreas to adjust to the higher amounts of dextrose given by secreting larger amounts of endogenous insulin. Hyperglycemia, glucosuria and osmotic diuresis are thus prevented. (NOTE: Dextrose = 3.4 Kcal/gram) 1. Carbohydrate intake must be calculated for newborns and the very low birth weight premature infant in terms of gm/kg/day or mg/kg/min. a. Preterm infants < 1 kg 1. Initial: 3 - 5 mg/kg/minute (Homeostasis) 2. Advance by: 0.5 - 1 mg/kg/minute per day b. Term newborns and older infants 1. Initial: 7 - 8 mg/kg/minute 2. Advance by: 2 - 4 mg/kg/minute per day c. Infants: Usual maximum rate of infusion: 18 - 20 mg/kg/minute d. Children: Usually require 6 - 9 mg/kg/minute 92 2. Practical guidelines: Recommendations according to percent dextrose: Serum and urine glucose must be monitored as some patients may not tolerate these increases. These patients (usually preterm infants) will require other percent concentrations of dextrose, e.g., 6%, 7% etc. Patient Age Group Initial concentration Advance by Premature infants Newborn infants 5 % Dextrose Older infants 5 % Dextrose 2.5 % Dextrose every other day 2.5 % Dextrose per day 5 % Dextrose per day Children Teenagers 5 % Dextrose Adults NOTE: Premature and newborn infants are more likely to become hypoglycemic if the dextrose solution is suddenly discontinued. Serum dextrose must be monitored if TPN discontinued. Excess carbohydrates (in comparison to protein and fats) may result in fatty infiltrates of the liver and an increase in pCO2 on blood gas. 3. Maximum dextrose concentrations for infants and children a. Peripheral: 10%. Concentrations above 10% are associated with an increase in phlebitis and a decreased duration of use of the peripheral line. The peripheral use of 12.5% dextrose containing TPN is discouraged however, 12.5% dextrose containing TPN is sometimes used in patients who require higher calories or who are fluid restricted. Close supervision of the IV site then becomes mandatory (e.g., direct nursing care, ICU care). b. Central: 20 - 25 %. The rapid dilution of TPN solutions with the larger quantities of blood in central veins, allows for solutions with higher final osmolalities to be used centrally (i.e., higher concentrations of dextrose). Typically, dextrose concentrations up to 20 % are used centrally. TPN with 25 % dextrose is usually reserved for severely malnourished patients. Occasionally, concentrations greater than 25% (i.e. 30 - 35 %) have been used in older infants and children who are severely fluid restricted. 93 G. Protein Requirements: Pediatric patients require a greater amount of protein per kilogram per day compared to adults. Again, this is due to their increased growth rates.3 Age group Premature neonates and infants Greater than 1 year of age Adolescents & adults Daily amount of parenteral protein to promote nitrogen retention 2.5 - 3 grams/kg/day 1.5 - 2 grams/kg/day 1 - 1.5 grams/kg/day 1. Initiation and Advancement: Similar to carbohydrates, pediatric patients are NOT started at the daily amount of protein to promote nitrogen retention. Again, patients are started on lower amounts of protein and advanced in a stepwise fashion. a. Neonates: Start with 0.5 - 1 gram/kg/day of protein and advance daily by 0.5 gm/kg/day. b. Older infants and children: Start with 1 gram/kg/day and advance daily by 0.5 - 1 gm/kg/day. Neonates receiving standard adult amino acid formulations were found to have elevated plasma concentrations of methionine, phenylalanine and glycine as well as decreased concentrations of tyrosine, cysteine and taurine compared to normal breast fed infants. Two amino acid formulations have been designed to meet the special amino acid requirements in neonates and young infants. TrophamineR and Aminosyn-PFR contain less methionine, phenylalanine and glycine than adult formulations. Both also contain taurine, tyrosine, and histidine. L- Cysteine HCL must be added at the time of TPN preparation due to its instability in solution for prolonged periods. NOTE: When using TrophamineR, 40 mg of cysteine HCL is added to the TPN for every one gram of protein. Since cysteine HCL comes as a HCL salt, one mmol of acetate or lactate is added to the TPN for every mmol (160 mg) of cysteine HCL. This acetate or lactate is added to balance the HCL load and prevent a metabolic acidosis which can be produced in premature and young infants. (Remember that bicarbonate results from acetate and lactate via the Kreb's cycle.) Studies have shown that neonates receiving TPN utilizing TrophamineR had "normal" amino acid patterns i.e., patterns that were similar to breast fed infants. Significantly greater weight gain and nitrogen balance were seen in infants were given Trophamine compared to adult amino acid formulations. 94 Further studies in neonates comparing Aminosyn-PFR and TrophamineR are needed. 4. Nonprotein calorie to gram nitrogen ratio: If an improper amount of nonprotein calorie to gram nitrogen ratio is given to a patient, (s)he will utilize proteins as a caloric source rather than for anabolic processes (i.e, as building blocks for cell growth). The optimal nonprotein calorie to gram nitrogen ratio in pediatric patients is not well defined. In the past, a nonprotein calorie to gram nitrogen ratio of 150 -200: 1 was suggested for adults. However, it is now realized that the ideal nonprotein calorie to gram nitrogen ratio differs with age and severity of illness. For critically ill infants and children, a nonprotein calorie to gram nitrogen ratio of 240 - 350: 1 has been suggested for proper utilization of amino acids. Remember: Grams of protein / 6.25 = nitrogen content in grams 5. Caloric density: 4 Kcal/gram. Since it is not optimal to use protein as a caloric source, the protein caloric content of hyperalimentation fluids is generally not calculated. H. Lipids: Lipids are administered as part of TPN to prevent or reverse an essential fatty acid deficiency and to provide a concentrated iso-osmotic source of calories. 1. Essential fatty acid deficiency: a. Both linoleic acid and linolenic acid are thought to be essential. b. The premature infant may develop biochemical evidence of essential fatty acid deficiency in as little as 2 days, due to limited fat stores. c. Provision of 2 - 4 % of the required total daily calories as IV fat emulsion or approximately 0.5 - 1 gram/kg/day will prevent clinical signs and symptoms of essential fatty acid deficiency. d. Signs of essential fatty acid deficiency include reduced growth, decreased platelets, impaired wound healing, dry scaly skin and sparse hair. e. Biochemical evidence of essential fatty acid deficiency includes a triene:tetraene ratio greater than 0.4. 2. Lipid Metabolism: a. Importance of Vitamin E: Lipid metabolism results in lipid peroxidation and free radical formation. Free radicals can damage cell membranes if Vitamin E is deficient. (Vitamin E acts as a free radical 95 scavenger.) Lipid emulsions do contain a small amount of Vitamin E, however, supplementation with MVI is recommended, especially in infants. In order to prevent peroxidative injury, a vitamin E : polyunsaturated fatty acid (PUFA) ratio of > 0.6 mg/g is needed. b. Decreased lipoprotein lipase activity: Lipoprotein lipase hydrolyzes fat particles to free fatty acids and monoglycerides. Both premature and term newborns have low lipoprotein lipase activity compared to adults. This results in a reduced lipid clearance rate. Hypertriglyceridemia / hyperlipidemia (fat intolerance) occurs when the rate of infusion of the fat emulsion exceeds the plasma lipid clearance rate. Premature infants, small for gestational age infants (regardless of gestational age) and nutritionally depleted older children are at risk for hypertriglyceridemia. Due to decreased fat clearance, lipid infusions for these patients should be administered over 24 hours. NOTE: In infants and children, IntralipidR is typically infused over 18 24 hours. c. Decreased metabolism of glycerol and free fatty acids: Plasma lipid clearance is also decreased in neonates due to their decreased metabolism of free fatty acids and glycerol. Carnitine facilitates the transport of free fatty acids across the mitochondrial membranes to the site of fat oxidation. Premature neonates and newborns have limited carnitine stores which can decrease the proper utilization of free fatty acids. 3. Lipid emulsion dosing guidelines 2,3 Initial dose Advance by Maximum dose Premature or SGA Full term or AGA Older children 0.5 gm/kg/day 1 gm/kg/day 0.25 gm/kg/day or 0.5 gm/kg/day every other day 3 gm/kg/day 3 - 4 gm/kg/day 1 gm/kg/day 0.5 gm/kg/day 2 - 3 gm/kg/day 4. Serum triglycerides should be monitored before every (or every other) increase in lipid emulsion, especially in premature infants and routinely thereafter. If triglyceride levels are less than 200 mg/dl the patient can be maintained on her/his present dose.3 5. Caloric Content: Fats are usually considered to contain 9 kcal/gram. Due to emulsifying agents and other additives, IntralipidR 10% = 1.1 kcal/ml and IntralipidR 20% = 2 kcal/ml. Usually 25 - 40 percent of the total calories are provided by lipids but no more than 60 percent of total calories should be provided by lipids. 96 6. Hypersensitivity reactions including allergic reactions, fever, chills, shivering, cyanosis, flushing, nausea, vomiting, headache, dizziness, or chest and back pain have been reported due to the egg phospholipids which are used to emulsify fat emulsions. Patients should be monitored for these immediate adverse reactions. 7. Controversies a. Hyperbilirubinemia: Free fatty acids, which displace bilirubin from albumin binding sites, may cause an increase in the concentration of unconjugated bilirubin and increase the risk of kernicterus. Decreased amounts of fat emulsion (0.5 - 1 gm/kg/day i.e., just enough to prevent essential fatty acid deficiency) are usually given to neonates with elevated bilirubin concentrations. These decreased amount of lipids are usually given when total bilirubin concentrations are greater than onehalf that required for exchange transfusion. b. Pulmonary compromise: In patients with pulmonary compromise, lipid emulsions may decrease pulmonary diffusion capacity with a resultant decrease in PO2. These effects were observed when large amounts of fat emulsion were administered over short periods of time. The risk is decreased if lipids are infused over 24 hrs. c. Heparin stimulates the release of lipoprotein lipase and has been postulated to be effective in reducing serum triglyceride concentrations in neonates receiving lipid emulsions. Further studies are needed before routine use of heparin can be recommended. NOTE: Heparin is routinely used in TPN at a final concentration of 1 unit/ml to decrease thrombus formation at the central catheter tip, and to increase the duration of patency of peripheral hyperalimentation lines. (see required text reading) I. Electrolytes and minerals 1. Requirements: Unless the patient has an electrolyte abnormality, start with the recommended daily amount and adjust according to serum chemistries. Element Sodium Potassium Chloride Magnesium Calcium Gluconate Phosphorus 97 Daily requirement (infants and children) 2 - 4 mEq/kg 2 - 3 mEq/kg 2 - 3 mEq/kg 0.25 - 0.5 mEq/kg 100 - 500 mg/kg 1 - 2 mmol/kg Comments: Sodium: Premature neonates may require higher daily amounts. Magnesium: Do not routinely add magnesium in the TPN for infants whose mothers have received therapeutic dose of magnesium (i.e. for tocolysis or prophylaxis against eclampsia). Check magnesium serum concentration first. Magnesium may be added if serum magnesium is not elevated. Calcium Gluconate: Usually, the higher amounts listed are needed in premature newborns and neonates (300 - 500 mg/kg/day), while the lower amounts are recommended for older infants (200 mg/kg/day) and toddlers (100 mg/kg/day). Older children may require only 1 - 2 grams per day of calcium gluconate. Phosphorous: Older infants and children will require less phosphorous (0.5 mmol/kg/day) than premature infants and newborns (up to 2 mmol/kg/day). Potassium phosphate = 0.68 mmol phosphate per mEq Sodium phosphate = 0.75 mmol phosphate per mEq 2. Calcium and Phosphate Compatibility Since premature newborns, neonates, and young infants require a greater amount of calcium and phosphorus compared to adults, calcium / phosphate compatibility in hyperalimentation fluid is an important issue. Many times the amount of calcium and phosphorous that these patients require is greater than the solubility and calcium-phosphate can precipitate. Many factors effect the solubility of calcium with phosphate in hyperalimentation solutions. Specific texts (e.g., Trissel's Handbook on Injectable Drugs) and solubility curves4 are utilized to determine if the amount of calcium and phosphate ordered in a hyperalimentation will precipitate. 2. Calcium and Phosphate Compatibility Factors which effect calcium and phosphorous solubility include: a. Concentration of calcium and phosphorous b. Salt form of calcium c. Concentration of amino acids d. Type of amino acid solution e. Concentration od dextrose 98 f. Addition of cysteine (effects pH) J. Vitamin requirements 1. MVI PediatricR provides the American Medical Association Nutrition Advisory Group (AMA-NAG) requirements for infants greater than 10 kg until 11 yrs of age. (See table 7 below) 5 2. Unlike the adult MVIR product, the pediatric product contains Vitamin K. 3. FDA recommendations for MVI PediatricR: Infants < 1 kg 30 % of a vial (1.5 ml) Infants 1 - 3 kg 65 % of a vial (3.25 ml) Infants > 3 kg - 11 yrs 100% of a vial (5 ml) 4. In premature infants, the above FDA recommendations may not be adequate for certain vitamins (vitamin A and E) and may result in higher serum concentrations of water soluble vitamins (e.g., ascorbic acid). 99 K. Trace elements requirements: 6 1. Trace elements should be given to premature infants upon initiation of TPN and to term neonates and infants who will receive TPN for > 2 weeks. 2. Copper, zinc, chromium, and manganese available as combination products: EXAMPLES: Trace element content per 1 ml: PTE-4 Pedtrace Neotrace Zinc 1 mg 0.5 mg 1.5 mg Copper 0.1 mg 0.1 mg 0.1 mg Manganese 25 mcg 25 mcg 25 mcg Chromium 1 mcg 0.85 mcg 0.85 mcg The usual dose of these products is 0.2 ml/kg/day. Please note the big difference in zinc concentrations in these products. Neotrace has the highest amount of zinc and (just as the name implies) is intended for use in neonates. PTE-4 and Pedtrace have less zinc than neotrace and are intended for use in infants and children whose zinc requirements are less than neonates. If PTE-4 or Pedtrace is used in neonates, additional zinc must be given in order for the neonate to receive the total daily recommended amount. Children > 40 50 Kg should use the adult trace element formulations (e.g., Multitrace). 3. Selenium 2 - 3 mcg/kg/day up to daily maximum of 30 - 40 mcg also needs to be added to the TPN. 4. Iodine a. Absorbed from topical povidone iodine solution or ointment, so no need to add to TPN. b. Thyroid profile monitoring recommended for long term TPN. 5. Iron a. IV iron dextran is recommended for infants > 2 months of age receiving TPN for > 1 month. Preterm infants < 2 months of age may experience hemolysis after given IV iron dextran. b. If iron is added to the hyperalimentation daily (controversial) the dose is 0.1 - 0.2 mg/kg/day. 100 c. For monthly IV replacements of iron: calculate iron needs by the following equation and administer the dose over 3 days. (Maximum daily dose = 25 mg). Body weight (pounds) x (100 - % Hgb) x 0.3 = mg of elemental iron 6. Disease states which alter trace element requirements: a. Increased losses: In diarrhea states or excess G.I. fistula losses extra zinc may be needed. b. Decreased elimination: 1. Cholestasis (obstructive jaundice): Eliminate copper and manganese from TPN 2. Renal failure: Eliminate Cr and Se from TPN NOTE: Some clinicians may eliminate Zn or decrease the daily amount. L. Complications associated with TPN include infectious, mechanical, metabolic and other problems such as cholestasis and rickets: (see Table 9-27) 6. For further discussion of the cns of TPN see requred reading text. 1. Infection: The most common organisms to cause sepsis in TPN patients are Staphylococcus epidermidis and Staph aureus. Other common bacteria include: Streptococcus, gram-negative organisms and Candida. Catheter site infections also occur. 2. Mechanical: One of the many mechanical problems with central TPN is thrombus formation. Urokinase (5,000 units/ml) may be used in children to lyse clots in catheters. When using urokinase to lyse a catheter thrombus, it is important to "treat the clot and not the patient" i.e., urokinase should NOT be injected past the catheter into the patient. The internal volume (ml) of the patient's central catheter must be known and only that same amount of urokinase used. Also, after allowing the urokinase to sit in the catheter and dissolve the clot, the urokinase should be withdrawn from the catheter. It should not be administered systemically to the patient. NOTE: The amount of urokinase that is used in adults to clear a catheter can have systemic effects in small infants if inadvertently administered through the catheter and not drawn back as required. 101 3. TPN cholestasis can occur in pediatric patients, usually after about 2 weeks of TPN. Premature infants and those receiving > 2.5 gm/kg/day of protein have a higher incidence of liver dysfunction. Other factors which may increase the incidence of TPN cholestasis include: sepsis, fasting (being NPO), and calorie overload. Discontinuation of TPN will usually reverse liver dysfunction. If TPN cannot be discontinued, TPN cholestasis may be managed by the following: a. Give the appropriate type and amino acids and reduce the amino acid load. b. Give the appropriate amount of calories (i.e. give an adequate but not an excessive amount). c. Cyclic hyperalimentation (i.e., cycling the patient off of hyperalimentation for part of the day): Pediatric precautions: Infants more often than older children and adolescents may not be able to tolerate infusion periods less than 12 hours/day. Intolerance is usually due to inability to handle the higher ml/hr rates of fluid volume or nutrients that are given over the shorter period of time (i.e., the total daily amount of fluid and nutrients may be given over < 24 hours time, this results in a higher ml/hour rate). d. Stimulate the gut with minimal enteral feeds. M. Heparin: As previously mentioned, heparin 1 unit per ml (final volume) of hyperalimentation solution is often used in the pediatric population, both in central and peripheral TPN. Therapeutic doses of heparin may be approached with extremely high hyperalimentation rates or with frequent heparin flushes. (Maintenance doses of heparin are considered to be 10 - 25 units/kg per hour.) Therefore, a reduction from the usual 1 unit/ml of heparin in the hyperal to 0.5 units/ml may be needed especially in small infants requiring larger volumes of fluid. 102 Goal: To familiarize students with the differences in nutritional requirements between adults and children with respect to fluids, electrolytes, calories, carbohydrates, proteins, fats and trace elements. Introduction: Adequate nutrition for the proper growth and development of a child requires individualization. The amount and type of fluid, calories, electrolytes, and trace elements are all based on age, weight, nutritional status, and disease state. I. The total daily fluid requirement of any patient is equal to the normal daily maintenance fluids plus replacement of any fluid deficit plus replacement of any significant abnormal ongoing losses. Two methods to calculate normal maintenance fluids are described below. Normal maintenance fluids provide replacement for normal body functions and for normal losses (for example, insensible water loss, urine output and stool losses). Other factors that may increase the patient's total daily fluid requirements need to be replaced in addition to the normal daily maintenance fluids. Total daily fluid requirement = Normal Maintenance Fluids + Deficit + Ongoing Abnormal Losses Total daily fluid requirements may be increased by: 4) increases in insensible water losses due to such factors as fever, hyperventilation, phototherapy, radiant warming, skin breakdown, burns, etc. 5) initial deficits of fluid i.e., dehydration 6) significant ongoing abnormal losses such as diarrhea, vomiting, nasogastric tube losses, high output renal failure, etc. A. Daily maintenance fluid requirements (i.e., normal maintenance fluids) are those required to maintain normal homeostasis for a 24 hour period. Surface area and body weight are two common methods used for the calculation of maintenance fluids in pediatric patients. NOTE: Premature infants will have greater daily maintenance fluid requirements then those shown here due to their larger surface area to body weight ratio and thinner skin, both of which significantly increase their insensible water losses from the skin. In fact, preterm infants < 750 grams often require 200 - 250 ml/kg/day to prevent dehydration. Due to their highly specialized needs, calculation of fluid requirements for premature neonates will be considered beyond the scope of this lecture. 103 1. Daily maintenance fluid requirements calculated by body surface area: For pediatric patients, the amount of daily maintenance fluid required is in the range of 1500 - 1800 ml/m2/day. Usually 1500 ml/m2/day is used. The surface area method is usually used in children > 10 kilograms because a precise measurement of surface area is often difficult in smaller infants. 2. Daily maintenance fluid requirements calculated by body weight Weight < 2.5 kg 2.5 - 10 kg 11 - 20 kg > 20 kg Daily maintenance fluid requirements 120 ml/kg/day. 100 ml/kg/day. 1000 ml plus 50 ml/kg for every kg over 10 kg. 1500 ml plus 20 ml/kg for every kg over 20 kg. EXAMPLES: Weight: 8 kg : 15 kg : 27 kg : Maintenance fluid 100 ml/kg/day = 800 ml/day 1000 ml + (50 ml/kg * 5) = 1000 + 250 = 1250 ml/day 1500 ml + (20 ml/kg * 7) = 1500 + 140 = 1640 ml/day 3. Factors which may increase insensible water loss will increase daily fluid requirements. a. Estimates of additional insensible water loss (e.g., fever) can be calculated as a percent increase of normal maintenance fluids (e.g. for fever, increase daily fluid by 12% of normal maintenance for every degree Centigrade over 37 degrees). b. Neonates who receive phototherapy require 20 ml/kg/day additional fluid due to increased insensible water loss. B. Fluid deficit is calculated by clinical assessment of dehydration. Clinical Signs Thirst Mild slight alert, Behavior restless Mucous membrane normal Tears present Eyes normal Skin elasticity immedi (pinch retracts) ately 104 Degree of dehydration Moderate moderate irritable to touch, may be lethargic dry +/sunken Severe intense hyperirritable to lethargic, may be comatose very dry absent grossly sunken slowly very slowly > 2 seconds Skin color normal Anterior fontanelle normal Weight loss 3-5% 30-50 Fluid deficit ml/kg pale sunken 8 - 10 % mottled or gray very sunken 12 - 15 % 80-100 ml/kg 120-150 ml/kg NOTE: If the pediatric patient is hemodynamically stable, 1/2 of the fluid deficit is replaced over the first 8 hours, and the second 1/2 of the fluid deficit is replaced over the next 16 hours. C. Ongoing losses also need to be replaced. Estimates of sensible fluid losses can usually be easily measured (e.g., NG tube losses, vomiting, etc). D. Fluid restriction: As in adults, the amount of daily fluids administered to a pediatric patient may need to be restricted. Situations which require fluid restriction include patients with cerebral edema, congestive heart failure, renal failure, SIADH, patent ductus arteriosus, and certain pulmonary disorders. Fluid restriction may be calculated 1) as a percent of maintenance fluids (e.g., 2/3 or 3/4 maintenance) or 2) as insensible loss (300 - 400 ml/m2) plus urine output. II. Pediatric Total Parenteral Nutrition (TPN) A. The indications for TPN in children are similar to the indications in adults, i.e., if the G.I. tract cannot be used as a route of administration for nutrition, then parenteral nutrition may be indicated. One big difference vs adults is that due to fewer body stores and a higher caloric daily requirement, children are started on hyperalimentation sooner than adults. Generally, the smaller or younger the child is, the sooner (s)he needs appropriate nutritional intake. Indications: 1. Congenital or acquired anomalies if the G.I. tract: gastroschisis, bowel fistulas, intestinal obstruction, atresias, short gut syndrome. NOTE: "Short gut syndrome" or "short bowel syndrome" is a condition which is present after a significant amount of intestine has been surgically removed. Often these patients are dependent upon lifetime parenteral nutrition. 2. Chronic or recurrent diarrhea: malabsorption syndrome, inflammatory bowel disease. 105 3. Malnutrition (i.e. TPN as a supplement in certain diseases in which adequate caloric intake is not being achieved via the oral route: cystic fibrosis, cancer, anorexia nervosa, hypermetabolic states, e.g., burns). 4. Patient who are NPO (or who will be NPO) for sufficient periods of time to cause a significant decrease in caloric intake (e.g., post-operative patients). B. Pediatric Parenteral Nutrition Practice Guidelines (from the American Society for Parenteral and Enteral Nutrition1): 1. Patients who are candidates for parenteral nutrition support are those requiring nonvolitional feeding who are either already malnourished or are at risk of developing malnutrition. 2. Peripheral parenteral nutrition should be used to provide partial or total nutrition for up to 2 weeks in patients who cannot ingest or absorb oral or enterally delivered nutrients, or when central vein parenteral nutrition is not feasible. 3. Peripheral parenteral nutrition may be used for short-term (less than 2 weeks) maintenance, supplemental nutrition, or repletion nutrition support in some older infants and children who are not fluid restricted. 4. Central intravenous nutrition support should be used in patients who do not tolerate enteral nutrition support or in whom peripheral access is limited, parenteral support will last longer than 2 weeks, nutrient needs cannot be met by peripheral parenteral nutrition, or fluid restriction is required. C. Monitoring: In order to assure that TPN is meeting the nutritional goals, growth parameters (i.e., weight, height, head circumference) need to be assessed periodically. Monitoring of specific laboratory parameters assures adequate intake and decreases the complications of TPN. (See required reading: Table 108.11, Suggested monitoring schedule during pediatric TPN) D. Fluid Calculations 1. Initial: The actual volume of TPN (hyperalimentation plus intralipid) to be given is calculated by subtracting the volume of the patient's other necessary fluids (e.g., continuous dopamine infusions, arterial lines, etc.) from the total daily fluid requirement. In patients who are not fluid restricted, who do not have fluid deficits or ongoing abnormal losses, and who do not receive other fluids, TPN is usually started at normal daily maintenance fluids. 106 2. Advancement of TPN fluid: In order to provide an adequate amount of calories for normal growth and development, the daily total fluid volume will need to exceed the daily normal maintenance fluid requirements. a. Precautions: Congestive heart failure can easily be produced in a pediatric patient, if fluids are advanced too rapidly or too much fluid is given per day. Daily fluids should be increased according to the following guidelines and patients need to be monitored for signs/symptoms of fluid overload, edema, and CHF. b. For infants < 10 kg the initial daily fluid volume may be increased (if tolerated) by 10 ml/kg/day until the desired caloric intake is achieved. The maximum amount of fluid (if tolerated) is 200 ml/kg/day. c. For infants > 10 kg, the initial daily fluid volume may be increased by 10% of the initial volume per day (if tolerated) until the desired caloric intake is achieved. The maximum amount of fluid (if tolerated) is 4000 ml/m2/day). E. Caloric Requirements: The goal of TPN is to provide adequate calories and nutrients for proper growth and development of the child. Proper growth of the child is determined by maintenance of the child's respective growth percentile for age and gender. For example, if an infant is 75th percentile for height and weight at age 3 months, then the goal is to maintain the 75th percentile for height and weight at older ages (i.e. as the child gets older, (s)he should be following the 75th percentile growth curves). 2. Caloric requirements per kg are greater in infants compared to children and adults. Children also require more calories per Kg than adults. These increases in caloric requirements are due to increases in cellular growth and physical activity, as well as an increased heat loss (due to the larger surface area per body weight seen in infants and children vs adults). TPN caloric requirements2 107 AGE (yrs) Kcal/kg/day 0-1 1-7 7 - 12 90 - 120 75 - 90 60 - 75 2. Factors that increase caloric requirements: Similar to adults, certain factors will increase daily caloric requirements in children. FACTOR INCREASE IN CALORIC NEED2 Fever 10 - 12 % for each degree > 37o C Cardiac failure Major surgery Burns Severe sepsis Long term growth failure 15 - 25 % 20 - 30 % up to 100 % 40 - 50 % 50 - 100 % NOTE: Infants with protein calorie malnutrition may require 150 - 175 Kcal/kg/day for growth. F. Carbohydrates: As in adults, pediatric patients are NOT started on TPN with the highest amount of dextrose required to give adequate calories. Carbohydrates are started at a lower amount and advanced in a stepwise fashion to allow an appropriate response of the pancreas. This stepwise advancement allows the pancreas to adjust to the higher amounts of dextrose given by secreting larger amounts of endogenous insulin. Hyperglycemia, glucosuria and osmotic diuresis are thus prevented. (NOTE: Dextrose = 3.4 Kcal/gram) 1. Carbohydrate intake must be calculated for newborns and the very low birth weight premature infant in terms of gm/kg/day or mg/kg/min. a. Preterm infants < 1 kg 1. Initial: 3 - 5 mg/kg/minute (Homeostasis) 2. Advance by: 0.5 - 1 mg/kg/minute per day b. Term newborns and older infants 1. Initial: 7 - 8 mg/kg/minute 2. Advance by: 2 - 4 mg/kg/minute per day c. Infants: Usual maximum rate of infusion: 18 - 20 mg/kg/minute d. Children: Usually require 6 - 9 mg/kg/minute 108 2. Practical guidelines: Recommendations according to percent dextrose: Serum and urine glucose must be monitored as some patients may not tolerate these increases. These patients (usually preterm infants) will require other percent concentrations of dextrose, e.g., 6%, 7% etc. Patient Age Group Initial concentration Advance by Premature infants Newborn infants 5 % Dextrose Older infants 5 % Dextrose 2.5 % Dextrose every other day 2.5 % Dextrose per day 5 % Dextrose per day Children Teenagers 5 % Dextrose Adults NOTE: Premature and newborn infants are more likely to become hypoglycemic if the dextrose solution is suddenly discontinued. Serum dextrose must be monitored if TPN discontinued. Excess carbohydrates (in comparison to protein and fats) may result in fatty infiltrates of the liver and an increase in pCO2 on blood gas. 3. Maximum dextrose concentrations for infants and children a. Peripheral: 10%. Concentrations above 10% are associated with an increase in phlebitis and a decreased duration of use of the peripheral line. The peripheral use of 12.5% dextrose containing TPN is discouraged however, 12.5% dextrose containing TPN is sometimes used in patients who require higher calories or who are fluid restricted. Close supervision of the IV site then becomes mandatory (e.g., direct nursing care, ICU care). b. Central: 20 - 25 %. The rapid dilution of TPN solutions with the larger quantities of blood in central veins, allows for solutions with higher final osmolalities to be used centrally (i.e., higher concentrations of dextrose). Typically, dextrose concentrations up to 20 % are used centrally. TPN with 25 % dextrose is usually reserved for severely malnourished patients. Occasionally, concentrations greater than 25% (i.e. 30 - 35 %) have been used in older infants and children who are severely fluid restricted. G. Protein Requirements: Pediatric patients require a greater amount of protein per kilogram per day compared to adults. Again, this is due to their increased growth rates.3 109 Age group Premature neonates and infants Greater than 1 year of age Adolescents & adults Daily amount of parenteral protein to promote nitrogen retention 2.5 - 3 grams/kg/day 1.5 - 2 grams/kg/day 1 - 1.5 grams/kg/day 1. Initiation and Advancement: Similar to carbohydrates, pediatric patients are NOT started at the daily amount of protein to promote nitrogen retention. Again, patients are started on lower amounts of protein and advanced in a stepwise fashion. a. Neonates: Start with 0.5 - 1 gram/kg/day of protein and advance daily by 0.5 gm/kg/day. b. Older infants and children: Start with 1 gram/kg/day and advance daily by 0.5 - 1 gm/kg/day. Neonates receiving standard adult amino acid formulations were found to have elevated plasma concentrations of methionine, phenylalanine and glycine as well as decreased concentrations of tyrosine, cysteine and taurine compared to normal breast fed infants. Two amino acid formulations have been designed to meet the special amino acid requirements in neonates and young infants. TrophamineR and Aminosyn-PFR contain less methionine, phenylalanine and glycine than adult formulations. Both also contain taurine, tyrosine, and histidine. L- Cysteine HCL must be added at the time of TPN preparation due to its instability in solution for prolonged periods. NOTE: When using TrophamineR, 40 mg of cysteine HCL is added to the TPN for every one gram of protein. Since cysteine HCL comes as a HCL salt, one mmol of acetate or lactate is added to the TPN for every mmol (160 mg) of cysteine HCL. This acetate or lactate is added to balance the HCL load and prevent a metabolic acidosis which can be produced in premature and young infants. (Remember that bicarbonate results from acetate and lactate via the Kreb's cycle.) Studies have shown that neonates receiving TPN utilizing TrophamineR had "normal" amino acid patterns i.e., patterns that were similar to breast fed infants. Significantly greater weight gain and nitrogen balance were seen in infants were given Trophamine compared to adult amino acid formulations. Further studies in neonates comparing Aminosyn-PFR and TrophamineR are needed. 4. Nonprotein calorie to gram nitrogen ratio: If an improper amount of nonprotein calorie to gram nitrogen ratio is given to a patient, (s)he will utilize proteins as a caloric source rather than for anabolic processes (i.e, as building 110 blocks for cell growth). The optimal nonprotein calorie to gram nitrogen ratio in pediatric patients is not well defined. In the past, a nonprotein calorie to gram nitrogen ratio of 150 -200: 1 was suggested for adults. However, it is now realized that the ideal nonprotein calorie to gram nitrogen ratio differs with age and severity of illness. For critically ill infants and children, a nonprotein calorie to gram nitrogen ratio of 240 - 350: 1 has been suggested for proper utilization of amino acids. Remember: Grams of protein / 6.25 = nitrogen content in grams 5. Caloric density: 4 Kcal/gram. Since it is not optimal to use protein as a caloric source, the protein caloric content of hyperalimentation fluids is generally not calculated. H. Lipids: Lipids are administered as part of TPN to prevent or reverse an essential fatty acid deficiency and to provide a concentrated iso-osmotic source of calories. 1. Essential fatty acid deficiency: a. Both linoleic acid and linolenic acid are thought to be essential. b. The premature infant may develop biochemical evidence of essential fatty acid deficiency in as little as 2 days, due to limited fat stores. c. Provision of 2 - 4 % of the required total daily calories as IV fat emulsion or approximately 0.5 - 1 gram/kg/day will prevent clinical signs and symptoms of essential fatty acid deficiency. d. Signs of essential fatty acid deficiency include reduced growth, decreased platelets, impaired wound healing, dry scaly skin and sparse hair. e. Biochemical evidence of essential fatty acid deficiency includes a triene:tetraene ratio greater than 0.4. 2. Lipid Metabolism: a. Importance of Vitamin E: Lipid metabolism results in lipid peroxidation and free radical formation. Free radicals can damage cell membranes if Vitamin E is deficient. (Vitamin E acts as a free radical scavenger.) Lipid emulsions do contain a small amount of Vitamin E, however, supplementation with MVI is recommended, especially in infants. In order to prevent peroxidative injury, a vitamin E : polyunsaturated fatty acid (PUFA) ratio of > 0.6 mg/g is needed. 111 b. Decreased lipoprotein lipase activity: Lipoprotein lipase hydrolyzes fat particles to free fatty acids and monoglycerides. Both premature and term newborns have low lipoprotein lipase activity compared to adults. This results in a reduced lipid clearance rate. Hypertriglyceridemia / hyperlipidemia (fat intolerance) occurs when the rate of infusion of the fat emulsion exceeds the plasma lipid clearance rate. Premature infants, small for gestational age infants (regardless of gestational age) and nutritionally depleted older children are at risk for hypertriglyceridemia. Due to decreased fat clearance, lipid infusions for these patients should be administered over 24 hours. NOTE: In infants and children, IntralipidR is typically infused over 18 24 hours. c. Decreased metabolism of glycerol and free fatty acids: Plasma lipid clearance is also decreased in neonates due to their decreased metabolism of free fatty acids and glycerol. Carnitine facilitates the transport of free fatty acids across the mitochondrial membranes to the site of fat oxidation. Premature neonates and newborns have limited carnitine stores which can decrease the proper utilization of free fatty acids. 3. Lipid emulsion dosing guidelines 2,3 Initial dose Advance by Maximum dose Premature or SGA Full term or AGA Older children 0.5 gm/kg/day 1 gm/kg/day 0.25 gm/kg/day or 0.5 gm/kg/day every other day 3 gm/kg/day 3 - 4 gm/kg/day 1 gm/kg/day 0.5 gm/kg/day 2 - 3 gm/kg/day 4. Serum triglycerides should be monitored before every (or every other) increase in lipid emulsion, especially in premature infants and routinely thereafter. If triglyceride levels are less than 200 mg/dl the patient can be maintained on her/his present dose.3 5. Caloric Content: Fats are usually considered to contain 9 kcal/gram. Due to emulsifying agents and other additives, IntralipidR 10% = 1.1 kcal/ml and IntralipidR 20% = 2 kcal/ml. Usually 25 - 40 percent of the total calories are provided by lipids but no more than 60 percent of total calories should be provided by lipids. 6. Hypersensitivity reactions including allergic reactions, fever, chills, shivering, cyanosis, flushing, nausea, vomiting, headache, dizziness, or chest and back pain have been reported due to the egg phospholipids which are used 112 to emulsify fat emulsions. Patients should be monitored for these immediate adverse reactions. 7. Controversies a. Hyperbilirubinemia: Free fatty acids, which displace bilirubin from albumin binding sites, may cause an increase in the concentration of unconjugated bilirubin and increase the risk of kernicterus. Decreased amounts of fat emulsion (0.5 - 1 gm/kg/day i.e., just enough to prevent essential fatty acid deficiency) are usually given to neonates with elevated bilirubin concentrations. These decreased amount of lipids are usually given when total bilirubin concentrations are greater than onehalf that required for exchange transfusion. b. Pulmonary compromise: In patients with pulmonary compromise, lipid emulsions may decrease pulmonary diffusion capacity with a resultant decrease in PO2. These effects were observed when large amounts of fat emulsion were administered over short periods of time. The risk is decreased if lipids are infused over 24 hrs. c. Heparin stimulates the release of lipoprotein lipase and has been postulated to be effective in reducing serum triglyceride concentrations in neonates receiving lipid emulsions. Further studies are needed before routine use of heparin can be recommended. NOTE: Heparin is routinely used in TPN at a final concentration of 1 unit/ml to decrease thrombus formation at the central catheter tip, and to increase the duration of patency of peripheral hyperalimentation lines. (see required text reading) I. Electrolytes and minerals 1. Requirements: Unless the patient has an electrolyte abnormality, start with the recommended daily amount and adjust according to serum chemistries. Element Sodium Potassium Chloride Magnesium Calcium Gluconate Phosphorus 113 Daily requirement (infants and children) 2 - 4 mEq/kg 2 - 3 mEq/kg 2 - 3 mEq/kg 0.25 - 0.5 mEq/kg 100 - 500 mg/kg 1 - 2 mmol/kg Comments: Sodium: Premature neonates may require higher daily amounts. Magnesium: Do not routinely add magnesium in the TPN for infants whose mothers have received therapeutic dose of magnesium (i.e. for tocolysis or prophylaxis against eclampsia). Check magnesium serum concentration first. Magnesium may be added if serum magnesium is not elevated. Calcium Gluconate: Usually, the higher amounts listed are needed in premature newborns and neonates (300 - 500 mg/kg/day), while the lower amounts are recommended for older infants (200 mg/kg/day) and toddlers (100 mg/kg/day). Older children may require only 1 - 2 grams per day of calcium gluconate. Phosphorous: Older infants and children will require less phosphorous (0.5 mmol/kg/day) than premature infants and newborns (up to 2 mmol/kg/day). Potassium phosphate = 0.68 mmol phosphate per mEq Sodium phosphate = 0.75 mmol phosphate per mEq 2. Calcium and Phosphate Compatibility Since premature newborns, neonates, and young infants require a greater amount of calcium and phosphorus compared to adults, calcium / phosphate compatibility in hyperalimentation fluid is an important issue. Many times the amount of calcium and phosphorous that these patients require is greater than the solubility and calcium-phosphate can precipitate. Many factors effect the solubility of calcium with phosphate in hyperalimentation solutions. Specific texts (e.g., Trissel's Handbook on Injectable Drugs) and solubility curves4 are utilized to determine if the amount of calcium and phosphate ordered in a hyperalimentation will precipitate. 2. Calcium and Phosphate Compatibility Factors which effect calcium and phosphorous solubility include: a. Concentration of calcium and phosphorous b. Salt form of calcium c. Concentration of amino acids d. Type of amino acid solution e. Concentration od dextrose f. Addition of cysteine (effects pH) 114 J. Vitamin requirements 1. MVI PediatricR provides the American Medical Association Nutrition Advisory Group (AMA-NAG) requirements for infants greater than 10 kg until 11 yrs of age. (See table 7 below) 5 2. Unlike the adult MVIR product, the pediatric product contains Vitamin K. 3. FDA recommendations for MVI PediatricR: Infants < 1 kg 30 % of a vial (1.5 ml) Infants 1 - 3 kg 65 % of a vial (3.25 ml) Infants > 3 kg - 11 yrs 100% of a vial (5 ml) 4. In premature infants, the above FDA recommendations may not be adequate for certain vitamins (vitamin A and E) and may result in higher serum concentrations of water soluble vitamins (e.g., ascorbic acid). 115 K. Trace elements requirements: 6 1. Trace elements should be given to premature infants upon initiation of TPN and to term neonates and infants who will receive TPN for > 2 weeks. 2. Copper, zinc, chromium, and manganese available as combination products: EXAMPLES: Trace element content per 1 ml: PTE-4 Pedtrace Neotrace Zinc 1 mg 0.5 mg 1.5 mg Copper 0.1 mg 0.1 mg 0.1 mg Manganese 25 mcg 25 mcg 25 mcg Chromium 1 mcg 0.85 mcg 0.85 mcg The usual dose of these products is 0.2 ml/kg/day. Please note the big difference in zinc concentrations in these products. Neotrace has the highest amount of zinc and (just as the name implies) is intended for use in neonates. PTE-4 and Pedtrace have less zinc than neotrace and are intended for use in infants and children whose zinc requirements are less than neonates. If PTE-4 or Pedtrace is used in neonates, additional zinc must be given in order for the neonate to receive the total daily recommended amount. Children > 40 50 Kg should use the adult trace element formulations (e.g., Multitrace). 3. Selenium 2 - 3 mcg/kg/day up to daily maximum of 30 - 40 mcg also needs to be added to the TPN. 4. Iodine a. Absorbed from topical povidone iodine solution or ointment, so no need to add to TPN. b. Thyroid profile monitoring recommended for long term TPN. 5. Iron a. IV iron dextran is recommended for infants > 2 months of age receiving TPN for > 1 month. Preterm infants < 2 months of age may experience hemolysis after given IV iron dextran. b. If iron is added to the hyperalimentation daily (controversial) the dose is 0.1 - 0.2 mg/kg/day. c. For monthly IV replacements of iron: calculate iron needs by the following equation and administer the dose over 3 days. (Maximum daily dose = 25 mg). 116 Body weight (pounds) x (100 - % Hgb) x 0.3 = mg of elemental iron 6. Disease states which alter trace element requirements: a. Increased losses: In diarrhea states or excess G.I. fistula losses extra zinc may be needed. b. Decreased elimination: 1. Cholestasis (obstructive jaundice): Eliminate copper and manganese from TPN 2. Renal failure: Eliminate Cr and Se from TPN NOTE: Some clinicians may eliminate Zn or decrease the daily amount. L. Complications associated with TPN include infectious, mechanical, metabolic and other problems such as cholestasis and rickets: (see Table 9-27) 6. For further discussion of the cns of TPN see requred reading text. 1. Infection: The most common organisms to cause sepsis in TPN patients are Staphylococcus epidermidis and Staph aureus. Other common bacteria include: Streptococcus, gram-negative organisms and Candida. Catheter site infections also occur. 2. Mechanical: One of the many mechanical problems with central TPN is thrombus formation. Urokinase (5,000 units/ml) may be used in children to lyse clots in catheters. When using urokinase to lyse a catheter thrombus, it is important to "treat the clot and not the patient" i.e., urokinase should NOT be injected past the catheter into the patient. The internal volume (ml) of the patient's central catheter must be known and only that same amount of urokinase used. Also, after allowing the urokinase to sit in the catheter and dissolve the clot, the urokinase should be withdrawn from the catheter. It should not be administered systemically to the patient. NOTE: The amount of urokinase that is used in adults to clear a catheter can have systemic effects in small infants if inadvertently administered through the catheter and not drawn back as required. 3. TPN cholestasis can occur in pediatric patients, usually after about 2 weeks of TPN. Premature infants and those receiving > 2.5 gm/kg/day of protein have a higher incidence of liver dysfunction. Other factors which may 117 increase the incidence of TPN cholestasis include: sepsis, fasting (being NPO), and calorie overload. Discontinuation of TPN will usually reverse liver dysfunction. If TPN cannot be discontinued, TPN cholestasis may be managed by the following: a. Give the appropriate type and amino acids and reduce the amino acid load. b. Give the appropriate amount of calories (i.e. give an adequate but not an excessive amount). c. Cyclic hyperalimentation (i.e., cycling the patient off of hyperalimentation for part of the day): Pediatric precautions: Infants more often than older children and adolescents may not be able to tolerate infusion periods less than 12 hours/day. Intolerance is usually due to inability to handle the higher ml/hr rates of fluid volume or nutrients that are given over the shorter period of time (i.e., the total daily amount of fluid and nutrients may be given over < 24 hours time, this results in a higher ml/hour rate). d. Stimulate the gut with minimal enteral feeds. M. Heparin: As previously mentioned, heparin 1 unit per ml (final volume) of hyperalimentation solution is often used in the pediatric population, both in central and peripheral TPN. Therapeutic doses of heparin may be approached with extremely high hyperalimentation rates or with frequent heparin flushes. (Maintenance doses of heparin are considered to be 10 - 25 units/kg per hour.) Therefore, a reduction from the usual 1 unit/ml of heparin in the hyperal to 0.5 units/ml may be needed especially in small infants requiring larger volumes of fluid. 118