Autism - Moore County Schools
advertisement

Exceptional Children’s Program
Staff Handbook
Acknowledgements
The following people were instrumental in the development of this document.
Kevin Allen
Laura Dendy
Becky Benton
Cathy Jones
Trish Dutton
Judy Clendenin
Linda Tufts
Tina Kissell
Evelyn Seidenberg
Freda Alley
Mary Beth Jackson
Kassia Stubbs
Main Table of Contents
Administrative Information
Student Support Team Process
EC Referral Process
Categories of Eligibility
Forms Information and Directions
CECAS Information
Procedures
Behavior Management Information
Testing Information
Administrative Information
(back to top)
Administrative Table of Contents
Roles and Responsibilities
Staff List
Facilitator Description
Facilitator List
Important Dates
Roles and Responsibilities
Becky Benton
Director
Laura Dendy
Mary Beth
Jackson
Lizzie Garner
Kassia Stubbs
Traci Salazar
Elizabeth Sager Michele Denny
Neil Waters
Reading
Math
Preschool
Compliance
Behavior
CECAS
Finance
Speech
Surrogates
Transportation
Day Care
Licensure
Transition
FBA/BIP
Compliance
Purchase Orders
Aug Com
ESY
Testing
Child Find
OCS
PBIS
(back to TOC)
Check Requests
NCPK
Car Requests
Infant/Toddler
Transition
CEU info.
MOORE COUNTY
SCHOOLS EX ED
STAFF LIST 20092010
School
Aberdeen Elem.
Resource
Jane Beth Page
Tiffany White
Aberdeen Primary
Self-Contained
Melissa Kelso
Vacant
Teacher Assistants
Vacant
Tara Toomer
Speech/Lang.
Shuris Campbell
Amanda DelBrocco
Beth Turello (50%)
Kari Healey
Dorianne Kenn-Harris
Anna Harris
Victor Humphrey 1:1
Suzanne Johnson (Interpreter)
*Paulette Veloon
Cameron Elem.
Amber Morton
Denise Graner
Gay Williamson
Karen Gunter
* Lindsey Honey
Carthage Elem.
Karyn Greco
Jerry Cheek
Kimberly Pace
Martha Kidd
Cheryl Hines
Heidi Williams
Neil Waters
Amy Sehi
Kim Schwenkbeck
Susan Zucchino
Liz Jefferson
Angela McDougald
Wendy Martin
Lindsey Watkins
Sherry B. Lovell (FAC)
Udenia Icenhour
Racein Figueroa
Debra York
Ginny Hobgood
Nancy Marley
Ellen Ashwell
Tracy Cropley
Teresa Gibbons
Peggy Frye)
LeAnne Baker
Sheryl Bristow 1:1
Ginny Hobgood
Karen McCulloch
Lynn Pennington
Janet Flinchum
William Kennedy
Teresa Batalla
Crain’s Creek Middle
Elise Middle
Highfalls Elem.
New Century Middle
North Moore High
BED
Pam Brady
Carolyn Lambert
Jill Andrews
Christie Sparks
Sarah Bright
Leah Bartram
Beth Luck (OCS)
Pam Wallace (OCS)
Mike Vogt
Vacant
Jenny Wood
School
Community Learning
Center at Pinckney
Pinecrest High
Pinehurst Elem.
Robbins Elem.
Sandhills Farm Life Elem.
Resource
BED
Self- Contained
Sharon Turner
Shania Streter
Raymond Phile
Terry Kerr
School
Southern Middle
Speech/Lang
Lindsey Honey
Richard Koenig
Marianne Arthur (OCS)
Aja Toala
Rhonda Bullock
Vacant (OCS)
Fidericia Adams (OCS)
Kimberly Blevins-Franklin
Susie Oles
Susan Murden
Jayne Cummings
Kim Salmon
Josh Wilson
Barbara Rich
Betty Black
Gail Deese
Tod Johnson
Charles Moore
Joseph Daniel Coles
Tyrone Thomas
Mandala Barber
Keith Parker
Josh Haley
Heidi Arnett 1:1
Eva London
“Antwon David Murchison
Tonja Gillespie
Sharon Brower
Cecilia Dickerson 1:1
Mitch Johnson
Lindsay Watkins
Mary Kundinger
Vacant
Carolyn Wade
Holli Murphy
Sara Barton
Leah Goldsberry
* M. Stoltenberg
Robin Briggs
Russ Saladin
Kimberly McQueen
Jessica King
Robin Covington (Braillist)
Vacant (Lang. Fac.)
Kristie Medlin
Frankie Bibey
*Teresa Batalla
Sandra Owens
Mary Odom
Stephanie West
Rhonda Phipps
Christine
Clouse
Robin Kummerfeldt
Southern Pines Elem.
Teacher Assistants
Bonita Powell
Lee Foreman (Yr. Round)
Vacant
Meera Shinn
Resource
Kaitlyn Yourous
D’Etta Kyle
BED
Kelly Fagan
Cathy Jones
Vacant
* Linda Tufts
Self-Contained
Richard Dodge
Vacant
Teacher Assistants
Barbara McDonald
Latanya Brown
Speech/Lang.
Shuris Campbell
Sheila Thompson
Martha Runyon
Vacant
Southern Pines Prim.
Union Pines High
Vass-Lakeview Elem.
West End Elem.
Westmoore Elem.
West Pine Elementary
West Pine Middle
Candace Hogan
Tamatha Moore
Danielle Duncan (Fac)
Jacquelyn Jenkins
Samantha Myatt
Tara McLean
Marcia Spencer
Vaetta Cameron
* Diane Allen
Nancy Carter
Rob Hooks
Christy McKinnon
Amanda Clevenger
Amee Tiffany
Rick Peters (OCS)
Toni Douglas (OCS)
Kathi Tideman
Tracy Murphy
Chris Thomas
Anna Garner
James Sineath
Cathy Bly
Vacant 1:1
Cathy Grant (Lang. Fac.)
Vicki Comer 1:1
Stephanie West
Holly Webb
Molly McGahey
Kim Baxter
Vacant
Katie Lockamy
Donna Brown (Int)
Michelle Akin(MU)
Elaine Rogers (KG)
Karen Finder
Scott McGrath
Helen Games
Vacant
Amy Sehi
Sue Duncan
D.J. Waters
Mary Katherine Doll
Kathy Anderson
Elaine Foree
* Pam Roscoe
Stacy Federhart Hill
Angela Shue
Ellen Ashwell
Allison Hunsinger
Jessica Barkley
Suzanne Badgett
Elaina Aponte
Tina Garner
Sharon Street
Ebony Leggett
Vacant
Amanda Hill
Maria Bear
Brooke Webster
Karen Smith Meyer
Katja Hinrichsen-Smith
Paige Gambaro
Tiffany Powell
Rita Maness
Brian Carthens
Keturah Thompson 1:1
Elizabeth Kellner 1:1
Mariam Downing - Interpreter
Amanda Hill
Preschool Classes
Aberdeen Prim.
Amy Bentley Lehm
Brenda Mayo
Lynnaundria McKeithen
(Lynn)
Paulette Veloon
Carthage Elem.
Jaclyn Kennedy
Jennifer Dumas
Beverly Collins
Neil Waters
OSCO - Preschool
Ann Absher
Lisa McMillan
Robbins Elem.
Morgan Comer
LaSanya Moseley
Southern Pines Prim.
Norma Jannone
Jennifer Beadell
Trisha Keith
Jean Harrison
Tonya Patterson
Pauline Brower
Diane Atherton
Joyce Nicol
Ben Purvis
Teresa Battalla
Virginia Hammill
Keri Crowl
Donna Taylor
Anna Quick
Diane Allen
Vass-Lakeview Elem.
Michele Adams
Kathy Fowler
Whitney Marion
Lindsey Honey
Vass-Lakeview
Jane Newton
Renee Bell
Paula Nieves
Lindsey Honey
West End Elem.
Patrice Martinez
Shannon Bateman
Sonya Hand
Michelle Cunningham (Braillist)
Pam Roscoe
EDUCATION CENTER EXCEPTIONAL ED STAFF & SUPPORT SERVICES STAFF
Director
Psychologists
Becky Benton
Specialist/PS Support
Lizzie Garner
Frieda Fields Alley
Administrative Assistant
Victoria Locust
Cinda Dedmond
Renee Bustos (preschool)
COTA
Hearing Impaired
Susan Wright Itinerant Staff
OT
Dawn Perry
Carol Stewart
OT
Ray Blatz
Vacant
OT
VI Teacher
Greg Stivland
Betty Brown
OT
Christin Dieter
OT
Andrea Bayard
PT
Janice Coffey
PT
Mike Slingerland
Audiologist
Susan O’Brian (Contract)
Program
Specialist
Program
Specialist
Compliance
Transition
Coordinator
Data Liaison
Behavior
Liaison
Behavior
Support
Assistant
Behavior
Support
Assistant
Laura Dendy
Mary Beth Jackson
Kassia Stubbs
Vacant
Alvita Thomas
Drew Bond
David Johnson
MOORE COUNTY SCHOOLS
EXCEPTIONAL CHILDREN PROGRAM
EC FACILITATOR JOB DESCRIPTION
1.
The EC Facilitator is the contact person at their school for the EC Office and
disseminates information to appropriate staff at his/her school.
2.
The EC Facilitator is NOT responsible for DOING the paperwork/CECAS
entries of the EC teacher/therapist at his/her school – only to provide
technical assistance as needed. All paperwork and CECAS are the
responsibility of the Case Manager.
3.
The EC Facilitator is the INITIAL EC contact for ALL SST referrals &
transfer students at his/her school.
4.
The EC Facilitator, at the receiving school, should transfer an ACTIVE
student from another MCS into his/her school in CECAS and assign the case
manager. CW Data Sheets are still sent to EC Dept. Data Manager via email.
5.
The EC Facilitator represents the EC teachers/staff at his/her school at EC
Department meetings in order to share information and concerns with
district representatives.
Facilitators
Aberdeen Elem.
Tiffany White
Aberdeen Primary
Keri Healey
Cameron Elem.
Denise Graner
Carthage Elem.
Karyn Greco
Crain’s Creek Middle School
Angela McDougald
Elise Middle
Sherry B. Lovell
Highfalls Elem.
Pam Brady
New Century Middle
Sara Bright
North Moore High
Karen McCulloch
CLC at Pinckney
Sharon Turner
Pinecrest High
Jayne Cummings
Pinehurst Elem.
Mary Kundinger
Robbins Elem.
Robin Briggs
Sandhills Farm Life Elem.
Rhonda Phipps
Southern Pines Elem.
Meera Shinn
Southern Middle
Shelia Thompson
Southern Pines Primary
Danielle Duncan
Union Pines High
Aymee Tiffany
Vass-Lakeview Elem.
Molly McGahey
West End Elem.
D.J. Waters
Westmoore Elem.
Angela Shue
West Pine Elementary
Allison Hunsinger
West Pine Middle
Maria Bear
IMPORTANT 2014-15
E.C. DEADLINES
Please put them on your calendar now
DECEMBER 2014 HEADCOUNT DEADLINE:
ANNUAL REVIEWS & 3 YEAR REEVALUATIONS COMING DUE
ON OR BEFORE DECEMBER 3, 2014
MUST BE CLOSED/VERIFIED IN CECAS BY *NOVEMBER 20TH 2014
DO NOT SCHEDULE MEETINGS BETWEEN NOVEMBER 20TH AND DECEMBER 3RD
APRIL 2015 HEADCOUNT DEADLINE:
ALL ANNUAL REVIEWS & 3 YR REEVALUATIONS COMING DUE
ON OR BEFORE APRIL 17TH
MUST BE CLOSED/VERIFIED IN CECAS BY * MARCH 24, 2015
DO NOT SCHEDULE MEETINGS BETWEEN MARCH 24TH AND APRIL 3RD
ESY Paperwork due to Laura Dendy by Friday, March 20, 2015
ALL ANNUAL REVIEWS AND 3 YEAR REEVALUATIONS
(including year round schools)
COMING DUE ANYTIME PRIOR TO THE LAST TRADITIONAL CALENDAR DAY OF SCHOOL FOR
STUDENTS AND OCTOBER 1(FOR STUDENTS MOVING FROM ONE MOORE COUNTY SCHOOL
TO ANOTHER)
MUST BE CLOSED/VERIFIED IN CECAS BY *The Last Student Day
MAY FINANCIAL AUDIT
Occurs about middle of May each year
Random files are selected by the state- current IEP-current 3yr reevaluation and
consent to place must be in the file. Entire folder will be requested by finance
*THESE DATES ARE CRITICAL FOR COMPLIANCE MONITORING AND THERE ARE NO
EXCEPTIONS
UNLESS: APPROVED BY THE E.C. DIRECTOR PRIOR TO THE DEADLINE.
*IT IS IMPORTANT THAT NON-COMPLIANCE ISSUES BE CORRECTED PRIOR TO
HEADCOUNT SUBMISSION
AND/OR YOUR LAST WORKING DAY OF THE TRADITIONAL CALENDAR
SST Process
(back to top)
Table of Contents
Mission Statement
Student Support Team Process
Flowchart
Intervention Documentation Forms
EC Referral Process
Moore County Schools
Student Support Team (SST)
Mission Statement
The mission of the Student Support Team (SST) is to identify, support, assist and refer those students identified
as at risk in academics, behavior, health, and attendance. The team’s focus is identification, screening,
intervention, and monitoring referred students by using all available resources to promote student success.
The team members should consist of: a facilitator, a case manager, and the referring teacher(s). The parent
should also be invited to SST meetings.
Other highly recommended members may include: school administration, regular education teachers,
exceptional children teachers, school counselors, school psychologists, school social workers, school nurses,
lead teachers, school resource officers, ESL teachers, and student.
The Student Support Team Process
1) Student demonstrates one or more difficulties that impact(s) her/his education. This concern may be
identified by a parent, a teacher, or a staff member. An outside-the-school individual can also identify a
student who has some type of difficulty/disability as well.
2) Once a concern is voiced, the student is referred to the Student Support Team (SST). The individual with
the concern would typically complete the referral paperwork; however, if the individual is not on staff with
the school, the teacher or another staff member can complete the paperwork OR help the individual
complete the paperwork.
3) Once the referral is made, several things will happen. First, the SST will schedule an initial meeting to
which the parent(s) will be invited. The parent will receive a letter notifying them of the meeting and a
Parent Questionnaire for them to complete and return to school. It is not necessary that the parent(s) attend
but we encourage them to participate in the problem-solving process.
4) The school nurse will check the student’s vision and hearing as well as the student’s cumulative records to
see if there are any health concerns.
5) If speech and/or language is/are a concern, the speech pathologist will be notified.
6) If the student is an English language learner, the teacher and/or the ESL teacher will complete a brief
questionnaire.
7) At the first meeting, the SST will examine the referral concern and existing data in order to make
suggestions to the teacher about interventions to try with the student to help that her/him make academic or
behavioral/emotional gains. The teacher will begin interventions and collect data for a specific number of
weeks decided upon at the SST meeting.
8) At the second meeting, the SST will examine recently collected data and decide to:
a) continue with interventions proven successful or b) develop new interventions to be used
b) with the student for a determined number of weeks.
9) At the third meeting, the SST will examine collected data and decide to:
a) continue with interventions proven to be successful,
b) develop new interventions to be used with the student for a determined number of weeks,
or
c) refer the student to the IEP committee for consideration for Exceptional Children’s
services.
10) While this is the general process, there are not a set number of meetings nor is there a set number of weeks
of interventions are to be used nor any other time frame. Each case is different and presents unique data.
Only the SST may determine the course of the problem-solving process.
Exceptions to the above:
1) If a student already has an IEP (resource or speech) and an additional concern is identified, the person with
the concern notifies the EC teacher in charge (resource or speech).
2) The EC teacher (resource or speech) will call an IEP meeting.
3) The IEP team with address the concern(s) and determine whether or not additional testing is needed.
4) If the IEP team decides more testing is necessary to change services, the additional testing is considered a
re-evaluation.
5) If a resource student is being referred for consideration of S/L services or and SI student is being referred
for academic concerns, interventions may need to take place. If so, the classroom teacher is responsible
for the interventions and will need to collect data.
6) After interventions are done and testing is completed, the IEP team will meet to examine the new
information and to make decisions for the student.
7) The person in charge of the case is the EC teacher, whether resource or SLP.
Referrals from medical personnel, private service providers, mental health
professionals, etc.:
All referrals from individuals outside the educational system must go through the SST process or the IEP
re-evaluation process. No exceptions.
Parent requests for testing:
1) Any school staff member who receives a written request for testing from a parent or guardian should
immediately notify the EC teacher (resource) and the chair of the SST. Notification can be done in person
or by email or phone. The EC teacher will need the original written request; you may make a photocopy
for your records if you wish.
2) Write the date the written request was received by school personnel on the written request. This is
important because the “90-day timeline” begins on the date the school receives the request, not the date
written by the parent on the request.
3) The SST will meet and begin interventions for the student.
4) The IEP will meet and refer the student for testing, which will run concurrently with interventions.
5) Please note that IF interventions are successful in improving student performance, the student may not
qualify for EC services despite testing.
6) The psychologist may meet with the parent(s) requesting testing in order to discuss the SST process and
the possibility of giving the interventions a chance to work before testing takes place.
STUDENT SUPPORT TEAM PROCESS
(For NON-EC Students)
Teacher requests, completes referral for
student and returns to SST
SST Chair schedules mtg,
assigns case mgr (who completes case
mgr checklist)
Parents are invited but
not required to attend;
SST mtgs should not be
rescheduled unless it is
deemed necessary to
include parents
1st SST mtg
Collaboration with peers and parent(s)
Interventions are put in place,
including those for language concerns
For articulation,
fluency, or voice only:
SLP conducts
screening, which may
lead to IEP mtg for
evaluation IF there are
no academic concerns
2nd SST mtg
Collaboration with peers and parent(s)
Progress noted, interventions
continued, problem resolved
No progress noted, new / revised
interventions are put in place, including
those for language concerns
3rd SST mtg
Progress noted, interventions
continued, problem resolved
4th SST mtg
Collaboration with peers and parent(s)
Progress noted, interventions
continued, problem resolved
No progress noted
Team may decide to try new
interventions OR refer to IEP team
for consideration of EC services.
Collaboration with peers and parent(s)
No progress noted
Team may decide to try new
interventions OR refer to IEP team for
consideration of EC services.
If to be referred to IEP team: SST chair checks student
SST folder for all necessary paperwork and documentation,
putting forms in order and clipping as necessary, before
giving the folder to either the resource teacher or the
speech/language pathologist.
If this is a dual referral (resource and speech/lang), then
folder goes to resource teacher.
Interventions: BASIC READING SKILLS
Area of Weakness: (circle one)
Identifying letters of alphabet
Phonemic awareness (manipulating sounds, blending &
segmentation)
Alphabetic Principle (associating sounds with letters)
Phonics (sounds, sound blends, such as /ck/ and /st/)
Word decoding (decoding new words or nonsense words)
Fluency
Other: ________________________________
Baseline/Pretest: (attach a copy of dated baseline data, with work sample of similar age peer for comparison)
Brief explanation of baseline:
________________________________________________________________________________________
_______________________________________________________________________________________
Intervention #1___ #2___ #3___: (ex. Work one-on-one {OR in small group} for 20 min, 3 times / week to teach skill)
_________________________________________________________________________________________________________
________________________________________________________________________________________
Dates of intervention
Dated Work Samples*
(Attach in order)
Observations, notes, etc.
Consistent
Positive Change **
Inconsistent Positive
Change***
No Change***
Negative Change***
Post-test: (attach a copy of dated post-test after the work samples)
Brief explanation of post-test data:
________________________________________________________________________________________
________________________________________________________________________________________
* Minimum of 3 dated work samples or progress monitoring (i.e., DIBELS) completed throughout the intervention
process and prior to the post-test
** If positive change, no need to alter intervention, continue
*** If consistent positive change is not made, modify the intervention and continue for next 3 weeks
Interventions: READING COMPREHENSION
Area of Weakness: (circle one)
Main idea
Making inferences
Literal (main characters, story
Cause/effect
Sequence
Author’s purpose
Vocabulary
Other: ___________
setting, etc.)
Baseline/Pretest: (attach a copy of dated baseline data, with work sample of similar age peer for comparison)
Brief explanation of baseline:
________________________________________________________________________________________
________________________________________________________________________________________
Intervention #1___ #2___ #3___: (ex. Work in small group for 20 min, 3 times /week to teach skill)
_________________________________________________________________________________________________________
________________________________________________________________________________________
Dates of intervention
Dated Work Samples*
(Attach in order)
Observations, notes, etc.
Consistent
Positive Change **
Inconsistent Positive
Change***
No Change***
Negative Change***
Post-test: (attach a copy of dated post-test after the work samples)
Brief explanation of post-test data:
________________________________________________________________________________________
________________________________________________________________________________________
* Minimum of 3 dated work samples or progress monitoring (i.e., DIBELS) completed throughout the intervention
process and prior to the post-test
** If positive change, no need to alter intervention, continue
*** If consistent positive change is not made, modify the intervention and continue for next 3 weeks
Interventions : MATH CALCULATIONS
Area of Weakness: (circle one and add the specific level that needs to be worked on)
Counting
Identifying numbers
Use of manipulatives
Patterns
Similarities/differences
Math vocabulary (more than,
less than, altogether, etc.)
Adding on/counting up
Addition
Subtraction
Multiplication
Division
Other: _____________
Baseline/Pretest: (attach a copy of dated baseline data, with work sample of similar age peer for comparison)
Brief explanation of baseline:
________________________________________________________________________________________
________________________________________________________________________________________
Intervention #1___ #2___ #3___: (ex. Work in small group for 20 min, 3 times /week to teach skill)
_________________________________________________________________________________________________________
________________________________________________________________________________________
Dates of intervention
Dated Work Samples*
(Attach in order)
Observations, notes, etc.
Consistent
Positive Change **
Inconsistent Positive
Change***
No Change***
Negative Change***
Post-test: (attach a copy of dated post-test after the work samples)
Brief explanation of post-test data:
________________________________________________________________________________________
________________________________________________________________________________________
* Minimum of 3 dated work samples or progress monitoring (i.e., DIBELS) completed throughout the intervention
process and prior to the post-test
** If positive change, no need to alter intervention, continue
*** If consistent positive change is not made, modify the intervention and continue for next 3 weeks
Interventions: MATH REASONING
Area of Weakness: (circle one)
Problem solving: 1-step ___ 2-step ___ multi-step ___
Math vocabulary (math terms, operational terms, etc.)
Other: ____________________________________________
Baseline/Pretest: (attach a copy of dated baseline data, with work sample of similar age peer for comparison)
Brief Explanation of baseline:
________________________________________________________________________________________
________________________________________________________________________________________
Intervention #1___ #2___ #3___: (ex. Work in small group for 20 min, 3 times /week to teach skill)
_________________________________________________________________________________________________________
________________________________________________________________________________________
Dates of intervention
Dated Work Samples*
(Attach in order)
Observations, notes, etc.
Consistent
Positive Change **
Inconsistent Positive
Change***
No Change***
Negative Change***
Post-test: (attach a copy of dated post-test after the work samples)
Brief explanation of post-test:
________________________________________________________________________________________
________________________________________________________________________________________
* Minimum of 3 dated work samples or progress monitoring (i.e., DIBELS) completed throughout the intervention
process and prior to the post-test
** If positive change, no need to alter intervention, continue
*** If consistent positive change is not made, modify the intervention and continue for next 3 weeks
Interventions: WRITTEN EXPRESSION
Area of Weakness: (choose one stage of writing where breakdown begins)
Letter formation/spacing
Writing words
Writing sentence(s)
Writing paragraph(s)
Pre-writing/planning
Writing openings/endings
Conventions
Editing
Other: _________________
Baseline/Pretest: (attach a copy of dated baseline data, with work sample of similar age peer for comparison)
Brief explanation of baseline:
________________________________________________________________________________________
________________________________________________________________________________________
Intervention #1___ #2___ #3___: (ex. Work in small group for 20 min, 3 times /week to teach skill)
_________________________________________________________________________________________________________
________________________________________________________________________________________
Dates of intervention
Dated Work Samples*
(Attach in order)
Observations, notes, etc.
Consistent
Positive Change **
Inconsistent Positive
Change***
No Change***
Negative Change***
Post-test: (attach a copy of dated post-test after the work samples)
Brief explanation of post-test data:
________________________________________________________________________________________
________________________________________________________________________________________
* Minimum of 3 dated work samples or progress monitoring (i.e., DIBELS) completed throughout the intervention
process and prior to the post-test.
** If positive change, no need to alter intervention, continue intervention as delivered.
*** If consistent positive change is not made, modify the intervention and continue for next 3 weeks.
Interventions: SOCIAL / EMOTIONAL / BEHAVIORAL
Area of Weakness: (circle one and add the specific level that needs to be worked on)
Social Skills Please specify: ____________________________________________________________________
Anger Management Please specify:______________________________________________________________
Behavioral control issues Please specify:__________________________________________________________
Other Please specify:__________________________________________________________________________
Baseline/Pretest: (attach a copy of dated baseline data, with rating scale completed for the “average” same age peer
for comparison)
Brief explanation of baseline:
________________________________________________________________________________________
________________________________________________________________________________________
Intervention #1___ #2 ___ #3___: (ex. Work in small group for 20 min, 3 times /week to teach skill)
_________________________________________________________________________________________________________
________________________________________________________________________________________
Dates of intervention
Dated Work Samples*
(Attach in order)
Observations, notes, etc.
Consistent
Positive Change **
Inconsistent Positive
Change***
No Change***
Negative Change***
Post-test: (attach a copy of dated post-test after the work samples)
Brief explanation of post-test data:
________________________________________________________________________________________
________________________________________________________________________________________
* Minimum of 3 dated work samples or progress monitoring (i.e., DIBELS) completed throughout the intervention
process and prior to the post-test
** If positive change, no need to alter intervention, continue
*** If consistent positive change is not made, modify the intervention and continue for next 3 weeks
EC Referral Process
The referral process begins in multiple ways; either when a written request is received from the
parent, once the IEP team has received the written referral from the local SST recommending
possible further evaluation, an out of state or Department of Defense transfer, transitioning from
Infant Toddler Program to preschool program or a child fails a preschool screening. The first three
situation automatically trigger the 90 day time line!
Note: If a note is received by the school from the parent requesting testing please contact your
school’s psychologist immediately.
Once a referral is received from SST then the school must hold an IEP team meeting to begin the EC
referral process. At this meeting the team will be reviewing all existing data and then determining
whether or not additional data is needed.
Required Forms
Invitation to Conference
Handbook on Parent’s Rights
DEC 1
DEC 2 (if team decides to conduct evaluation)
DEC 5
Minutes
REMINDER
If a notification comes from an outside agency we have 30 days to set up a meeting with the parents
and discuss referral or not.
(back to top)
Categories of Eligibility
(back to top)
Autism
Definition
A developmental disability significantly affecting verbal and nonverbal communication and
social interaction, generally evident before age three that adversely affects a child’s
educational performance. Other characteristics often associated with autism are engagement
in repetitive activities and stereotyped movements, resistance to environmental change or
change in daily routines, and unusual responses to sensory experiences.
Autism does not apply if a child’s education performance is adversely affected primarily
because the child has an emotional disability, as described in paragraph (b)(5) of this section.
A child who manifests the characteristics of autism after age three could be identified as
having autism if the criteria in paragraph (i) of this section are satisfied.
Eligibility
Must demonstrate at least three of the four characteristics listed below:
Impairment in communication
Impairment in social interaction
Unusual response to sensory experiences
Restricted, repetitive, or stereotypic patterns of behavior, interests, and/or activities
The disability must:
Have an adverse effect on educational performance, and
Require specially designed instruction
Required Screenings and Evaluations
(A) Hearing screening;
(B) Vision screening;
(C) Observation across settings, to assess academic and functional skills;
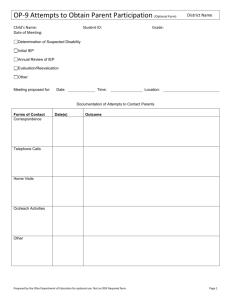
(D) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(E) Social/developmental history;
(F) Educational evaluation;
(G) Adaptive behavior evaluation;
(H) Psychological evaluation;
(I) Speech-language evaluation which includes, but is not limited to, measures of language semantics
and pragmatics;
(J) An assessment using an appropriate behavior rating tool or an alternative assessment instrument
that identifies characteristics associated with autism spectrum disorder.
Deaf-Blindness
Definition
Hearing and visual impairments that occur together, the combination of which causes such severe
communication and other developmental and educational needs that they cannot be accommodated
in special education programs solely for children with deafness or children with blindness.
Eligibility
To be determined eligible in the disability category of deaf-blindness, a child must demonstrate:
A visual impairment, in combination with a hearing impairment,
Resulting in severe communication, developmental, and educational needs, and that
Cannot be accommodated in a program for a child with solely a visual impairment or hearing
impairment.
The disability must:
Have an adverse effect on educational performance, and
Require specially designed instruction.
Required Screening and Evaluations
(A) Motor screening;
(B) Observation across settings, to assess academic and functional skills;
(C) Summary of conference(s) with parents or documentation of attempts to conference with
parents;
(D) Social/developmental history;
(E) Educational evaluation;
(F) Adaptive behavior evaluation;
(G) Psychological evaluation;
(H) Communication evaluation, including receptive, expressive, and augmentative
communication skills;
(I) Audiological evaluation, followed by an otological evaluation when appropriate;
(J) Medical evaluation, including health history, precautions, and medications; and
(K) Ophthalmological or optometric evaluation;
Deafness
Definition
Hearing impairment that is so severe that the child is impaired in processing linguistic information
through hearing, with or without amplification that adversely affects the child’s educational
performance.
Eligibility
To be determined eligible in the disability category of deafness, a child must have a deficiency in
hearing as demonstrated by the elevated threshold of auditory sensitivity to pure tones or speech.
The disability must:
Have an adverse effect on educational performance, and
Require specially designed instruction.
Required Screening and Evaluations
(A) Vision screening;
(B) Motor screening;
(C) Observation across settings, to assess academic and functional skills;
(D) Summary of conference(s) with parents or documentation of attempts to conference with
parents;
(E) Social/developmental history;
(F) Educational evaluation;
(G) Communication evaluation, including receptive, expressive, and augmentative
communication skills;
(H) Audiological evaluation, including air conduction testing, bone conduction testing, speech
receptive testing with and without amplification, and impedance testing to determine the type
and extent of hearing loss;
(I) Otological evaluation to provide diagnoses of middle and inner ear disorders.
Developmental Delay
Definition
A child aged three through seven, whose development and/or behavior is delayed or atypical, as
measured by appropriate diagnostic instruments and procedures, in one or more of the following
areas: physical development, cognitive development, communication development, social or
emotional development, or adaptive development, and who, by reason of the delay, needs special
education and related services.
Eligibility
To be determined eligible in the disability category of developmental delayed, a child must be:
Between the ages of three through seven, whose development and/or behavior is so
significantly delayed or atypical that special education and related services are required.
Delayed/Atypical Development. A child may be defined as having delayed/atypical patterns
of development in one or more of the following five areas: physical development, cognitive
development, communication development, social/emotional development or adaptive
development.
The criteria for determining delayed development for ages three through seven are:
o A 30 percent delay using assessment procedures that yield scores in months, or test
performance of 2 standard deviations below the mean on standardized tests in one
area of development; or
o A 25 percent delay using assessment procedures that yield scores in months or test
performance of 1.5 standard deviations below the mean on standardized tests in two
areas of development.
Identification of these children will be based on informed educational/clinical opinion and
appropriate assessment measures.
Delayed/Atypical Behavior: A child with delayed or atypical behavior is characterized by behaviors
that are so significantly inadequate or inappropriate that they interfere with the child’s ability to
learn and/or cope with normal environmental or situational demands. There must be evidence that
the patterns of behavior occur in more than one setting over an extended period of time.
The criteria for determining delayed/atypical behavior for ages three through five must be
documented in one or more of the following areas:
Delayed or abnormalities in achieving milestones and/or difficulties with issues, such as:
o Attachment and/or interaction with other adults, peers, materials, and objects;
o Ability to communicate emotional needs;
o Ability to tolerate frustration and control behavior, or
o Ability to inhibit aggression.
Fearfulness, withdrawal, or other distress that does not respond to comforting or
interventions;
Indiscriminate sociability, for example, excessive familiarity with relative strangers; or
Self-injurious or other aggressive behavior.
The criteria for determining delayed patterns of behavior and adaptive skills for ages six through
seven must be exhibited in two or more of the following ways:
The inability to interact appropriately with adults and peers;
The inability to cope with normal environmental or situational demands;
The use of aggression or self-injurious behavior, or
The inability to make educational progress due to social/emotional deficits.
Identification of these children will be based on informed educational/
clinical opinion and appropriate assessment measures.
Required Screening and Evaluations
(A) Hearing screening;
(B) Vision screening;
(C) Motor screening;
(D) Health screening;
(E) Speech-language screening;
(F) Observation across settings, to assess academic and functional skills;
(G) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(H) Social/developmental history;
(I) Educational evaluation;
(J) Adaptive behavior evaluation; and
(K) Psychological evaluation, including cognitive and social-emotional measures;
Emotional Disability
Definition
Means a condition exhibiting one or more of the following characteristics over a long period of time
and to a marked degree that adversely affects a child's educational performance:
An inability to make educational progress that cannot be explained by intellectual, sensory,
or health factors.
An inability to build or maintain satisfactory interpersonal relationships with peers and
teachers.
Inappropriate types of behavior or feelings under normal circumstances.
A general pervasive mood of unhappiness or depression.
A tendency to develop physical symptoms or fears associated with personal or school
problems.
Serious emotional disability includes schizophrenia. The term does not apply to children who are
socially maladjusted, unless it is determined that they have an emotional disturbance.
Eligibility
To be determined eligible in the disability category of serious emotional disability:
One of the following characteristics must be exhibited:
An inability to make educational progress that cannot be explained by intellectual, sensory,
or health factors;
An inability to build or maintain satisfactory interpersonal relationships with peers and
teachers;
Inappropriate types of behavior or feelings under normal circumstances;
A general pervasive mood of unhappiness or depression; or
A tendency to develop physical symptoms or fears associated with personal or school
problems.
Additionally, the condition must be exhibited:
Over a long period of time; and
To a marked degree.
The disability must:
Have an adverse effect on educational performance, and
Require specially designed instruction.
Required Screening and Evaluations
(A) Hearing screening;
(B) Vision screening;
(C) Two scientific research-based interventions to address behavioral/emotional
skill deficiency and documentation of the results of the interventions, including
progress monitoring documentation;
(D) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(E) Communication evaluation;
(F) Review of existing data;
(G) Social/developmental history;
(H) Observation across settings, to assess academic, functional, and behavioral
skills;
(I) Educational evaluation;
(J) Psychological evaluation, to include an intellectual evaluation;
(K) Behavioral/emotional evaluation which may include a behavior/emotional skill rating
Hearing Impairment
Definition
An impairment in hearing, whether permanent or fluctuating, that adversely affects a child’s
educational performance but that is not included under the definition of deafness in this section.
Eligibility
To be determined eligible in the disability category of hearing impairment, a child must have a
documented hearing loss of a type and extent to:
Have an adverse effect on educational performance, and
Require specially designed instruction.
Required Screening and Evaluations
(A) Vision screening;
(B) Usher Syndrome screening;
(C) Social/developmental history;
(D) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(E) Observation across settings, to assess academic and functional skills;
(F) Educational evaluation;
(G) Communication evaluation, including receptive, expressive, and augmentative
communication skills;
(H) Otological evaluation for diagnoses of middle or inner ear disorders; and
(I) Audiological evaluation to include air conduction testing, speech reception
testing with and without amplification, and impedance testing to determine the
type of any hearing loss that may be present.
Intellectual Disability
Definition
Significantly subaverage general intellectual functioning that adversely affects a child’s educational
performance existing concurrently with deficits in adaptive behavior and manifested during the
developmental period.
Eligibility
To be determined eligible in the disability category of intellectual disability, a child must
demonstrate both:
Intellectual functioning well below the mean on an individually administered standardized
intelligence test, and the standard error of measurement of that test shall be taken into
account in the interpretation of the results. Measures below the mean are as follows:
o Mild: Two standard deviations below the mean plus or minus one standard error of
measure;
o Moderate: Three standard deviations below the mean plus or minus one standard error
of measure;
o Severe: Four or more standard deviations below the mean plus or minus one standard
error of measure.
Adaptive behavior deficits at or below:
o Two standard deviations below the mean in one domain, or
o One and one-half standard deviations below the mean in two or more domains.
The disability must:
Have an adverse effect on educational performance, and
Require specially designed instruction.
Required Screening and Evaluations
(A) Hearing screening;
(B) Vision screening;
(C) Health screening;
(D) Motor screening;
(E) Speech/language screening;
(F) When there is no prior diagnosis of intellectual disability, two research-based
interventions to address academic and/or functional skill deficiencies and
documentation of the results of the interventions, including progress
monitoring documentation;
(G) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(H) Review of existing data;
(I) Social/developmental history;
(J) Observation across settings, to assess academic, functional, and behavioral
skills;
(K) Educational evaluation;
(L) Adaptive behavior evaluation; and
(M) Psychological evaluation, to include an intellectual evaluation.
Multiple Disabilities
Definition
Two or more disabilities occurring together (such as intellectual disability-blindness, intellectual
disability-orthopedic impairment, etc.), the combination of which causes such severe educational
needs that they cannot be accommodated in special education programs solely for one of the
impairments. Multiple disabilities does not include deaf-blindness.
Eligibility
To be determined eligible in the disability category of multiple disabilities, a child must
demonstrate:
Two or more disabilities occurring together,
The combination of which is so severe, complex, and interwoven that identification in a
single category of disability cannot be determined.
The disability must:
Have an adverse effect on educational performance, and
Require specially designed instruction
Required Screening and Evaluations
(A) Hearing screening;
(B) Vision screening;
(C) Social/developmental history;
(D) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(E) Observation across settings, to assess academic and functional skills;
(F) Educational evaluation;
(G) Adaptive behavior evaluation;
(H) Psychological evaluation;
(I) Speech/language evaluation;
(J) Medical evaluation; and
(K) Motor evaluation.
Orthopedic Impairment
Definition
A severe physical impairment that adversely affects a child's educational performance. The term
includes impairments caused by a congenital anomaly, impairments caused by disease (e.g.,
poliomyelitis, bone tuberculosis, etc.), and impairments from other causes (e.g., cerebral palsy,
amputations, and fractures or burns that cause contractures, etc.).
Eligibility
To be determined eligible in the disability category of orthopedic impairment, a child must
demonstrate:
A severe physical impairment;
Caused by congenital abnormalities, disease, or other causes.
The disability must:
Have an adverse effect on educational performance, and
Require specially designed instruction.
Required Screening and Evaluations
(A) Hearing screening;
(B) Vision screening;
(C) Social/developmental history;
(D) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(E) Observation across settings, to assess academic and functional skills;
(F) Educational evaluation;
(G) Medical evaluation;
(H) Motor evaluation.
Other Health Impairment
Definition
Having limited strength, vitality or alertness, including a heightened alertness to environmental
stimuli, that results in limited alertness with respect to the educational environment, that:
Is due to chronic or acute health problems such as asthma, attention deficit disorder or
attention deficit hyperactivity disorder, diabetes, epilepsy, a heart condition, hemophilia, lead
poisoning, leukemia, nephritis, rheumatic fever, sickle cell anemia, and Tourette’s Syndrome,
etc.
Adversely affects a child's educational performance.
Eligibility
To be determined eligible in the disability category of other health impairment, a child must have a
chronic or acute health problem resulting in one or more of the following:
Limited strength;
Limited vitality;
Limited alertness, including heightened alertness to environmental stimuli that results in
limited alertness with respect to the educational environment.
The disability must:
Have an adverse effect on educational performance, and
Require specially designed instruction.
Required Screening and Evaluations
(A) Hearing screening;
(B) Vision screening;
(C) Two research-based interventions to address academic and/or behavioral skill
deficiencies and documentation of the results of the interventions, including
progress monitoring documentation;
(D) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(E) Observation across settings, to assess academic and functional skills;
(F) Social/developmental history;
(G) Educational evaluation; and
(H) Medical evaluation.
Specific Learning Disability
Definition
General: Means a disorder in one or more of the basic psychological processes involved in
understanding or in using language, spoken or written, that may manifest itself in the impaired
ability to listen, think, speak, read, write, spell, or to do mathematical calculations, including
conditions such as perceptual disabilities, brain injury, minimal brain dysfunction, dyslexia, and
developmental aphasia.
Disorders not included: Specific learning disability does not include learning problems that are
primarily the result of visual, hearing, or motor disabilities, of mental retardation, of serious
emotional disturbance, or of environmental, cultural, or economic disadvantage.
Eligibility
To be determined eligible in the disability category of specific learning disability using the
discrepancy option, a child must:
Demonstrate inadequate achievement for their age or to meet State approved grade-level
standards in one or more of the following areas:
o Oral expression;
o Listening comprehension;
o Written expression;
o Basic reading skills;
o Reading fluency skills;
o Reading comprehension;
o Mathematics calculation; and
o Mathematical problem solving.
Demonstrate a discrepancy between achievement (as measured by the educational
evaluation) and measured ability (as measured by the intellectual evaluation) of at least 15
points. Subscale, subtest, factor or other scores used to estimate intellectual functioning may
not be used to determine a discrepancy;
Exhibit characteristics consistent with the definition of specific learning disabilities.
The disability must:
Not be the primary result of:
o Sensory deficits;
o Motor deficits;
o Intellectual disability;
o Serious emotional disability;
o Environmental influences;
o Cultural linguistic influences,
o Economic influences;
o Lack of instruction in reading or math; and/or
o Limited English proficiency.
Have an adverse effect on educational performance, and
Require specially designed instruction.
Required Screening and Evaluations
(A) Hearing screening;
(B) Vision screening (far and near acuity);
(C) Speech/language screening;
(D)Two research-based interventions to address academic skill deficiencies
and documentation of the results of the interventions, including progress
monitoring documentation;
(E) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(F) Review of existing data;
(G) Social/developmental history;
(H) Observation across settings, to assess academic, and functional skills;
(I) Educational evaluation; and
(J) Psychological evaluation, to include an intellectual evaluation.
Eligibility through Alternative to discrepancy
If the IEP team determines that the assessment measures obtained did not accurately reflect the
discrepancy between achievement and ability, the team may consider documentation of an
alternative to the discrepancy. The IEP team must:
determine that the assessment measures did not accurately reflect the discrepancy between
achievement and ability;
state in writing the assessment procedures used, the assessment results, the criteria applied to
judge the importance of any difference between expected and current achievement; and
determine whether a substantial discrepancy in the student’s performance is present.
The use of a process based on a child’s response to scientific research-based intervention. LEAs can
utilize a process that determines a student’s response to scientific research-based intervention as part
of a comprehensive evaluation to determine eligibility in the disability category of Specific Learning
Disability. A problem-solving process must be utilized to make educational decisions about a child’s
responsiveness. The following must occur during the problem-solving process:
Tier I –
Hearing screening;
Vision screening (far and near acuity);
Implementation of a scientific research-based intervention;
Progress monitoring data;
Documented parent and teacher assessment of the effectiveness of the intervention;
Summary of conference(s) with parents or documentation of attempts to conference with
parents; and
Review of existing data.
Tier II –
Analysis of Tier I scientific research-based intervention;
Documented modifications/discontinuation of the intervention or implementation of a new
scientific research-based intervention;
Progress monitoring data;
Documented parent and teacher assessment of the effectiveness of the intervention; and
Summary of conference(s) with parents and other school staff.
Tier III –
Analysis of Tier II scientific research-based intervention;
Documented modifications/discontinuation of the intervention or implementation of a new
scientific research-based intervention;
Progress monitoring data;
Documented parent, staff, and problem-solving team assessment of the effectiveness of the
intervention;
Summary of conference(s) with parents, school staff, and the problem solving team;
Speech language screening;
Social/developmental history; and
Observation by an independent observer for the purpose of intervention and to inform
instruction.
Tier IV –
Analysis of Tier III scientific research-based intervention;
Documented modifications/discontinuation of the intervention or implementation of a new
scientific research-based intervention;
Summary of conference(s) with parents, school staff, and the problem solving team; and
Option 1: Modify Level III intervention (frequency, intensity, duration, or content) and
implement the modifications; or
Option 2: Complete referral for special education. If Option 2 is chosen, receipt of the
completed referral for special education by school personnel begins the 90 day timeline,
defined in NC 1503-2.2(c)(1), and requires that informed parent consent for evaluation be
obtained.
To be determined eligible for services in the disability category of specific learning disabilities using
a process based on a child’s response to scientific research-based interventions, the following criteria
must be met:
The child demonstrates achievement that is not adequate for the child’s age or the attainment
of State-approved grade-level standards, when provided with learning experiences and
instruction appropriate for the child’s age or State-approved grade-level standards, including
at least two scientific, research-based interventions in one or more of the following areas:
o Listening comprehension;
o Oral expression;
o Written expression;
o Basic reading;
o Reading fluency;
o Reading comprehension;
o Mathematics calculation;
o Mathematics reasoning; or
o The child exhibits a pattern of strengths and weaknesses in performance,
achievement, or both, relative to age, State-approved grade-level standards, or
intellectual development, that is determined by the group to be relevant to the
identification of a specific learning disability, using appropriate assessments.
The child does not make sufficient progress to meet age or State approved grade-level
standards in one or more of the areas identified in paragraph (a) of this section; or the IEP
team determines the child needs an intervention, in order to make sufficient progress, that
requires resources beyond what can be reasonably provided in general education
The child exhibits characteristics of specific learning disabilities consistent with the
definition.
The disability must:
Not be the primary result of:
o Sensory deficits;
o Motor deficits;
o Intellectual disability;
o Serious emotional disability;
o Environmental, cultural/linguistic influences;
o Limited English proficiency;
o Economic influences;
o Lack of instruction in reading or math.
o Have an adverse effect on educational performance, and
Require specially designed instruction.
Speech or Language Impairment
Definition
A communication disorder, such as an impairment in fluency, articulation, language, or
voice/resonance, that adversely affects a child's educational performance.
Language may include function of language (pragmatic), the content of language (semantic),
and the form of language (phonologic, morphologic, and syntactic systems).
A speech or language impairment may result in a primary disability or it may be secondary to
other disabilities.
Eligibility
To be determined eligible for services in the disability category of speech or language impairment, a
child must meet the criteria listed in one or more of the following areas:
Articulation. It is required that a child’s speech have:
o Two or more phonemic errors not expected at the child’s age or developmental level
observed during direct testing and/or in conversational speech, and/or
o Two or more phonological processes not expected at the child’s age or development
level observed during direct testing and/or in conversational speech.
Fluency. It is required that a child demonstrate non-fluent speech behavior characterized by
repetitions/prolongations/blocks on a regular basis.
Language. It is required that two diagnostic measures occur, one assessing comprehension
and one assessing production of language. It is required that:
o Standard scores on the particular standard evaluation instrument suggest a language
disorder; and/or
o Non-standardized/informal assessment indicates that the child has difficulty
understanding and/or expressing ideas and/or concepts.
Voice. It is required that a child must demonstrate consistent deviations in vocal production
that are inappropriate for chronological/mental age, gender, and ability.
The disability must:
Have an adverse effect on educational performance, and
Require specially designed instruction.
Required Screening and Evaluations
(A) Hearing screening;
(B) Articulation screening;
(C) Fluency screening;
(D) Language screening;
(E) Voice/resonance screening;
(F) Social/developmental history;
(G) Observation across settings, to assess academic, functional, and behavior skills;
(H) Summary of conference(s) with parents or documentation of attempts to
conference with parents; and
(I) Educational evaluation.
Additionally, one of the following evaluations shall be completed. The required
evaluation(s) shall be determined based on screening results and shall be individualized
to address the specific area(s) of concern as listed:
(A) Articulation evaluation
(B) Fluency evaluation
(C) Language evaluation including form, content and function
(D) Voice/resonance evaluation
Traumatic Brain Injury
Definition
An acquired injury to the brain caused by an external physical force, resulting in total or partial
functional disability or psychosocial impairment, or both, that adversely affects a child's educational
performance. Traumatic brain injury applies to open or closed head injuries resulting in impairments
in one or more areas, such as cognition; language; memory; attention; reasoning; abstract thinking;
judgment; problem-solving; sensory, perceptual, and motor abilities; psychosocial behavior; physical
functions; information processing; and speech. Traumatic brain injury does not apply to brain
injuries that are congenital or degenerative, or to brain injuries induced by birth trauma.
Eligibility
To be determined eligible in the disability category of traumatic brain injury, a written verification
by a licensed physician or a licensed psychologist, appropriately practicing in the specialty of
neuropsychology, that the child has sustained an injury from which brain injury can be inferred must
be obtained. No time limits exist for written verification.
Psychological evaluation for traumatic brain injury must be conducted by school
psychologists licensed by the State Department of Public Instruction, or by psychologists
who are appropriately practicing in the specialty of neuropsychology and are licensed by the
North Carolina State Board of Examiners of Practicing Psychologists. All psychological
evaluations for Traumatic Brain Injury must be current within one year. All school
psychologists providing assessment of children with Traumatic Brain Injury must meet the
guidelines of the Exceptional Children Division for training in the assessment of Traumatic
Brain Injury and be listed on the Exceptional Children Division's registry of approved
providers (hereafter referred to as the registry.)
The disability must:
o Have an adverse effect on educational performance, and
o Require specially designed instruction.
Required Screening and Evaluations
(A) Hearing screening;
(B) Vision screening;
(C) Speech/language screening;
(D) Two scientific research-based interventions to address academic and/or
behavioral skill deficiencies and documentation of the results of the
interventions, including progress monitoring documentation.
* Note: Screenings (A) through (D) may be waived for students who have been medically diagnosed
with traumatic brain injury and who have received medical and/or rehabilitative services in a
medical or rehabilitation program or setting within the previous twelve months.
(E) Review of medical history and records;
(F) Review of educational history and records;
(G) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(H) Social/developmental history;
(I) Observation across settings to assess academic and functional skills;
(J) Educational evaluation;
(K) Psychological evaluation for traumatic brain injury; and
(L) Motor evaluation.
Visual Impairment including Blindness
Definition
An impairment in vision that, even with correction, adversely affects a child's educational
performance. The term includes both partial sight and blindness. A visual impairment is the result of
a diagnosed ocular or cortical pathology.
Eligibility
To be determined eligible in the disability category of visual impairment, including blindness, a
child must have:
A visual acuity between 20/70 and 20/200 in the better eye after correction to be considered
visually impaired.
A visual acuity of 20/200 or less in the better eye after correction or a peripheral field so
contracted that the widest diameter subtends an arc no greater than 20 degrees to be
considered legally blind.
The disability must:
Have an adverse effect on educational performance; and
Require specially designed instruction.
Required Screening and Evaluations
(A) Hearing screening;
(B) Summary of conference(s) with parents or documentation of attempts to
conference with parents;
(C) Social/developmental history;
(D) Educational evaluation;
(E) Ophthalmological or optometric evaluation;
(F) For preschool children:
Observation across settings to include:
1. Observation of physical, behavioral and environmental
characteristics;
2. Shutting or covering one eye, tilting head or thrusting head forward,
squinting eyelids together;
3. Difficulty with work requiring vision;
4. Avoidance of near work task or irritation when required to do near
work;
5. Inability to see distant objects;
6. Difficulty with navigation; and
7. Eye appearance (e.g., crossed eyes, nystagmus).
(G) For school age children:
a. Observation across settings to assess academic, and functional skills;
b. Functional vision assessment; and
c. Braille skills inventory and/or media assessment.
Forms Information
and Directions
(back to top)
Table of Contents
Parent Invitation to Conference
Student Invitation to Conference (18 or older)
Student Invitation to Conference (14 to 17)
Referral DEC 1
Preschool Referral DEC 1
Consent for Evaluation DEC 2
Summary of Evaluation/Eligibility Worksheets
(AU, DB, Deafness, HI, DD, SED, ID, MU, OI, OHI, SLD, SI, TBI, VI)
Eligibility Determination DEC 3
IEP DEC 4
Secondary Transition DEC 4a
Additional Transition Meeting Information for Moore County Schools
Related Services Support Description DEC 4b
Prior Written Notice DEC 5
IEP Committee Minutes – DEC 5
IEP Committee Minutes (when not using a DEC 5)
Prior Written Notice – Disciplinary Change in Placement DEC 5a
Change in Placement Worksheet
Manifestation Determination Form
Consent for Services DEC 6
Reevaluation DEC 7
Moore County Reevaluation Forms
Communication Plan Worksheet for Deaf and Hard of Hearing (Worksheet 1)
ESY Worksheet (Worksheet 2)
Services Plan for Parentally Placed Private Schools (Worksheet 3 - speech only)
Manifestation Determination Form
Monthly Review of Home/Hospital Placement due to Discipline
Maintenance and Access of Records (DEC 9)
Parent Contact Log (DEC 10)
Release to Share Information
Evaluation Matrix
Request for Screening (DEC 21)
Document Receipt Form
Folder Order Forms
IEP Progress Reports
Graduation/Exit Documentation
Review of Accommodations Used During Testing
Parent Invitation to Conference Directions
As team members, IDEA requires parents of students with disabilities to be invited to the IEP team
meeting.
When parents share custody of a student, and educational rights of the parents are not in question,
the LEA must issue an invitation to participate in the meeting to both parents. Participation in
meetings may be through alternative means.
By checking the purpose of this meeting the parent is informed of the items that may be discussed at
the IEP meeting. If a parent is not in attendance, the IEP team may not discuss items not checked on
the original invitation.
IDEA requires the listing of participants’ positions, not individual names.
IDEA requires that parents receive adequate notice to participate in the meeting. Reasonable notice
is defined as 7-10 days. Adequate notice should be provided to all participants, including related
service providers.
While it is not documented on the form, LEAs are responsible for ensuring that parents receive a
copy of the Handbook on Parent’s Rights at least one time each school year.
If the LEA has documented notice that the parent(s) will attend the meeting and the parent cancels
on the day of the meeting, or does not attend, the LEA may conduct the meeting as scheduled.
If the LEA has documentation that the parent(s) indicate they will be in attendance, a second notice
is not required.
Invitation/Prior Notice
INVITATION TO CONFERENCE
Date:
Dear
/
/
:
Re:
For a student to receive the education needed, it is important for the school and the parents to work together. We are requesting that you
attend a conference to discuss
’s special needs. You may also bring another individual(s) whom you believe has knowledge or special
expertise regarding your child. Although it is not required for you to notify the school of additional participants, it is helpful in making
appropriate arrangements. If your child is transitioning from the Part C-Infant Toddler Program, you may request we invite one or more of
the Part C-Infant Toddler representatives.
The purpose of this meeting is to: (Check all that may apply)
Discuss special education referral for initial evaluation or reevaluation determination.
Discuss evaluation results to determine if your child is or continues to be eligible for special education and related services.
Discuss and/or develop, review, and/or revise your child’s IEP.
Discuss and/or review, and/or revise your child’s educational placement.
Other:
Transition Planning:
For a child who is or will be 14 years of age or older during the duration of this IEP:
Your child is being invited to attend this meeting as required by state and federal statute.
The following required members of the IEP team are expected to attend the meeting: (Attach Request to Excuse if all are not checked.)
LEA Representative
Special Education Provider of the Student
General Education Teacher of the Student
Individual who can Interpret Evaluation Results
Other participants expected to attend the meeting:
The following agency representative(s) invited to attend the meeting are:
(Parental permission to invite agency representative(s) must be in the Exceptional Children confidential record.)
The meeting is scheduled for (date)
/
/
, at (time)
, (place)
.
If this time is inconvenient, I will be happy to reschedule the meeting at a mutually agreeable time. Please call (phone)
or
email
. If you are unable to attend or would prefer to participate by telephone, a conference call can be arranged. At this meeting, you
are entitled to all the due process parental rights described in the Handbook on Parents’ Rights.
Sincerely,
Name
Title
School
Parent/Guardian Response to Invitation:
Please respond to this notice by checking the appropriate option below and return one copy of this form prior to the meeting.
I will attend the meeting as scheduled.
I will participate in this IEP team meeting by phone or other means. I can be reached at the following phone number on the date/time
mentioned above: (
)
.
I cannot attend or participate in the meeting at this time. Please contact me to arrange a mutually agreed upon time.
Phone (
)
.
Parent/Guardian Signature:
2nd Notice: / /
, Type of Notice:
Date:
Student Invitation to Conference Directions (age 18 and older)
Individuals responsible for issuing the invitation to the student need to ensure the student understands, to the
best of his/her ability, what the form means.
Parents of students age 18 or older are required to be notified of the IEP meeting.
Participation in the meetings may be through alternative means.
Please include the full name of the student on the form.
IDEA requires the listing of participants’ positions, not individual names.
IDEA requires that the student receive adequate notice to participate in the meeting. Reasonable notice is
defined at 7-10 days.
Adequate notice should be provided
While it is not documented on the form, LEAs are responsible for ensuring that the student age 18 or older,
receives a copy of the Handbook on Parent’s Rights at least one time each school year.
If the LEA has documented notice that the student age 18 or older will attend the meeting and the student
cancels on the day of the meeting, or does not attend, the LEA may conduct the meeting as scheduled.
If the LEA has documentation that the student age 18 or older indicates he/she will be in attendance, a second
notice is not required.
Invitation-Student Age 18 & Older/Prior Notice
INVITATION TO CONFERENCE FOR STUDENTS AT AGE 18 OR OLDER
Date:
Dear
/
/
:
For you to receive the education you need and to plan for your post-secondary goals, it is important that you and the school work
together. We are requesting that you attend a conference to discuss your special needs. You may also bring another person(s) who has
knowledge or special expertise about you. Although it is not required for you to notify the school of additional participants, it is
helpful in making appropriate arrangements. Your parents will be notified of the meeting.
The purpose of this meeting is to: (Check all that apply)
Discuss special education referral for initial evaluation or reevaluation determination.
Discuss evaluation results to determine if you are or continue to be eligible for special education and related services.
Discuss and/or develop, review, and/or revise your IEP and/or educational placement .
Other:
The following required members of the IEP team are expected to attend the meeting: (Attach Request to Excuse if all are not checked.)
LEA Representative
Special Education Provider of the Student
General Education Teacher of the Student
Individual who can Interpret Evaluation Results
Other participants expected to attend the meeting:
The following agency representative(s) invited to attend the meeting are:
(Student permission to invite agency representative(s) must be in the Exceptional Children confidential record.)
The meeting is scheduled for (date)
/
/
, at (time)
, (place)
.
If this time is inconvenient, I will be happy to reschedule the meeting at a mutually agreeable time. Please call (phone)
or
email
. If you are unable to attend or would prefer to participate by telephone, a conference call can be arranged. At this meeting, you are
entitled to all the due process parental rights described in the Handbook on Parents’ Rights.
Sincerely,
Name
Title
School
Student Response to Invitation:
Please respond to this notice by checking the appropriate option below and return one copy of this form prior to the meeting.
I will attend the meeting as scheduled.
I will participate in this IEP team meeting by phone or other means. I can be reached at the following phone number on the
date/time mentioned above: ( )
.
I cannot attend the meeting at this time. Please contact me to arrange another time. Phone ( )
.
Student Signature: ______________________________________________________________
2nd Notice:
/
/
, Type of Notice:
Date: ______ / ______ / ______
Student Invitation to Conference (age 14 to 17) Directions
Individuals responsible for issuing the invitation to the student need to ensure the student understands, to the
best of his/her ability, what the form means.
Alternative means to allow for participation may be provided.
Please include the full name of the student on the form.
IDEA requires the listing of participants’ positions, not individual names.
Student Invitation-Prior to Age 18/Prior Notice
STUDENT INVITATION TO CONFERENCE
(REQUIRED FOR STUDENTS AGES 14 through 17)
Date:
Dear
/
/
:
You are invited to come to a meeting to develop, review and, as appropriate, revise your Individualized
Education Program (IEP). This meeting is about planning your future. You are the key person in this
planning, so it is very important that you attend. We will discuss transition services at this meeting. The IEP
will be written to help you reach your personal goals for what you want to do after you finish high school.
At this meeting you will have a chance to:
Share your preferences, needs, and interests;
Discuss where you would like to work, live, and/or continue your education.
Then, together all members of your IEP team may:
Discuss your strengths and areas for growth;
Develop a plan for the coming year;
Outline members’ roles and responsibilities to help you prepare for adult life; and
Discuss transfer of parental rights (inform student one (1) year prior to the 18th birthday).
The meeting is scheduled for (date)
/
/
, at (time)
, (place)
.
Your parent(s) have been invited to this meeting. If you have any questions about this letter or the meeting,
please see me.
The following members of your IEP team are expected to attend the meeting:
LEA Representative
Special Ed. Teacher of the Student
General Ed. Teacher of the Student
Individual who can Interpret
Evaluation Results
Please sign this form and return it to me before the meeting.
Sincerely,
Special Education Provider
Student Signature: ___________________________________________ Date: ______/______/______
I will attend the meeting.
I will not attend the meeting.
Referral (DEC 1 pg. 1) Directions
This form documents initial referral for the determination of special education evaluation. The initial referral
must be completed either when a written request is received from the parent, once the IEP team has received the
written referral from the local SST recommending possible further evaluation, an out of state or Department of
Defense transfer, transitioning from Infant Toddler Program to preschool program or a child fails a preschool
screening.
Out of state transfers require a review of existing data to determine what, if any additional information is
needed to determine eligibility in North Carolina. If any additional data is needed based on the review, it is
considered an initial evaluation for purposes of determining eligibility and placement.
Until the above stated process is complete, the LEA must provide comparable services in accordance with
IDEA. The LEA has a responsibility to expedite this process for out of state transfer students.
In responding to items A-E, review formal and informal assessment results, to include parental input, as part of
your review of existing data.
Section is I used to reflect what information is currently known about the student.
Referral/Prior Notice DEC 1 (1 of 4)
SPECIAL EDUCATION REFERRAL
Student:
DOB:
NC Wise #
/
/
Grade:
School:
Gender:
Ethnicity:
Parent/Guardian:
Address:
Telephone:
(Home)
(Work)
(Cell)
Email:
Student’s Teacher(s):
Is this student transferring from another state with a current IEP?
Vision Screening Date:
Hearing Screening Date:
/
/
/
Pass
/
Pass
Fail
yes
no
Far
R 20/
L 20/
Near
R 20/
L 20/
Fail
dB (Intensity Level)
Hz (Frequencies)
Comment:
I. DISCUSSION OF STUDENT’S STRENGTHS (Must address all areas.)
A. Describe student’s academic and functional skill strengths (reading, math, written language, daily living activities).
B. Describe student’s behavioral/social skill strengths.
C. Describe student’s study/work skill strengths.
D. Describe student’s communication skill strengths.
E. Describe student’s motor skill strengths (gross/fine motor).
Referral (DEC 1 pg. 2) Directions
Section II is used to reflect what information is currently known about this student.
School Age Referral/Prior Notice DEC 1 (2 of 4)
Student:
Grade:
School:
II. REASON(S) FOR REFERRAL/AREAS OF CONCERN
Language Arts
Phonemic Awareness
Word Identification
Alphabetic Knowledge
Reading Comprehension
Reading Fluency
Written Expression
Writing Mechanics
Writing Conventions
Vocabulary (Reading/Oral)
Other
Mathematics
Basic Math Facts
Computation
Problem-Solving
Word Problems
Geometry
Measurement
Probability/Data
Analysis
Math Reasoning
Other
Behavior/Social
Noncompliance
Motivation
Lack of Motivation
Self-concept/Esteem
Peer or Adult Relationships
Withdrawn/Moody
Overactive
Verbally Aggressive
Physically Aggressive
Fearful/Anxious
Ritualistic Behaviors
Self-destructive
Overly Sensitive/Cries Easily
Poor Social Boundaries
Other
Health/Medical
Visual Acuity
Hearing
Seizures
Overweight/Underweight
Tired/Listless
Frequently Gets Hurt
Diagnosed Medical Condition
Communication
Expressive Language
Receptive Language
Non-verbal
Articulation
Voice Problems
Fluency
Vocabulary
Other
Motor
Daily Living Skills
Toileting
Dressing Self
Feeding Self
Drinking From Cup
Communicating Basic
Wants/Needs
Safety (to self or others)
Understanding/Responding
to Social Cues
Gullible/Naïve
Understanding /Responding
to Environmental Cues
Other
Other Concerns:
Medication
Physical Complaints
Diagnosed Mental Health Condition
Copying
Handwriting
Walking/Running
Throwing/Catching
Fine Motor Coordination
Gross Motor Coordination
Moving from sitting to standing
Moving from standing to sitting
Transitioning from class to class
Frequent falls
Concerns with child safety
Commode transfer
Overall coordination
Other
Other
Study/Work Skills
Disorganized
Making Transitions
Avoids Difficult Tasks
Following Directions
Completing Tasks
Does not work independently
Remaining in seat
Attention Span/Concentration
Excessive Daydreaming
Turning in Assignments
Difficulty with Memory
Other
Person(s) Making Referral:
Referral (DEC 1 pg. 3) Directions
Date school received written referral starts the 90-day timeline.
Section III, part A must include specific results gathered through progress monitoring.
In part F of Section III LEAs are instructed not to restate A-E, but to provide a synthesis of the information
gathered through the review of existing information.
Referral/Prior Notice DEC 1 (3 of 4)
Student:
Grade:
Date School Received Written Referral:
/
School:
/
III. REVIEW OF EXISTING DATA BY IEP TEAM MEMBERS (Must address all areas A-F.)
A. Describe the instructional practices/interventions implemented to address area(s) of noted concern and state the
outcomes.
B. Describe evaluation and/or information provided by the parent.
C. Describe results of local and state assessment data.
D. Describe observations by teachers, related service providers, administrators.
E. Describe information, if any, reviewed from other sources.
F.
Summarize what was learned about the student from the review of existing data listed in A – E.
Referral (DEC 1 pg, 4) Directions
In Section VI the IEP team must check one.
IEP teams are obligated to conduct assessments to address all areas of need regardless of the suspected
disability. (This would be based off of what is checked on page two of the DEC 1.)
Note:
If a child has been referred for multiple concerns, it is possible that the IEP team may complete more
than one DEC 3 Summary of Evaluation/Eligibility Worksheet. In doing so, if the child would qualify for more
than one area (ex: SED and SLD) the team must determine which is the primary disability. This is noted on the
DEC 3 Eligibility Determination Form. When completing the DEC 4 you would also note both eligibilities on
page 1.
Referral/Prior Notice DEC 1 (4 of 4)
Student:
Grade:
School:
IV. IEP TEAM DETERMINATION
No evaluation will be conducted based on the review of existing information. The special education process ceases.
Explain decision not to evaluate:
Team completes Prior Written Notice & provides copy to parent along with the Handbook on Parents’ Rights.
Determine eligibility based solely on existing evaluation data made available to the IEP Team through the referral
process. No additional data are being requested. (For preschool students consider current IFSP.) List the source(s) of
existing evaluation data:
(To use this option, existing data must consist of all components required for eligibility by NC Policies Governing
Programs and Services for Children with Disabilities. The IEP Team completes eligibility worksheet(s) and
determination and proceeds as appropriate.) Provide parent with Handbook on Parents’ Rights.
Conduct Evaluation
What information is needed to determine if the student is or is not eligible for special education and related services?
Specify what areas of information are needed:
Obtain parent permission for evaluation and provide parent with Handbook on Parents’ Rights. Eligibility
determination, IEP (if eligible), and placement determination must be completed within 90 days of the date that the
school received the written referral. Complete compliance section below.
V. IEP TEAM. The following were present and participated in the referral meeting.
(Note with an * any team member who used alternative means to participate.)
Signature
Position
NOTICE OF PROCEDURAL COMPLIANCE TO BE COMPLETED BY SCHOOL:
Based on receipt of written referral, the ninety-calendar-day timeline for placement determination is
Copy given/sent to parent(s)
/
/
Date
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
.
Preschool Referral DEC 1 (2a of 4)
Student:
DOB:
/
/
PREVIOUS EARLY INTERVENTION SERVICES (EI):
Is this student currently transitioning from Part C-Infant/Toddler Program?
Date transition meeting from Part C-Infant Toddler Program was held:
yes
/
no
/
Who referred the child for EI services?
Age at which child started receiving EI services/child service coordination:
Age at which child stopped receiving EI services/child service coordination:
Frequency of EI services:
The student:
Has a current Individualized Family Service Plan (IFSP). Intervention goals include: (circle all that apply)
Cognitive
Adaptive
Communication
Fine Motor
Social/Emotional
Gross Motor
Behavior
Family Issues
Other:
Receives EI special instruction: (circle all that apply)
Speech/Language Therapy
Occupational Therapy
Physical Therapy
Developmental Instruction
Describe the progress the child has made on his/her IFSP goals:
Preschool Referral DEC 1 (2b of 4)
Student:
DOB:
/
/
REASON(S) FOR REFERRAL/AREAS OF CONCERN
Learning/Behavioral
difficulty remembering facts, details
fearful
asks for help too quickly
repeats same problem solving strategy,
short attention span for age
even when unsuccessful.
quickly abandons playing with toys
will not attempt difficult tasks
difficulty following directions
difficulty making transitions from one
destructive
activity to another.
physically aggressive with others
fearful of new situations
appears withdraw
cries easily
temper tantrums (describe)
consistent inappropriate emotional
reactions to situations/people
fights and/or bites
plays poorly with others (explain)
provokes/aggravates others/defiant
takes inappropriate risks
requires constant supervision
talks about hurting self or others
talks excessively, attention seeking
repeats same behavior over and over (explain)
other:
Communication
difficulty using spoken language
nonverbal
unable to communicate basic wants/needs
is not understood by familiar listener
speech is choppy, stuttering
has a vocabulary of less than 50 words
difficulty eating certain foods (list foods)
difficulty understanding language of others
is not understood by unfamiliar listener
voice constantly sounds hoarse
slow, labored speech
drools constantly
frequently chokes on liquids, food
frequent middle ear infections
Physical/Sensory
lacks age appropriate self-care (feeding, dressing/undressing, toileting, bathing)
impaired vision (explain)
date of last Opthamological exam:
impaired hearing (explain)
date of last Audiological exam:
/
/
date of last Otological exam:
/
lacks age appropriate gross motor skills
lacks age appropriate visual - motor skill
falls down easily, hurts him/herself frequently
lacks physical mobility at home/school
has seizures/epilepsy
cochlear implant: date of implantation:
/
/
overreacts to typical sights, sounds, tastes, textures
primary mode of communication (circle): signing, cueing, auditory-oral/verbal
(Parent Signature)
/
_____/_____/_____
(Date)
Consent for Evaluation/Reevaluation/Prior Notice DEC 2 Directions
Informed consent must be provided by parents for each proposed area of evaluation.
See Categories section of this handbook or DEC 20 for a complete listing of required screenings and
evaluations for each eligibility category.
IEP teams are obligated to conduct screenings and evaluations to address all areas of need regardless of the
suspected disability.
All area of need identified on the DEC 1 or DEC 7 must be included in the assessment measures checked.
In the event the IEP team determines during the evaluation process that other evaluations are needed, another
DEC 2 must be obtained. The team decision and consent may occur without a meeting.
The area of speech/language must be checked when it is determined that a communication evaluation is needed.
Consent for Evaluation/Reevaluation/Prior Notice DEC 2
PARENT/GUARDIAN/STUDENT AT AGE OF MAJORITY
CONSENT FOR EVALUATION/REEVALUATION
Check Purpose:
Student:
Dear
Initial Evaluation
Reevaluation
Grade:
School:
:
The IEP Team has recognized the need for gathering more information about your child. The proposed screening(s) and evaluation(s)
administered by qualified personnel will include the use of assessment instruments in the areas checked below to help identify
strengths, areas of concern and to determine the existence of a disability. Each LEA must conduct a full and individualized initial
evaluation before the initial provision of special education and related services to a child with a disability.
AREA
Physical Health
INFORMATION
Vision, hearing, medical screening/evaluation.
Educational
A variety of assessments measuring academic achievement and special abilities.
Psychological
Intellectual Assessment
A battery of tests and testing procedures measuring mental ability, behavioral/emotional
skills, perceptual development, and processing development. An intellectual assessment
may or may not yield an intellectual quotient (IQ) score.
Social Appraisal
Developmental history, social, personal, and behavioral.
Speech/Language
Understanding and using spoken language or using other modes of communication
screening/evaluation.
Motor
Visual motor integration, eye/hand coordination, fine and gross motor.
Adaptive Behavior
Functional behavior that is needed to meet the natural and social demands in one’s
environment, including daily living and self-help skills.
Vocational Evaluation
A comprehensive process involving an interdisciplinary team approach in assessing an
individual's vocational potential, training, and work placement needs.
Other
PARENT/GUARDIAN CONSENT
The results of these evaluations will be shared with you. You are entitled to a copy of the evaluation report(s).
Please sign A or B and return to:
Name:
Position:
A. YES, I give my permission for my child to receive evaluation or reevaluation services. I have received the Handbook on
Parents’ Rights that explains due process procedures.
Signature: _________________________________________________________
Date:
/
/
B. NO, I do not give my permission for my child to receive evaluation or reevaluation services. I have received the Handbook on
Parents’ Rights that explains due process procedures.
Signature: _________________________________________________________
Date:
/
/
This is the final action (decision) of the local education agency. If you disagree, you, as the parent or adult student, are entitled to the due process rights that are
described in your Handbook on Parents’ Rights (www.ncpublicschools.org/ec/policy/resources/rights). The deadline for filing a petition for a due process hearing is
one year (1 year) from receipt of this notice.
If you do not have a copy of the Handbook on Parents’ Rights or would like another one, please contact your school principal or call the local director of
Exceptional Children Programs. The principal or director can also help you understand your rights if you have any questions, or you can call the Exceptional
Children’s Assistance Center, 1-800-962-6817. Please save this notice for your records.
Copy given/sent to parent(s): / /
Summary of Evaluation/Eligibility Worksheet Directions
Use these directions for ALL of the Eligibility Worksheets
Summary of Evaluation/Eligibility Worksheets are disability specific based on the requirements for initial
placement.
Information documented on this worksheet provides a summary of assessment information gathered from all
sources (formal and informal assessments, beginning with the referral concerns, the review of existing
information and the evaluation process).
The summary of evaluation must be written in a manner that is understandable to all IEP team members,
including parents. Recording scores alone would not be sufficient.
The LEA is required to report the results of all screening and evaluation instruments completed through the
evaluation process including those that are not required components to determine eligibility.
Refer to definitions of individual screening and evaluations in NC Policies Governing Services for Children
with Disabilities.
Communication evaluation is not defined in NC Policies. A communication evaluation yields the same
information as a speech/language evaluation and may include augmentative and pragmatic assessments.
The Strengths/Needs section ensures that the team documents, reviews and discusses everything that has been
learned about the student from onset of the referral process, and through formal and informal assessment.
Review of existing information is gathered from the initial referral or the reevaluation determination.
Documenting the impairment is a requirement of North Carolina Policies Governing Services for Children with
Disabilities. There are specific criteria for each disability category; therefore, this section is included on each
eligibility worksheet and will vary depending on the disability. Directions for completing this section will also
vary, as teams may simply be required to “check” items or could be required to provide general statements,
summarizing the requested information.
Adverse effect on educational performance includes both academic and functional levels of performance.
Information gathered here, based upon the unique needs of the student, including how he/she learns and
demonstrates his/her knowledge, will guide the team in the development of an appropriate present level of
performance, should the student be determined eligible.
The team should consider the student’s response to scientific based interventions and the progress made during
the intervention process.
Academic levels of performance may include how the student is performing compared to age/grade level
standards in all academic areas.
Functional levels of performance may include daily living, social and behavior/emotional.
When ongoing evaluation of the problem indicates that expected progress is not being make and resources
beyond general education are needed, eligibility for special education may be considered.
Specially designed instruction means adapting, as appropriate, to the needs of an eligible child, the content,
methodology, or delivery of instruction.
Include a statement(s) that describes the intervention implemented and a review of existing data that document a
need for specially designed instruction.
DEC 3-AU (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-AUTISM SPECTRUM DISORDER
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
Hearing Screening:
Vision Screening:
/
/
/
/
/
/
/
/
Academic/Functional
Skills observations
across settings:
Summary of conference
with parent(s) or
documentation of
attempts to conference:
Social/Developmental
History:
Educational Evaluation:
/
/
Adaptive Behavior:
/
/
Psychological
Evaluation:
/
/
/
/
Speech/Language
Evaluation which
includes but is not
limited to measures of
language, semantics,
and pragmatics:
Behavioral Assessment
related to Autism
Spectrum Disorder:
/
/
Summary of Required Screenings and Evaluations
Pass
Pass
Fail
Fail
dB (Intensity Level)
Far R 20/
L 20/
Near R 20/
L 20/
Hz (Frequencies)
Other:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
DEC 3-AU (2 of 2)
Student:
School:
DOB:
/
Grade:
Documentation of impairment in the following areas (MUST demonstrate impairment at least three of four):
A. Communication:
B. Social Interaction:
C. Sensory Responses/Experiences:
D. Restricted, repetitive, or stereotypic patterns of behavior, interests, and/or activities:
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
/
DEC 3-DB (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-DEAF/BLINDNESS
Student:
DOB:
School:
/
Grade:
Date
Instrument
/
/
Motor Screening:
/
/
/
/
/
/
Academic and
functional skills
observation across
settings:
Summary of conference
with parent(s) or
documentations of
attempts to conference
with parent(s):
Social/Developmental
History:
/
/
Educational Evaluation:
/
/
Adaptive Behavior
Evaluation:
/
/
Psychological
Evaluation:
/
/
/
/
Communication
Evaluation including
receptive, expressive,
and augmentative
communication skills:
Audiological
Evaluation:
/
/
Otological (when
appropriate):
/
/
/
/
Medical Evaluation
including health history,
precautions, and
medications :
Ophthalmological or
optometric Evaluation:
/
/
Other:
Summary of Required Screenings and Evaluations
/
DEC 3-DB (2 of 2)
Student:
School:
DOB:
/
/
Grade:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
Documentation of impairment in the following areas (MUST address all three):
A. Visual impairment in combination with hearing impairment:
B. Severe communication, developmental and educational needs:
C. Needs cannot be met in a program designed solely for visually impaired or hearing impaired:
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
DEC 3-Deafness/HI (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEETDEAFNESS OR HEARING IMPAIRMENT
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
Vision Screening:
/
/
/
/
Usher Syndrome
Screening:
( 12 years and older)
Motor Screening
/
/
Social/Developmental
History:
/
/
/
/
/
/
Academic/Functional
Skills Observation
across settings:
Summary of conference
with parent(s) or
documentations of
attempts to conference
with parent(s):
Educational Evaluation:
/
/
/
/
/
/
/
/
Summary of Required Screenings and Evaluations
Pass
Fail
Far R 20/
Near R 20/
L 20/
L 20/
Communication
Evaluation, including
receptive, expressive,
and augmentative
communication skills:
Otological Evaluation to
provide a diagnosis of
middle and inner ear
disorders:
Audiological Evaluation
including air conduction,
bone conduction, and
speech reception testing
with and without
amplification, and
impedance testing to
determine type of any
hearing loss that may
be present:
Other:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
DEC 3-Deafness/HI (2 of 2)
Student:
School:
Documentation of impairment in the following areas: (must address all three)
Hearing loss:
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
DOB:
/
Grade:
/
DEC 3-DD (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-DEVELOPMENTAL DELAY
(Ages 3 through 7)
Student:
DOB:
School:
/
/
Grade:
/
/
Hearing Screening:
/
/
Vision Screening:
/
/
Motor Screening:
/
/
Health Screening:
/
/
Speech/Language
Screening:
/
/
/
/
/
/
Academic and Functional
Skills Observation across
settings:
Summary of conference
with parent(s) or
documentations of
attempts to conference
with parent(s):
Social/Developmental
History:
/
/
Educational Evaluation:
/
/
Adaptive Behavior
Evaluation:
/
/
/
/
Psychological Evaluation
(including cognitive and
social/emotional
measures):
Other:
Pass
Fail
Method of Screening:
Pass
Fail
Method of Screening:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about the student?
Strengths:
Needs:
DEC 3-DD (2 of 2)
Student:
School:
DOB:
/
/
Grade:
Documentation of impairment with A and/or B:
A. Delayed/Atypical Development in one or more of the following areas: physical, cognitive, communication, social/emotional, or
adaptive: (30% delay in an assessment that yields scores in months or 2 or more standard deviations below the mean on
standardized tests in one area; or 25% delay in an assessment that yields scores in months or 1.5 or more standard deviations below
the mean on standardized tests in two or more areas.)
B. Delayed/Atypical behavior(s) that is so significantly inadequate or inappropriate that it interferes with the child’s ability to learn
and/or cope with normal situational or environmental demands. Must be evidenced that the patterns of behavior occur in more than
one setting over an extended period of time. List documentation required by NC Regulations for specific age criteria.
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
DEC 3-SED (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-SERIOUS EMOTIONAL DISABILITY
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
Hearing Screening:
Vision Screening:
/
/
/
/
/
/
Two research-based
interventions to address
behavior/emotional skill
deficiencies and
documentation of the
results of the
interventions:
Summary of conference
with parent(s) or
documentation of
attempts to conference:
Communication
Evaluation:
/
/
Review of Existing
Data:
/
/
Social/Developmental
History:
/
/
/
/
Academic, Functional
and Behavioral
Observation across
settings:
Educational Evaluation:
/
/
/
/
/
/
Psychological
Evaluation (to include
an intellectual
evaluation):
Behavioral/Emotional
Evaluation (which may
include a behavioral/
emotional skill rating):
Other:
Summary of Required Screenings and Evaluations
Pass
Pass
Fail
Fail
dB (Intensity Level)
Far R 20/
L 20/
Near R 20/
L 20/
Hz (Frequencies)
DEC 3-SED (2 of 2)
Student:
DOB:
School:
/
/
Grade:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
Documentation of impairment in one the following areas:
A. An inability to make educational progress that cannot be explained by intellectual, sensory, or health factors.
B. An inability to build or maintain satisfactory interpersonal relationships with peers and teachers:
C. Inappropriate types of behaviors or feelings under normal circumstances:
D. A general pervasive mood of unhappiness or depression:
E. A tendency to develop physical symptoms or fears associated with personal or school problems:
F. A diagnosis of schizophrenia:
Documentation that the above condition(s) have been exhibited over a long period of time and to a marked degree:
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
DEC 3-ID (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-INTELLECTUAL DISABILITY
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
Hearing Screening:
Vision Screening:
/
/
Health Screening:
/
/
Motor Screening:
/
/
Speech/Language
Screening:
/
/
/
/
/
/
Two research based
interventions to address
academic and/or functional
skill deficiencies and
documentation of the
results of the interventions:
Summary of conference
with parent(s) or
documentation of
attempts to conference:
Review of Existing Data:
/
/
Social/Developmental
History:
/
/
/
/
Academic/Functional and
Behavior Skills
observations across
settings:
Educational Evaluation:
/
/
Adaptive Behavior
Evaluation:
/
/
Psychological Evaluation
(including an intellectual
evaluation):
/
/
Other:
Summary of Required Screenings and Evaluations
Pass
Pass
Fail
Fail
dB (Intensity Level)
Far R 20/
L 20/
Near R 20/
L 20/
Hz (Frequencies)
DEC 3-ID (2 of 2)
Student:
School:
DOB:
/
/
Grade:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
Documentation of impairment in the following areas:
A. Intellectual functioning at one of the following levels on an individually administered standardized intelligence test:
a) Mild: two standard deviations below the mean plus or minus the standard error of measure:
b) Moderate: three standard deviations below the mean plus or minus the standard error of measure:
c) Severe: four or more standard deviations below the mean plus or minus the standard error of measure:
B. Adaptive behavior deficits at or below: a) two standard deviations below the mean in one domain or b) one and one-half standard
deviations below the mean in two or more domains.
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
DEC 3-MU (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-MULTIPLE DISABILITIES
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
Hearing Screening:
Vision Screening:
/
/
/
/
/
/
/
/
Social/Developmental
History:
Summary of
conference(s) with
parents or
documentation of
attempts to conference
with parent(s):
Academic and
Functional Skills
Observation across
settings:
Educational Evaluation:
/
/
Adaptive Behavior
Evaluation:
/
/
Psychological
Evaluation:
/
/
Speech/Language
Evaluation:
/
/
Medical Evaluation:
/
/
Motor Evaluation:
/
/
Other:
Summary of Required Screenings and Evaluations
Pass
Pass
Fail
Fail
dB (Intensity Level)
Far R 20/
L 20/
Near R 20/
L 20/
Hz (Frequencies)
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
DEC 3-MU (2 of 2)
Student:
School:
DOB:
/
Grade:
Documentation of impairment in the following area(s):
A. Two or more disabilities occurring together:
B. Severity and complexity of educational needs is such that they cannot be accommodated in a program solely for one of the
disabilities:
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
/
DEC 3-OI (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-ORTHOPEDIC IMPAIRMENT
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
Hearing Screening:
Vision Screening:
/
/
Social/Developmental
History:
/
/
/
/
/
/
Summary of
conference(s) with
parents or
documentation of
attempts to conference
with parent(s):
Academic and
Functional Skills
Observation across
settings:
Educational Evaluation:
/
/
Medical Evaluation:
/
/
Motor Evaluation:
/
/
Other:
Summary of Required Screenings and Evaluations
Pass
Pass
Fail
Fail
dB (Intensity Level)
Far R 20/
L 20/
Near R 20/
L 20/
Hz (Frequencies)
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
DEC 3-OI (2 of 2)
Student:
School:
Documentation of impairment in the following area(s):
A severe physical impairment:
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
DOB:
/
Grade:
/
DEC 3-OHI (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-OTHER HEALTH IMPAIRMENT
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
Hearing Screening:
Vision Screening:
/
/
/
/
/
/
Two research based
interventions to address
academic and/or
functional skill
deficiencies and
documentation of the
results of the
interventions:
Summary of conference
with parent(s) or
documentation of
attempts to conference:
Academic and,
Functional Observation
across settings:
/
/
Social/Developmental
History:
/
/
Educational Evaluation:
/
/
Medical Evaluation:
/
/
Other:
Summary of Required Screenings and Evaluations
Pass
Pass
Fail
Fail
dB (Intensity Level)
Far R 20/
L 20/
Near R 20/
L 20/
Hz (Frequencies)
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
DEC 3-OHI (2 of 2)
Student:
School:
DOB:
/
/
Grade:
Documentation of impairment in the following areas:
A chronic or acute health problem along with one or more of the following:
A) Limited strength:
B) Limited vitality:
C) Limited alertness, including heightened alertness to environmental stimuli that results in limited alertness with respect to the
educational environment:
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
MOORE COUNTY SCHOOLS
_______________________
P. O. Box 1180 – Carthage, North Carolina 28327 – 910/947-2976 – FAX 910/947-3011
MEDICAL STATEMENT
Name:_________________________________DOB: ______________
Definition: Other health impaired students have chronic or acute health problems which cause limited strength,
vitality or alertness to such an extent that special educational services are necessary. The health problems may
include heart conditions, chronic lung disease, tuberculosis, rheumatic fever, nephritis, asthma, sickle cell
anemia, hemophilia, epilepsy, lead poisoning, leukemia, diabetes, genetic impairments or some other illness
which may cause a student to have limited strength, vitality or alertness, adversely affecting educational
performance or developmental progress.
Diagnosis: ______________________________________________________________________________
__________________________________________________________________
Briefly describe how this condition adversely affects the student’s educational performance or developmental
progress. Please explain how it impacts on this student’s alertness, strength, and/or vitality:_______________
________________________________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
Does this student’s health problem significantly affect attendance? ( ) Yes ( ) No Explain: _______________
________________________________________________________________________________________
________________________________________________________________________________________
Does the health problem require medication that can impact on strength, vitality, and/or alertness? ( ) Yes ( ) No
If yes, please explain ______________________________________________________________________
_______________________________________________________________________________________
Will the child need medication and/or medical procedures administered during the school day? What special
training, if any, will school personnel need for this?______________________________________________
_______________________________________________________________________________________
Does the child have any restrictions or limitations (e.g. PE) or need special accommodations? ( ) Yes ( ) No
If yes, please explain: _____________________________________________________________________
_______________________________________________________________________________________
Physician’s Signature _________________________________
Date__________________
Print Name ________________________________
Title __________________
Address __________________________________
Phone _________________
__________________________
DEC 3-SLD (1 of 2)
Discrepancy/Alt to Discrepancy Model
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-SPECIFIC LEARNING DISABILITY
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
/
/
/
/
/
/
/
/
/
/
Social/Developmental
History:
/
/
/
/
Academic, Functional
and Behavioral
Observation across
settings:
Educational Evaluation:
/
/
/
/
Discrepancy Model:
Hearing Screening:
Vision Screening:
Speech/Language
Screening:
Two research-based
interventions to address
academic skill
deficiencies and
documentation of the
results of the
interventions, including
progress monitoring
documentation:
Summary of
conference(s) with
parent(s) or
documentation of
attempts to conference:
Review of Existing
Data:
Psychological
Evaluation (to include
an intellectual
evaluation):
Other:
Summary of Required Screenings and Evaluations
Pass
Fail
Pass
Fail
dB (Intensity Level)
Far R 20/
Near R 20/
L 20/
L 20/
Hz (Frequencies)
DEC 3-SLD (2 of 2)
Discrepancy/Alt to Discrepancy Model
Student:
DOB:
School:
/
/
Grade:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student? Include characteristics of a specific learning disability consistent with the definition.
Strengths:
Needs:
Document the impairment in the Discrepancy/Alternative to Discrepancy Method:
Discrepancy:
A. Inadequate achievement to meet age, or State-approved grade level standards as evidenced by a discrepancy between
achievement and measured ability of at least 15 points in one or more of the following areas:
Oral Expression
Listening Comprehension
Written Expression
Basic Reading Skills
Reading Fluency Skills
Reading Comprehension
Mathematics Calculation
Mathematical Problem Solving
OR
A pattern of strengths and weaknesses in performance, achievement, or both relative to age, State-approved grade-level
standards, or intellectual development.
B.
Insufficient progress to meet age or State-approved grade-level standards in one or more of the areas identified above in
(A) of this section when using a process based on the student’s response to scientific, research-based intervention.
Alternate to Discrepancy:
A.
Documentation that the assessment measures did not accurately reflect the discrepancy between achievement and ability;
B.
Documentation of the assessment measures used, the assessment results, the criteria applied to judge the importance
of the difference between expected and current achievement.
Attach documentation gathered for (A) and (B) above and used in the determination of the presence of a substantial
discrepancy in the student's performance.
For either approach used above, have the following factors been ruled out as the primary cause of the disability: sensory or motor
deficits, intellectual or serious emotional disabilities, environmental, cultural, linguistic, or economic influences, or lack of instruction
in reading or math?
YES
NO
If “NO”, describe which factor(s) are the primary contributors to the academic delay.
Note: The child cannot be considered eligible as SLD if the response is ‘NO”.
What is the adverse effect on educational performance? (Include a statement of the relationship of the behavior
noted during the observation to the student’s academic functioning. Also, address the effect of any applicable
educationally relevant medical findings.)
What evidence exists that the student requires specially designed instruction?
IEP TEAM MUST COMPLETE ELIGIBILITY DETERMINATION.
DEC 3-SLD (1 of 2)
Responsiveness to Instruction Model
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-SPECIFIC LEARNING DISABILITY
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
Hearing Screening:
Vision Screening:
/
/
Review of Existing
Data:
/
/
/
/
/
/
Research based
interventions to address
academic skill
deficiencies and
documentation of the
results of the
interventions:
Summary of
conference(s) with
parent(s) or
documentation of
attempts to conference:
Social/Developmental
History:
/
/
/
/
/
/
Academic, Functional
and Behavioral
Observation across
settings:
Speech/Language
Screening:
Other:
Summary of Required Screenings and Evaluations
Pass
Pass
Fail
Fail
dB (Intensity Level)
Far R 20/
L 20/
Near R 20/
L 20/
Hz (Frequencies)
DEC 3-SLD (2 of 2)
Responsiveness to Instruction Model
Student:
DOB:
School:
/
/
Grade:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student? Include characteristics of a specific learning disability consistent with the definition.
Strengths:
Needs:
Based on information from multiple sources, provide documentation of significant delays in the following:
A. Inadequate achievement to meet age, or State-approved grade level standards in one or more of the following areas:
Oral Expression
Listening Comprehension
Written Expression
Basic Reading Skills
Reading Fluency Skills
Reading Comprehension
Mathematics Calculation
Mathematical Problem Solving
OR
A pattern of strengths and weaknesses in performance, achievement, or both relative to age, State-approved
grade-level standards, or intellectual development.
B.
Insufficient progress to meet age or State-approved grade-level standards in one or more of the areas identified above
in (A) of this section; or the IEP team determines the students needs an intervention, in order to make sufficient
progress, that requires resources beyond what can be reasonably provided in general education.
Have the following factors been ruled out as the primary cause of the disability: sensory or motor deficits,
intellectual or serious emotional disabilities, environmental, cultural, linguistic, or economic influences, or lack
of instruction in reading or math?
YES
NO
If “NO”, describe which factor(s) are the primary contributors to the academic delay.
Note: The child cannot be considered eligible as SLD if the response is ‘NO”.
What is the adverse effect, if any, on educational performance?
What evidence, if any, exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
DEC 3-SI (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-SPEECH/LANGUAGE IMPAIRED
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
Date
Summary of Required Screenings and Evaluations
Instrument
Summary of Required Screenings and Evaluations
Pass
Fail
dB (Intensity Level)
Method of Screening (if availability):
/
/
Hearing Screening:
/
/
Articulation Screening:
/
/
Fluency Screening:
/
/
Language Screening:
/
/
/
/
/
/
Voice/Resonance
Screening:
Summary of
conference(s) with
parent(s) or
documentation of
attempts to conference:
Social/Developmental
History:
/
/
/
/
/
/
/
/
• Fluency;
/
/
• Language (including
form, content, and
function); or
/
/
• Voice/resonance;
/
/
Academic, Functional
and Behavioral
Observation across
settings:
Educational Evaluation:
One of the following
evaluations, based on
screening results,
individualized to
address the specific
area(s) of concern:
• Articulation;
Other:
Hz (Frequencies)
DEC 3-SI (2 of 2)
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
Documentation of impairment in one or more of the following areas:
A.
Articulation-Two or more phonemic errors and/or phonological processes not expected at the child’s age or developmental
level;
B.
Fluency-Demonstration of non-fluent speech behavior;
C.
Language-Standard scores on an evaluation instrument suggest a language disorder and /or non-standardized/informal
assessment indicates that the child has difficulty understanding and or expressing ideas and/or concepts (language); or
D. Voice-Demonstration of consistent deviations in vocal production that are inappropriate for chronological/mental age, gender,
and ability.
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
DEC 3-TBI (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-TRAUMATIC BRAIN INJURY
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
/
/
/
/
Hearing Screening:
Vision Screening:
Speech/Language
Screening:
Two research-based
interventions to address
academic and/or
behavioral skill
deficiencies and
documentation of the
results of the
interventions:
*Note: Screenings listed
above may be waived for
students who have been
medically diagnosed with
traumatic brain injury and
who have received medical
and/or rehabilitative
services in a medical or
rehabilitation program or
setting within the previous
twelve months.
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
Review of medical
history and records:
Review of educational
history and records:
Summary of
conference(s) with
parent(s) or
documentation of
attempts to conference:
Social/Developmental
History:
Academic, Functional
and Behavioral Skills
Observation across
settings:
Educational Evaluation:
Psychological Evaluation
which is current within
one year and is
conducted by a qualified
professional described
in NC Regulations:
Motor Evaluation:
Other:
Summary of Required Screenings and Evaluations
Pass
Fail
dB (Intensity Level)
Hz (Frequencies)
DEC 3-TBI (2 of 2)
Student:
School:
DOB:
/
/
Grade:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
Documentation of impairment in the following areas:
Written verification of traumatic brain injury (e.g., that the child has sustained an injury from which brain injury can be inferred) by
a licensed physician or licensed psychologist (appropriately practicing in the specialty of neuropsychology). No time limits exist
for written verification.
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
DEC 3-VI (1 of 2)
SUMMARY OF EVALUATION/ELIGIBILITY WORKSHEET-VISUAL IMPAIRMENT
Student:
DOB:
School:
/
/
Grade:
Date
Instrument
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
Hearing Screening:
Summary of
conference(s) with
parent(s) or
documentations of
attempts to conference:
Social/Developmental
History:
Educational Evaluation:
Ophthalmological or
optometric Evaluation:
For school age
children:
Academic, Functional
and Behavioral
Observation across
settings (address
expanded core
curriculum):
Braille Skills Inventory
and/or Learning Media
Assessment:
Functional Vision
Assessment:
For preschool children:
Observation across
settings to include:
• Physical, behavioral,
and environmental
characteristics;
• Shutting or covering
one eye, tilting head
or thrusting head
forward, squinting
eyelids together;
• Difficulty with tasks
requiring vision;
• Avoidance of near
work tasks or irritation
when required to do
near work;
• Inability to see
distant objects;
• Difficulty with
navigation;
• Eye appearance
(eg. crossed-eyes
or nystagmus)
Other:
Summary of Required Screenings and Evaluations
Pass
Fail
dB (Intensity Level)
Hz (Frequencies)
DEC 3-VI (2 of 2)
Student:
School:
DOB:
/
/
Grade:
As a result of the required screenings, evaluations, and review of existing information, what do we now know about
the student?
Strengths:
Needs:
Documentation of impairment in one the following areas:
A. Visual acuity between 20/70 and 20/200 in the better eye after correction:
B. Visual acuity of 20/200 or less in the better eye after correction or a peripheral field so contracted that the widest diameter
subtends an arc no greater than 20 degrees to be considered legally blind.
What is the adverse effect on educational performance?
What evidence exists that the student requires specially designed instruction?
AFTER COMPLETING WORKSHEET, IEP TEAM MUST DETERMINE ELIGIBILITY.
(See Eligibility Determination Form)
Eligibility Determination (DEC 3) Directions
Sources include information gathered during the referral process, reevaluation process, formal and informal
assessments, records review, etc.
At time of reevaluation, attach individual eligibility worksheets if additional data was collected in order to
determine continued eligibility.
Refer to the Summary of Evaluation/Eligibility Worksheet in responding to the following statements.
At time of reevaluation if no additional data was collected, refer to the review of existing data documented on
the DEC 7 in responding to the questions on adverse effects and specially designed instruction
Eligibility determination must be made for the primary category of disability, and, as applicable, for the
secondary category(s) of disability. Speech or language impaired is one of the fourteen disability categories. It
is a related service when it is needed for a student to benefit from special education.
Related services are not disability categories and do not have specified eligibility criteria. The need for related
services must be based on data and determined by the IEP team. (Why is this service needed or not needed for
this student to benefit from special education?)
For a student who is already identified as a student with a disability, adding or discontinuing a related
service will be done through the reevaluation process, which may or may not include formal
assessment(s). The reevaluation process resets the date for the required reevaluation.
IDEA requires signatures regarding the eligibility determination for students with specific learning disabilities.
While signatures are not required by state law for other areas of eligibility, Moore County does require this
form to be signed for all areas of eligibility.
Eligibility Determination DEC 3
ELIGIBILITY DETERMINATION
Check Purpose:
Initial Eligibility
Reevaluation
Student:
Grade:
School:
The IEP Team has summarized all required screening and evaluation information including a discussion of the student’s strengths and
needs on attached evaluation/eligibility worksheet(s).
Based on information from a variety of sources that have been documented and carefully considered, the IEP Team has determined:
yes
no
The student meets criteria for one or more of the fourteen disabling conditions consistent with the definitions
described in NC Policy 1500-2 (must attach individual eligibility worksheets);
yes
no
The disability has an adverse effect on educational performance; and
yes
no
The disability requires specially designed instruction.
All three must be yes in order for the student to be eligible for special education and related services if required to benefit from
special education.
The IEP Team has also concluded:
yes
no
The determination is not the result of lack of appropriate instruction in reading, including the essential
components of reading instruction. The term “essential components of reading instruction” means explicit and
systematic instruction in: phonemic awareness, phonics, vocabulary development, reading fluency (including
oral reading skills), and reading comprehension strategies.
yes
no
The determination is not the result of lack of appropriate instruction in math; and
yes
no
The determination is not the result of Limited English proficiency of the student.
All three must be yes in order for the student to be eligible for special education and related services if required to benefit from
special education.
Statement of Eligibility:
,
is eligible for special education and related services if required to benefit from special education. He/she meets the eligibility
criteria for
(primary eligibility category) and
(secondary eligibility category(s), if applicable). (Attach
individual eligibility worksheets for all identified areas of eligibility.)
is not eligible for special education and related services.
IEP Team Signatures
SLD Only*
Agree
Disagree
Agree
Disagree
Agree
Disagree
Agree
Disagree
Agree
Disagree
Agree
Disagree
Agree
Disagree
Agree
Disagree
*For SLD only. If an IEP Team member disagrees, he/she must submit a separate statement of their reason for disagreement.
Copy given/sent to parent(s)
Position
/
/
Date of Meeting
Individualized Education Program (DEC 4 pg. 1) Directions
The “Student Profile” is a springboard for the development of the IEP.
Strengths should include attributes of the child that may go beyond the scope of academic/functional
performance that will help facilitate planning appropriate instruction and enable the student to access and be
successful in the general curriculum.
N/A should not be indicated when noting parental concerns. Simply note that the parent did not participate in
the IEP or participated but indicated no concerns.
N/A should not be indicated when noting parent’s/student’s vision for student’s future. Simply note that the
parent/student did not participate in the IEP or participated but did not indicate a vision statement.
LEAs are not prohibited from inviting students to participate in the development of their IEP prior to their
fourteenth birthday, recognizing that participation can occur in multiple ways.
Facilitating a smooth process depends on the individual needs of the child and the nature of the anticipated
transition. For example, a student will be moving mid-year. The parent has expressed concerns about the
student’s inability to manage change. In this instance, this section may include a description of steps outlining
correspondence with the new school and teacher/staff, well in advance of the move in order to ensure the
student can continue to make progress toward his/her annual goals.
IEP DEC 4 (1 of 10)
Check Purpose:
Initial
Annual Review
Reevaluation
Addendum
Transition Part C to B
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
Duration of Special Education and Related Services: From:
/
/
To:
/
/
Student:
DOB:
School:
Primary Area of Eligibility*
/
/
Grade:
Secondary Area(s) of Eligibility: (if applicable)
(*Reported on Child Count)
Student Profile
Student’s overall strengths:
Summarize assessment information (e.g. from early intervention providers, child outcome measures, curriculum based
measures, state and district assessments results, etc.), and review of progress on current IEP/IFSP goals:
Parent’s concerns, if any, for enhancing the student’s education:
Parent’s/Student’s vision for student’s future:
Consideration of Transitions
If a transition (e.g. new school, family circumstances, etc.) is anticipated during the life of this IEP/IFSP what information
is known about the student that will assist in facilitating a smooth process?
N/A
The student is age 14 or older or will be during the duration of the IEP.
Yes
No
IEP (DEC 4 pg. 2) Directions
For all students who have identified special factors, consideration must be given to any service, intervention,
device, accommodation and/or other program modification that may be needed in order for the student to
receive FAPE.
For any student whose behavior is impeding his/her learning, regardless of disability category, the IEP team
must address the behavior either through an annual goal (what the student will learn), a behavior intervention
plan (interventions/instruction adults provide on behalf of the student) or both.
Behavior Intervention Plans are part of the IEP.
When answering the question on special communication needs check “yes” for students who are speech
primary or receive speech as a related service and any others who have special communication needs.
If you answer yes to the student being deaf or hard of hearing, all of the following boxes must be discussed and
there is a worksheet to help answer each of those components. The worksheet is located in the forms section
of this handbook.
If you answer yes to specially designed physical education, a present level of performance, goals, and shortterm objectives/benchmarks (as required) must be developed in consultation with individual(s) knowledgeable
of the physical education curriculum and the student’s motor skills.
IEP DEC 4 (2 of 10)
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
Duration of Special Education and Related Services: From:
/
/
To:
/
/
Student:
DOB:
School:
/
/
Grade:
Consideration of Special Factors (Note: If you check yes, you must address in the IEP.)
Does the student have behavior(s) that impede his/her learning or that of others?
Does the student have Limited English Proficiency?
Yes
Yes
No
If the student is blind or partially sighted, will the instruction in or use of Braille be needed?
Does the student have any special communication needs?
Is the student deaf or hard of hearing?
Yes
No
Yes
Yes
No
N/A
No
No
The child’s language and communication needs;
Opportunities for direct communications with peers and professional personnel in the child’s language and communication mode;
Academic level;
Full range of needs, including opportunities for direct instruction in the child’s language; and
Communication mode.
(Communication Plan Worksheet available at www.ncpublicschools.org/ec/policy/forms.)
Does the student require specially designed physical education?
Yes
No
IEP (DEC 4 pg. 3) Directions
Using current/relevant formal/informal evaluation data, a present level of performance must be completed in
order to develop each area from which annual goal(s) will be developed.
The present level of performance should be comprehensive for each area of need. Annual goals must originate
from the present level of performance, and must be reasonably calculated to be addressed within one year.
The major components of the present level of performance are the specific strengths and needs in academic and
functional areas that establish a baseline in describing where the student is currently performing. The team may
also include any additional information known about the student and his/her learning style.
Standardized scores and grade level alone do not reflect strengths and needs.
Functional performance must be addressed for all students within the present level of performance, and annual
goals, developed as appropriate.
Federal Regulations require that student assessed through modified achievement standards have annual goals
aligned to grade level competencies. In North Carolina, students in grade 3-8, & 10 who are assessed via the
Extend2 are subject to this requirement.
In determining the competency goal, the IEP team is instructed to consider the developed present level of
performance of each academic/functional area, and align it with a selected grade level competency(s) from the
NC Standard Course of Study reflecting the student’s current grade placement. The skills that the student needs
to develop in order to obtain the competency(s) become annual goals.
Teams are instructed to write annual goals based on the skill needs of the student, not subject areas. Therefore,
science competency(s) may be selected and referenced as part of language arts or math goals.
LEAs may require standards-based IEPs for all students.
IEP DEC 4 (3 of 10)
Complete Pages 3-4 for Each Annual Goal
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
Duration of Special Education and Related Services: From:
/
/
To:
/
/
Student:
DOB:
School:
/
/
Grade:
Present Level(s) of Academic and Functional Performance
Include specific descriptions of what the student can and cannot do in relationship to this area. Include current academic
and functional performance, behaviors, social/emotional development, other relevant information, and how the student’s
disability affects his/her involvement and progress in the general curriculum.
Annual Goal
Academic Goal
Functional Goal
Does the student require assistive technology devices and/or services?
If yes, describe needs:
Yes
No
(Address after determination of related services.) Is this goal integrated with related service(s)?
*If yes, list the related service area(s) of integration:
Yes*
No
IEP (DEC 4 pg. 4) Directions
Annual goals address academic/functional areas. They may be measurable and provide a direction for change.
The annual goal must be reasonably calculated to be accomplished within the life of the IEP, not to exceed one
year.
If a student requires assistive technology, it must be documented either as an annual goal or through
supplemental aids and services.
If an annual goal is integrated (more than one provider working towards the same annual goal), progress
monitoring must be conducted by each individual from his/her individual perspective. Integrated annual goals
are one example of highly collaborative IEP teams.
Benchmarks consist of who will do what by when.
Short Term Objectives consist of who will do what under what conditions (optional) and a level of
attainment/objective criteria.
When benchmarks/short-term objectives are used, a minimum of two must be listed per annual goal.
Individuals are required to maintain (in a separate location) data to support the progress noted toward annual
goals.
Examples include a record of teacher observation(s), teacher made test(s), log(s), chart(s), project(s),
portfolio(s), work sample(s), journal(s), etc.
IEP DEC 4 (4 of 10)
Complete Pages 3-4 for Each Annual Goal
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
Duration of Special Education and Related Services: From:
/
/
Student:
To:
/
/
DOB:
School:
/
/
Grade:
Competency Goal
Required for areas (if any) where student participates in state assessments using modified achievement standards.
Select Subject Area:
Language Arts
Mathematics
Science
List Competency Goal from the NC Standard Course of Study:
(Standard must match the student’s assigned grade.)
Note: Selected Grade Standard Competency Goals listed are those identified for specially designed instruction. In addition to those
listed, the student has access to grade level content standards through general education requirements.
Benchmarks or Short Term Objectives (if applicable)
(Required for students participating in state alternate assessments aligned to alternate achievement standards)
Describe how progress toward the annual goal will be measured
IEP (DEC 4 pg. 5) Directions
Students with disabilities must be considered general education students first.
To complete this section, IEP teams must discuss all of the classes, nonacademic services and activities in
which the student will participate with his/her non-disabled peers.
Complete the chart with as much specificity as possible. Testing accommodations for state and district-wide
assessments must be addressed for general education program participation and for special education testing and
instruction.
Any supplemental aids, services, modifications/accommodations, including test accommodations must be
supported by documented student characteristics in the present level of performance, other areas of the IEP such
as special factors, or the student’s record.
General education teachers, as part of the IEP team, will participate in the determination and implementation of
the supplemental aids/services, modifications/accommodations, and assistive technology identified.
Teams should discuss and document any technical assistance that is necessary for general education teachers or
other school personnel to implement the IEP.
Any individual(s), including general education teacher(s), who have responsibility in implementing the IEP,
must be informed of those responsibilities.
LEAs must develop a mechanism to disseminate this information to ensure implementation. Moore County
requires each case manager to disseminate this information to all necessary people.
IEP DEC 4 (5 of 10)
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
Duration of Special Education and Related Services: From:
/
/
To:
/
/
Student:
DOB:
School:
/
/
Grade:
Least Restrictive Environment
I. General Education Program Participation
In the space provided, list the general education classes, nonacademic services, and activities (ex: lunch, recess,
assemblies, media center, field trips, etc.) in which the student will participate and the supplemental aids, supports,
modifications, and/or accommodations required (if applicable) to access the general curriculum and make progress
toward meeting annual goals. Discussion and documentation must include any test accommodations required for
state and/or district-wide assessment. If supplemental aids/services, modifications/ accommodations and/or
assistive technology will be provided in special education classes include in the table below.
General
Education/Special
Education
Nonacademic Services
& Activities
(If Applicable)
Supplemental Aids/Services
Modifications/Accommodations
Assistive Technology (If Applicable)
Implementation Specifications
(Example: Who? What? When? Where?)
If the student is in preschool, describe how the student is involved in the general education program.
N/A
Specify the technical assistance, if any, that will be provided to the general education teacher(s) and/or other
school personnel for implementation of the IEP.
None
IEP (DEC 4 pg. 6) Directions
Teams are instructed to complete the testing accommodation grid with accuracy. Individuals who are
responsible for implementation of the accommodations in the classroom must be informed of their
responsibilities.
IEP DEC 4 (6 of 10)
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
Student Name:
Duration From:
/
/
To:
/
/
II. North Carolina Assessment Program
Select the appropriate state assessment(s) that will allow the student to demonstrate his/her knowledge. Select testing accommodations
that correlate to classroom accommodations used routinely throughout the academic year. Accommodations that are listed on the IEP
must be used on a routine basis in classroom instruction. For specifics regarding accommodation use and availability for specific tests,
refer to the Testing Students with Disabilities publication, available at http://www.ncpublicschools.org/accountability/policies/tswd.
Braille Edition
Computer Skills Portfolio
Large Print Edition
One Test Item Per Page
Assistive Technology: Specify
_______________________
Braille Writer/Slate and Stylus (and Braille Paper)
Crammer Abacus
Dictation to scribe
For Writing assessment, will not receive valid conventions score.
Interpreter/ Transliterator Signs/Cues Test
Not for test of reading skills
Keyboarding Devices
Magnification Devices
Student Marks in Answers in Test Book
Student Reads Aloud to Self
Test Administrator
Reads Test Aloud Not
for test
of reading skills
Read Everything
Read by Student Request
Other
Hospital/Home Testing
Multiple
Test
Sessions
More Frequent Breaks (Every
Min.)
Over Multiple Days (Number of Days
Approximately 30 minutes
Scheduled
Extended Time
Approximately 1 Hour
Other
)
Competency
Tests
Math 1
Life Skills Science
1&2
Verbal
End of
Math
High
School
Reading
EOC
Occupational Course Test
Course of Study
English1
Science
Math
Grades
3–8
Writing
3-8 or
OCS
NC Extend2
Reading
NC Testing Program
Approved Accommodations
Science
Reading
Student will participate in
the Extend 1.
Math
End of Grade
NC
Tests
Writing
Test
(Grade 3
Pretest
Grades
& Grades
4, 7,
3 – 8)
and 10
Standard Test Administration
with no Accommodations
Test of Computer
Skills –Begins
Grade 8
IEP Teams are instructed to select for each assessment, only those accommodations that do not invalidate the score.
Testing in
Separate Room
Small Group
One-on-One
Computer/typewriter/word processor
NCCLAS
IEP (DEC 4 pg.7) Directions
LEAs should contact the testing coordinator for a list of district-wide assessments. Alternate assessments must
be available to students if the LEA conducts district-wide assessments. If no district-wide assessments are
administered, please indicate N/A
The Alternate Assessment Justification section must be completed for any student who is participating in an
alternate assessment. If the student is not participating in an alternate assessment, simply check, N/A.
In the space provided, outline the specific number of session(s), length of the session(s) and the location of
where the specially designed instruction will occur. Examples of location are, but not limited to, the general
education classroom, special education classroom, therapy room, total school environment, etc.
LRE will be determined by the amount of time a student is removed from non-disabled peers. In the example of
total school environment, a student may or may not be served with non-disabled peers; time with just nondisabled peers MUST be calculated when determining LRE.
IEP DEC 4 (7 of 10)
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
Duration of Special Education and Related Services: From:
/
/
To:
Student:
/
/
DOB:
School:
/
/
Grade:
III. District-Wide Assessment Program
In the space provided, list the district-wide assessments, if any, and any accommodations or alternate
assessments
to be used by the student.
DISTRICT-WIDE
ASSESSMENT(S)
ALTERNATE
ASSESSMENT(S)
IMPLEMENTATION
SPECIFICATIONS
ACCOMMODATION(S) OR
IV. Alternate Assessment Justification
If the student is participating in any alternate assessment(s), explain why the regular testing program, with or without
accommodations, is not appropriate and why the selected assessment is appropriate:
N/A
V. Specially Designed Instruction, Related Services, and Nonacademic Services and Activities
A. Anticipated Frequency and Location of Specially Designed Instruction
Special Education:
Sessions Per:
Week
Month
Reporting
Period
1st Semester
2nd Semester
1st Semester
2nd Semester
1st Semester
2nd Semester
Session Length:
Year
Location:
IEP (DEC 4 pg. 8) Directions
Related services are those services the IEP team identifies that are required to assist the student to benefit from
special education
A related service support description can be used when the student and/or staff needs support from a related
services provider rather than direct intervention services for the student. No annual goal(s) are required for a
related service support description, although, a related service support description can coexist with annual
goal(s) for related services.
Related service support description does not require a session length.
Non-academic services and activities in which the student is removed from participation with non-disabled
peers must be factored into the educational placement of the student.
Examples of non-academic services and activities are, but not limited to lunch, recess, assemblies, media center,
field trips, etc.
LRE is not determined by location, but time removed from non-disabled peers.
The instructional day is defined as the time between bell to bell, and therefore, can vary form school to school
within an LEA.
Educational placement must be calculated based on the total minutes of the instructional day.
IEP DEC 4 (8 of 10)
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
Duration of Special Education and Related Services: From:
/
/
To:
/
/
Student:
DOB:
School:
/
/
Grade:
B. Anticipated Frequency and Location of Related Services
The IEP Team determined related services are not required to assist the student to benefit from special education.
The IEP Team determined the following related services are required to assist the student to benefit from special education.
Related Service(s):
Sessions Per:
Week Month
Reporting
Period
Year
Session Length:
Location:
Support Description
Support Description
Support Description
Transportation is required as related service. Describe special transportation services:
C. Nonacademic Services & Activities (Refer to Section I: General Education Program Participation)
List the nonacademic services and activities in which the student will not participate with nondisabled peers.
This time must be factored into the determination of continuum of alternative educational placement below.
Nonacademic Services & Activities:
Sessions Per:
Week Month
Year
Reporting
Period
Session Length:
VI. Continuum of Alternative Educational Placements
Indicate educational placement by checking only one box below:
(Educational placement is determined by calculating the amount of time the student is removed from nondisabled peers.)
School Age:
Regular - 80% or more of the day with nondisabled peers
Resource - 40% - 79% of the day with nondisabled peers
Separate - 39% or less of the day with nondisabled peers
Separate School
Residential
Home/Hospital
Preschool:
Regular Early Childhood Program 80% of time
Regular Early Childhood Program 40%-79% of time
Regular Early Childhood Program less than 40% of time
Separate Class
Separate School
Residential Facility
Service Provider
Home
IEP (DEC 4 pg. 9) Directions
The LRE justification statement must be addressed for every student.
Completion of this section is only required if the LEA’s schedule for progress monitoring is different than at
issuance of report cards.
ESY must be addressed for every student.
IEP DEC 4 (9 of 10)
INDIVIDUALIZED EDUCATION PROGRAM (IEP)
Duration of Special Education and Related Services: From:
/
/
Student:
To:
/
/
DOB:
School:
/
/
Grade:
VII. Least Restrictive Environment Justification Statement
If the student will be removed from nondisabled peers for any part of the day (general education classroom,
nonacademic services and activities), explain why the services cannot be delivered with nondisabled peers with
the use of supplemental aids and services.
N/A Student will not be removed from nondisabled peers.
VIII. Progress toward annual goals will be reported with the issuance of report cards unless otherwise
specified below:
IX. Extended School Year Status (ESY worksheet available at www.ncpublicschools.org/ec/policy/forms.)
Is not eligible for extended school year
Is eligible for extended school year
Eligibility is under consideration and will be determined by
/
/
X. Record of IEP Team Participation (Note with an * any team member who used alternative means to participate.)
A. IEP Team. The following were present and participated in the development and writing of the IEP.
Name
Copy given/sent to parent(s): by
Position
LEA Representative
on
/
Date
/
/
General Education Teacher
/
/
Special Education Teacher
/
/
Parent
/
/
Student
/
/
/
/
/
/
/
/
/
/
/
.
IEP (DEC 4 pg. 10) Directions
This form is used when holding an addendum IEP meeting.
If, at the conclusion of a manifestation determination, it was determined the behavior in question was not a
manifestation resulting in a change in educational placement (continuum) for the student, it should be noted by
checking “yes” where it asks if the IEP was amended due to a disciplinary change in placement.
IDEA allows for the amendment of an IEP without holding a meeting. However, Moore County is requiring
that an IEP meeting be held if an addendum to the IEP is made.
It is important to document the details of the amendment on this form!
IEP DEC 4 (page 10 of 10)
INDIVIDUALIZED EDUCATION PROGRAM (IEP) ADDENDUM
Duration of Special Education and Related Services: From:
/
/
To:
/
/
Student:
DOB:
School:
/
/
Grade:
X. Record of IEP Team Participation continued
(Note with an * any team member who used alternative means to participate.)
B. Reevaluation. The IEP was reviewed at reevaluation and was found to be appropriate. An annual review of
this IEP will be conducted on or before
Name
/
/
.
Position
LEA Representative
General Education Teacher
Special Education Teacher
Parent
Student
Date
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
XI. Amending the IEP
The IEP was amended due to a disciplinary change in placement.
yes
no
A. IEP Addendum Team.
The following were present and participated in the development and writing of the addendum to the IEP.
Name
Position
LEA Representative
General Education Teacher
Special Education Teacher
Parent
Student
Date
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
/
B. Amending the IEP without holding a meeting after the annual IEP Team meeting for the school year.
The parent and LEA agreed that the IEP could be amended by
on / /
without holding a
meeting.
Copies of the amendment were provided to individuals responsible for implementing changes to the IEP by
on / /
Indicate page(s) and section(s) where any amendment(s) were made:
A revised copy of the IEP with amendments incorporated was provided to parent(s) on
/
/
by
.
Secondary Transition Component (DEC 4a pg. 1) Directions
Students with disabilities, age 14 and older, are required to have a transition component to their IEP.
Sections A, B, and C of the component are required for students who are 14 and 15 years old. All sections of
the component are required for students 16 years and older.
IDEA requires students be informed that rights will transfer to them at age 18. This notice must be given at age
17. Checking “yes” to the question on this form will meet this requirement. Check N/A if the statement does
not apply.
Section “A” provides information and documentation regarding who provided information how it was collected.
IEP teams are instructed to provide details, as requested.
IDEA requires that students with disabilities have a measurable post-secondary goal in the areas of
education/training and employment. The only optional post-secondary goal is independent living. The IEP
team will determine if a goal to support independent living is appropriate.
Post-secondary goals must be written for what the student will do after high school and should not reflect
his/her current/activities.
Annual goals, based on the student’s present level of performance should clearly be linked to his/her postsecondary goals. What skills will the student need in order to accomplish his/her post-secondary goals?
Section “C” is required for all students age 14 and up. Check one of the options listed.
If possible, the four-year plan for the student who is in high school should be examined and attached.
Secondary Transition DEC 4a (1 of 2)
SECONDARY TRANSITION COMPONENT
Duration of Special Education and Related Services: From:
/
/
Student:
/
To:
DOB:
School:
Has the student been informed of his/her rights, if age 17 and older?
/
/
/
Grade:
Yes
N/A
Section A - Student Needs, Strengths, Preferences and Interests (Beginning at age 14 and updated annually)
The following people gave information about the student’s needs, strengths, preferences and interests and course of study
selection:
Student
Parent(s), Guardian(s) and Family Members
Adult Service Agency Representatives (specify):
School Staff
Other (Explain):
Indicate which age appropriate transition assessments were conducted for the development of measurable postsecondary goals
and transition activities and the date they were conducted:
INFORMAL ASSESSMENT(S):
Interest and Skill Inventories
Observations/Situational Assessments
Rating Scales
Interviews
Other (Explain):
FORMAL ASSESSMENT(S):
Other (Explain):
Section B – Course of Study (Beginning at age 14 and updated annually)
The student is following a course of study that leads to the high school diploma:
Future Ready Core Course of Study (effective with the 9 th grade class of 2009/2010)
College/University Prep Course of Study*
College Tech Prep Course of Study*
Career Preparation Course of Study*
Occupational Course of Study
(*Not applicable to students entering 9th grade beginning with the freshman class of 2009-2010.)
The student is following extensions of the standard course of study and pursuing the graduation certificate
The student is in middle school and is following the North Carolina Standard Course of Study
North Carolina Standard Course of Study
.
; or the extensions of the
Section C – Postsecondary Goals (Beginning at age 16 and updated annually)
Indicate the student’s measurable post-secondary goals in each of the following areas on an annual basis:
Education/Training:
Employment:
Independent Living (if appropriate):
.
Secondary Transition Component (DEC 4a pg. 2) Directions
This section is required for students who are 16 and older and can reflect activities that span multiple years.
Transition activities should be written to support the student’s post-secondary goals and should answer the
question, what things are necessary for the student to achieve his/her goal(s)? The transition services/activities
are the specific steps/strategies that focus on improving the academic/functional achievement of the child to
facilitate his/her movement from school to post-school.
Transition activities may or may not be required for each transition area; however, teams are required to discuss
each area and indicate in the space provided that an activity is not required.
It is important to remember that responsibilities for the activities can be assigned to individuals outside of the
school (parents, student, outside agencies.)
If an outside agency(s) is assigned responsibility for a transition activity, a representative(s) of the agency(s)
must be invited to the IEP meeting. Parent(s) or student(s) who are 18 years old and older, must consent to the
involvement of the outside agency. Documentation of this consent is located on the “Invitation to Conference”
form.
Secondary Transition DEC 4a (1 of 2)
SECONDARY TRANSITION COMPONENT
Duration of Special Education and Related Services: From:
/
/
To:
/
/
Student:
Section D – Transition Services (By age 16 and updated annually)
Transition
Areas
Instruction
Transition Activities
Responsible
Person and/or Agency
Anticipated
Completion
Date
/
/
Related Services
/
/
Community
Experiences
/
/
Employment
/
/
Adult Living
Skills
/
/
Daily Living
Skills
(if appropriate)
Functional
Vocational
Evaluation
(if appropriate)
/
/
/
/
Additional Transition Meeting Directions per Moore County
Transition Training
Judy Clendenin, Transition Facilitator
Moore County Schools, (updated October, 2009)
Definition of Transition Services—
The term “transition services” means a coordinated set of activities for a child with a
disability that:
Is designed to be within a results-oriented process, that is focused on improving the
academic and functional achievement of the child with a disability to facilitate the child’s
movement from school to post-school activities, including postsecondary education,
vocational education, integrated employment (including supported employment);
continuing and adult education, adult services, independent living, or community
participation;
Is based on the individual child’s needs, taking into account the child’s strengths,
preferences, and interests; and
Includes instruction, related services, community experiences, the development of
employment and other post-school adult living objectives, and, if appropriate, acquisition
of daily living skills and functional vocational evaluation.
IDEA, 2004, Secondary Transition; U.S. Department of Education, Office of Special
Education Programs 02-01-2007
Transition Planning is Simple . . .
Post-School Goals—Where is the student going?
Transition Activities and IEP Goals/Objectives—How is the student going to
get there?
Responsible Persons and Timelines—Who is going to help the student and
when are things going to be done?
Transition Planning is Life Planning . . .
At age 14, in NC, Transition Begins and Comes First. It should
drive the IEP.
Complete the transition plan first before determining
annual goals, etc.
Review transition plan first at IEP meeting to show focus of
meeting.
Purpose of Transition Planning:
To help students and their families think about life after high school and identify long-range goals for the future
To design the high school experience to ensure that students gain the skills and
connections needed to achieve post-school goals
To provide opportunities for joint planning with future service providers
To increase the chances of post-school success
DEC 4 (2a) - Transition—General Rules to Follow:
Page 1 is completed at age 14, or if age 13 and turning 14 during school year
and done annually after that.
Student must be invited to IEP meeting.
Post-secondary goals mean occurring after the student graduates from high
school.
Page 2 (Section D—Transition Activities), is completed at age 16 or if 15
and turning 16 during school year and done annually after that.
Transition Activities, p. 2--occur while the student is in high school and will
help them reach their post-secondary goals.
Indicator 13
Percent of youth aged 16 and above with an IEP that includes coordinated,
measurable, annual IEP goals and transition services that will reasonably enable
the child to meet the postsecondary goals. [20 U.S.C.1416 (a) (3) (B)]
Good websites for Indicator 13 and other transition information:
www.nsttac.org and www.ncdcdt.org
NSTTAC Indicator 13 Checklist
1. Is there an appropriate measurable postsecondary goal or goals that covers
education or training, employment, and, as needed, independent living?
2. Is (are) there the postsecondary goal(s) updated annually?
3. Is there evidence that the measurable postsecondary goal(s) were based on ageappropriate transition assessment(s)?
4. Are there transition services in the IEP that will reasonably enable the student to
meet his or her postsecondary goal(s)?
5. Do the transition services include courses of study that will reasonably enable
the student to meet his or her post-secondary goal(s)?
6. Is (are) there annual IEP goal(s) that will reasonably enable the child to meet
his/her postsecondary goal(s)?
7. Is there evidence that the student was invited to the IEP team meeting where
transition services were discussed?
8. If appropriate, is there evidence that a representative of any participating
agency was invited to the IEP team meeting with the prior consent of the parent
or student who has reached the age of majority?
Does the IEP meet the requirements of Indicator 13? (Circle one)
--Yes (all Ys or NAs are circled)
--No (one or more Ns circled)
Item #1: Is there an appropriate measurable postsecondary goal or goals
that cover(s) education or training, employment, and, as needed, independent
living?
(Section C, p. 1, DEC 4 (2a) Transition)
All goals must be:
Measurable = Countable, Example: “After graduation, Nellie will . . .”
An outcome, not a process
Written in complete sentence form
Based on students’ preferences, interests, needs and strengths
Based on transition assessments
Written for post-secondary education or training, employment, and, if
appropriate, independent living.
May change from year to year
May initially be less specific, increasing in detail as student approaches
graduation
Should reflect high but realistic expectations
Examples of Post-Secondary Goals --Education/Training
After graduation, Nellie will attend the community college in order to obtain CNA
certification.
After graduation, Nellie will receive on-the-job training through adult services of
the Workforce Investment Act (WIA) Program in a clerical assistant position.
After graduation, Nellie will complete a 4-year degree in social work from a
university.
After graduation, Nellie will attend the compensatory education program at the
community college.
After graduation, Nellie will participate in habilitative training related to
individualized needs in the areas of adult living skills and communication.
(Community College): After graduation, Caleb will obtain an A.A. degree in
Early Childhood Education at community college.
(Compensatory Education): After graduation, Jack will attend the compensatory
education program at the community college 2 times a week.
(WIA OJT): After graduation, Keila will participate in a WIA sponsored on-thejob training program as an office assistant.
(Continuing Education courses): After graduation, Rose will complete continuing
education courses in floral arrangement, computer skills, and financial management.
(Employability training at a community-rehab. program (CRP): After graduation,
Danny will be enrolled in the fork-lift operator training program of a communityrehab. program.
(Web-based education program): Haley will complete an on-line degree in
marketing from an accredited web-based college program after graduation.
(Employment-based training program): After graduation, through his employment
at a home improvement center, Harold will participate in and successfully complete
the manager trainee program.
(Habilitative training): After graduation, Dustin will receive daily habilitation and
community access training through state or Medicaid sponsored developmental
disabilities services.
(Volunteerism): After graduation, Delores will participate in productive activities
(volunteer work) at community non-profit agency(s) with one-on-one assistance.
Employment - Examples of Post-Secondary Goals (from general to more specific
as student becomes older).
(Freshman): After graduation, Sarah will work full-time in a job where she can
help others.
(Sophomore): After graduation, Sarah will work full-time at a local
agency/business in an area related to human services.
(Junior): After graduation, Sarah will work full-time at a local agency/business in
an area related to young children or the elderly.
(Senior): Immediately after graduation, Sarah will work as a full-time childcare
assistant’s helper at a local daycare.
(Full-time competitive): Kelsey will obtain a full-time job in the field of
Information Technology after completion of a 4-year degree.
(Part-time competitive): After graduation, Patty will work part-time as a
cashier/stocker at a local retail business using supported employment job coaching.
(Mobile work crew): Immediately after graduation, Freddie will work part-time in
a supported employment mobile work crew in the area of custodial cleaning.
(Community Rehab. Program) CRP: During the summer following graduation,
Jamal will begin production-based employment at the local community rehabilitation
program.
After graduation, Nellie will participate in productive activities with the assistance
of a CAP- MR/DD worker.
After graduation, Nellie will work full-time as a childcare assistant at a daycare.
Independent Living - Examples of Post-Secondary Goals
Following graduation, Nellie will live at home & participate in as many daily living &
home living activities as possible.
After graduation, Nellie will live in an apartment with a roommate.
Following graduation, Nellie will live in a Developmentally Disabled Adult group home.
After graduation, Nellie will live at home while attending college and will move into an
independent living arrangement sometime after completing her college degree.
After graduation, Nellie will live in a rented trailer with her husband.
Following graduation, Grace will live at home and perform personal hygiene and clothing
care tasks, contribute financially to household expenses, and prepare simple meals.
Immediately after graduation, Miranda will live at home with her parents while preparing
to move into an apartment with a roommate.
After graduation, Tim will live at home until a placement in a Developmentally Disabled
Adult (DDA) group home is made.
After graduation, Tommy will live at home while attending college and move into an
independent living situation after obtaining a college degree.
After graduation, Caroline will continue to participate in sports activities offered by the
recreation department and be an active member of her church, maintain her hobby of collecting
Disney memorabilia and play computer games.
After graduation, Sam will oversee his medical care including making appointments,
maintaining records, monitoring/administering medication, and making financial arrangements
for medical bills.
Don will access public transportation to and from work each day beginning his first day
of employment.
Item #2: Is (are) the postsecondary goals(s) updated annually? Are they
updated in conjunction with the development of the current IEP.
Item #3: Age-Appropriate Transition Assessment-- Is there evidence that the
measurable postsecondary goal(s) were based on age-appropriate transition
assessment(s)?
DEC 4, Page 1--
SECTION A – Student Needs, Strengths, Preferences & Interests—
Give interest inventory(s), interviews, informal assessments of your choice that are
age-appropriate such as:
(Choose from assortment I have given you.) Examples: Student Dream Sheet,
Parent/Student Questionnaire, Career Interest Survey, Piney Mountain Learning Styles
and Interest Inventory or any that you have from workbooks, internet, etc., to one or more
of the following to assess students, preferences, interests, needs and strengths:
_____Student
_____Parent(s) and Family Members
_____Adult Service Agency Representatives
_____School Staff
_____Other (Explain): ________________________________
Indicate how age-appropriate transition assessments were conducted for the
development of measurable post-secondary goals and transition activities. Write in
the title of assessment(s) given and date given.
_____Interest and Skill Inventories (Example: Piney Mountain Career Interest Assessment, 9/9/07)
_____Observations/Situational Assessments
_____Formal and Informal Assessments (Example: Student Dream Sheet, 9/7/07)
_____Rating Scales
_____Interviews
_____Other (Explain):______________________________________________
For each postsecondary goal, is there at least one of the following listed?
1. Instruction
2. Related Service(s)
3. Community Experience(s)
4. Employment—(means development of employment and post-school objectives)
5. Adult Living Skills
6. Acquisition of Daily Living Skills (if appropriate)
7. Functional Vocational Evaluation (if appropriate)
Item #4: Are there transition services in the IEP that will reasonably
enable the student to meet his/her postsecondary goal(s)?
DEC 4 (2a) page 2 of 2, Section D Transition Activities (by age 16 and updated
annually)
All Transition Activities . . .
Occur while the student is in high school
Outline the steps toward achieving post-school goals
Are dynamic and observable—such as: provide, meet with, visit,
organize, create, examine, work towards, conduct, observe,
complete, explore, develop, participate in, obtain, identify, enroll
in, expand, extend, study, receive…
Developed to support each post-school goal
Can occur on the school campus, at home, or in the community
“Responsible person and/or agency” should be a wide range of people
(Do not name names.)
Can be one-time events or ongoing activities
Can be services delivered to the student or activities in which the
student is involved or a combination of both
Form the link between the post-school goals and the IEP
Please see examples of transition activities on the following pages for each
of the seven areas + extra handout entitled: “Transition Activities”.
1. Instructional Activities--Instruction the student needs to receive in specific areas to
complete needed courses, succeed in the general curriculum and gain needed life skills.
(Storms, O’Leary and Williams, 2000)
Ideas for Instructional Activities:
Tutoring and remediation activities
Following a course of study
Participation in general education elective courses and/or CTE pathway
Arranging for classroom accommodations and modifications
Social skill training relevant to work, college, or the community
Preparation for college admission tests
Study/test-taking skills training
College/university campus tours
Referral to Vocational Rehabilitation (VR) for financial assistance for postsecondary education/training
Assistance with college applications/financial aid forms
Driver’s education
Instruction in financial management skills, using transportation services or
any other community access skill set
Examples of Statements for Instructional Activities:
Take curriculum assistance class for help in (math, reading, writing).
Take SAT prep class.
Stay after school for ______________ tutoring ____ days a week.
Meet with VR counselor.
Complete a career technical education class in the area of ____________.
Enroll in Driver’s Education & obtain license.
2. Related Services Activities--include supportive services that assist in benefiting from
transition services delivered through special education and the projected related services needed
to transition from school to adult life.
Ideas for Related Services Activities:
Physical Therapy
Speech Therapy
Occupational Therapy
Transportation
Mobility and Orientation Training
Rehabilitation Counseling
Assistive Technology
Medication Monitoring
Rehabilitation Engineering
Mental Health Counseling
Behavior Management Support
Examples of Statements for Related Services Activities:
Arrange for reliable transportation to college/work.
Determine who will repair wheel chair.
Determine who will replace batteries for hearing aid.
Determine who will monitor medication.
Meet with guidance counselor to review course of study and classes.
3. Community Experience Activities--are services occurring in the community
delivered by the school or other agencies that provide students with the opportunity to practice
skills in the actual settings in which they will be used. Community experiences also involve
participating in the community through the use of local businesses, recreational services,
volunteer work, leisure activities, etc.
Ideas for Community Experience Activities:
Community-based training in any area/domain
Attending a concert
Visiting a museum, art gallery or community exhibit
Joining an aerobics class, taking a line dancing class, or swimming at the YMCA
Using public transportation or arranging for a ride
Going to the beauty shop
Renting a video or going to the movies
Attending church or participating in a church choir
Volunteer work (examples: humane society, hospital)
Using the public library, bank, or post office
Examples of Statements for Community Experience Activities:
Attend exercise classes at the Recreation Department.
Play on a basketball, baseball team through Parks & Recreation.
Take guitar lessons, dance lessons, etc..
Participate in the church choir.
Volunteer at a local hospital or nursing home.
Become an assistant coach for little league sports.
4. Employment Activities—are employment-related experiences provided by the school or
other agencies that provide the training and education needed for a future job or career.
Ideas for Employment Activities (School-Based)
Instruction in job-seeking skills
Completion and presentation of career portfolio
Career counseling
Web-based career awareness activities
Participating in job clubs
Attending job fairs
Participation in school-based enterprises and small businesses
Vocational training through an on-campus job
Mock interviews with business leaders
Participation in on-site vocational training at a community rehabilitation
program
Ideas for Employment Activities (Work-Based)
Job shadowing at local retail stores
Participation in enclaves or mobile work crews
WIA or CTE internships
Part-time or full-time paid employment
Volunteerism or community service work
Industry tours
Situational assessment
Work Adjustment—Job Coaching
Referral to Vocational Rehabilitation (VR) for supported employment
Obtaining applications and/or interviewing for job
Registering at the Job Link Center
Examples of Statements for Employment Activities:
Attend job fair.
Complete the Construction Technologies (CTE) pathway.
Tour retail stores & obtain information about job opportunities.
Continue to work at __________ (List current job student has.)
Visit local Employment Security Commission Office.
5. Adult Living Skills—are those skills used on an as-needed basis in order to function as
independently as possible as an adult.
Ideas for Adult Living Activities:
Setting up a checking or savings account
Registering to vote and/or voting
Instruction in obtaining and maintaining a car
Getting a driver’s license
Investigating residential options
Touring apartment complexes and meeting with apartment managers
Learning options for obtaining large household items (examples: furniture,
appliances)
Instruction in various tax requirements
Instruction in setting up accounts for utilities
Caring for a pet
Examples of Statements for Adult Living Activities:
Open & learn how to use a checking account.
Register to vote.
Plan a budget and pay bills.
Complete income tax form.
Learn how to maintain your car.
Investigate residential options.
Learn self-advocacy skills.
6. Daily Living Skills (if appropriate)—Daily living skills involve activities that are
required for day-to-day functioning within the home and the community. These activities consist
of things that are done routinely by self-sufficient adults. Daily living skills can also include any
activity that encourages increased independence.
Ideas for Daily Living Activities:
Cooking
Cleaning tasks
Clothing care
Personal care or assisting with personal care (such as bathing, dressing)
Paying routine bills
Shopping for food or health care products
Hair care or nail care
Simple home maintenance (such as replacing light bulb or hanging picture)
Handling a medical emergency
Self-medication or monitoring routine health procedures (such as asthma,
diabetes)
Examples of Statements for Daily Living Activities:
Clean the house.
Shop for & prepare meals.
Learn the importance of hygiene.
Enroll and complete a Foods & Nutrition Class.
7. Functional Vocational Evaluation (if appropriate)—is the assessment of a
student’s interest, aptitudes, and vocational skills. Assessment information can be obtained
through a variety of formal and informal procedures including traditional psychometric tests,
situational assessments, and observations. Vocational assessment can be performed by the
school or outside agencies. Information obtained through vocational evaluation should be used
in a functional manner to assist with the transition planning process.
Ideas for Functional Vocational Evaluation Activities:
Standardized/formal assessments (if results are used in a functional manner)
Interviews, surveys, or questionnaires
Work samples
Portfolio assessment
Situational assessment
Environmental, Method, and Task Analysis
Examples of Functional Vocational Evaluation Activities:
Attend VR conferences for testing & assessment.
Complete work portfolio.
Write a resume.
Practice job interviews.
Item #5: Courses of Study Aligned with Postsecondary Goal(s): Do the
transition services include courses of study that will reasonably enable the student to
meet his or her postsecondary goal(s)?
A multi-year description of coursework to achieve the student’s desired post-school goals,
from the student’s current to anticipated exit year. (From: Storms, O’Leary &
Williams[200]
Page 1, SECTION C--Course of Study--Check only one item in this section.
When the student is in the 8th grade, the Course of Study leading to the high
school diploma should be determined.
If student will be receiving the graduation certificate, check that line only.
If student is 14 years old and in 6 th or 7th grade, check only the option that
says “The student is in middle school and is following the NC Standard Course of
Study” or “the extensions of the NC Standard COS” option (since the student will
remain in middle school).
Item #6: Is (are) there annual IEP goal(s) related to the student’s transition
services needs?
Annual IEP Goals(s) Is (are) there annual IEP goal(s) that will reasonably enable
the child to meet the postsecondary goal(s)?
There must annual goal(s) included in the IEP that will help the student
make progress towards the stated postsecondary goal(s).
Examples of annual goals directed toward post-secondary goals.
Given community college information, John will demonstrate knowledge of
the college’s admission requirements by describing these requirements and
identifying admission deadlines with 90% accuracy by November, 2006.
Given a bus schedule adapted with pictures, Stephanie will select the correct time
and stop for five scenarios of activities presented to her with 80% accuracy.
In order to be successful at a four-year college, Hal will write using
conventional grammar, usage, sentence structure, punctuation, capitalization, and
spelling with 80% accuracy based on the district grade level rubric.
In order to be successful in on-the-job training, Frankie will practice selfadvocacy skills by discussing his disability, learning characteristics and needed
accommodations and modifications with all his general education teachers, without
prompting based on teacher report.
In order to gain entry into and successfully complete a training program in
welding, Kyle will improve his reading comprehension skills to an 8.0 grade level.
In order to succeed in a community-based employment program, Susan will
complete two-step picture directions using a picture chart 95% of the time.
In order to independently communicate information about himself while in
the community, Juan will write his first and last name and phone number with 100%
accuracy.
Item #7: Is there evidence that the student was invited to the IEP Team
meeting where transition services were discussed?
(In the IEP folder, is there evidence that the student was invited to the IEP meeting?)
Item #8: If appropriate, is there evidence that a representative of any
participating agency was invited to the IEP Team meeting with the prior
consent of the parent or student who has reached the age of majority?
Are there transition services listed on the IEP that are likely to be provided
or paid for by an outside agency such as:
Agency(ies) identified that would provide or pay for postsecondary
services
Evidence of parent consent (student when age of majority) to invite
agency(ies)
Evidence that agency(ies) were invited to the IEP meeting
Examples of Coordination:
Letter of consent to invite outside agency signed by parent, then invitation to
invite outside agency such as VR or other agency, community college
disability services office, etc.
Finally . . . Steps in the Transition Planning Process
Step 1: Facilitate student, family and adult service provider involvement
Step 2: Identify post-school goals based on age-appropriate transition
assessments
Step 3: Determine present level of performance as it relates to post-school
goals
Step 4: Determine a course of study
Step 5: Determine transition activities
Step 6: Determine responsible persons and timelines for transition activities
and services
Step 7: Determine IEP goals/objectives linked to the post-school goals
Related Services Support Description (DEC 4b) Directions
These support services are a part of an Individualized Education Program (IEP). The description will be written
by an IEP team that includes the related service provider and attached to the IEP.
The purpose of the service is to support the student’s access and participation in his/her special education
program.
The related service provider’s service (intervention) notes documenting these services are available on request.
The student needs support from a related service provider rather than skills-based services in order to acquire
specific skills. Therefore, these services do not require specific IEP goals, benchmarks or progress reports.
The service frequency will be documented on the IEP service delivery page (DEC 4) specifying how often the
related service provider will monitor, although emergencies or unforeseen incidents may require additional
visits.
The description will specify what the student needs from the related service provider in order to access his/her
educational environment and participate in his/her special education program.
This description of services must be signed and dated by the related service provider. The IEP team, which
includes the related service provider, must review it at least annually. It can be modified based on the student’s
needs.
Related service provider visits and time spent on behalf of the student will be documented and the record
maintained in the therapist’s file.
DEC 4b (1 of 2)
OT/PT/SLP RELATED SERVICES SUPPORT DESCRIPTION
Duration of Special Education and Related Services: From:
Student:
/
To:
DOB:
School:
/
/
/
/
Grade:
Date approved by IEP team and included/attached to IEP:
Service (Check all that apply):
/
OT
/
/
PT
SLP
Description of student needs (Explanation of why support is needed):
Classroom interventions delegated to classroom staff with related service provider support/training for teachers and staff:
(Program description, logs attached)
Active/Passive Range of Motion to Upper/Lower Extremities
Positioning program (e.g., in wheelchair, stander or other equipment)
Walking program with/without assistive device
Assistive technology/augmentative communication, and adapting switches and toys:
Check equipment
Feeding program
Sensory processing modifications
Transfers
Provide staff development/modeling techniques
Other:
Related service provider support:
Instruction for delegated activities, use of equipment
Observation of students in classroom settings
Monitor programs, specifically:
Connect IEP goals with NC Standard Course of Study
Adaptation (including assignments and assessments), accommodations, integration of skills or consultation for participation in
and/or with class
Assist in statewide (e.g., EOG, EOC, etc.) and/or district-wide assessments
Analyze and engineer environments, increasing opportunities for communication
DEC 4b (2 of 2)
Student:
DOB:
/
Related service provider support: (continued)
Programming assistive technology/augmentative communication, and adapting switches and toys:
Check in with bus staff
Equipment maintenance
Prepare classroom materials including home practice/carry over material(s)
Collaborate with other service delivery providers
Communicate and coordinate with outside agencies
Facilitate transitions to job/vocational settings and problem solve issues that arise
Evacuation planning support/consultation
Other:
Equipment Needed: (p=personal; c=classroom)
Switches/toys:
Splints or braces:
Computer adaptation:
Positioning devices, specifically:
Toileting aids, devices or equipment:
Mat/mat table
Walker or ambulation aid:
Stander:
Wheelchair
Wheelchair tray
Feeding equipment
Sensory Processing Tools:
Other:
Additional Comment(s) or Explanation(s):
(Therapist Signature)
_____/_____/_____
(Date)
/
Prior Written Notice (DEC 5 pg. 1) Directions
Check all the purposes that apply.
Complete all the requested student information. Use the student’s full name.
Under eligibility the first statement only applies at the time of initial referral, if the IEP team decides not to
evaluate the student.
Indicate which area of disability is the primary and which, if any, is the secondary area(s) of disability. The
primary area of disability is the one indicated for the purpose of Child Count.
Prior Written Notice DEC 5 (1 of 3)
PRIOR WRITTEN NOTICE
Decisions of the Local Education Agency (LEA)
Check Purpose:
Eligibility
Educational Placement/Change in Placement
Reevaluation
Disciplinary Change in Placement
Other:
Student:
DOB:
School:
/
/
Grade:
Dear
:
State and federal laws regarding students with disabilities require that the Local Education Agency (LEA) notify and
inform you if certain changes are being made to your child’s educational program. You must be informed when the
school district:
begins or refuses to begin the process of identification, evaluation, or educational placement of your child or the
provision of a free appropriate public education to your child;
proposes to change the identification, evaluation, or educational placement of your child; or
refuses to change your child’s free appropriate public education which usually means the IEP.
The IEP Team or other group of appropriate individuals determined that
ELIGIBILITY
Will not be evaluated.
Is not eligible for special education and related services.
Is eligible for special education in the category or categories of
.
Will receive the following related services in order to benefit from special education:
REEVALUATION
Continues to meet eligibility criteria for special education as
Eligibility category is being changed from
to
.
.
.
Will continue to receive the following related services in order to benefit from special education:
.
Will begin receiving the following related service(s) in order to benefit from special education:
.
Is no longer in need of the following related services in order to benefit from special education:
.
Prior Written Notice (DEC 5 pg. 2) Directions
EDUCATIONAL PLACEMENT (Least Restrictive Environment) REFERS TO CONTINUUM OF SERVICES
WITHIN THIS SECTION.
A Summary of Performance is required for the first two options dealing with graduating or reaching maximum
age of entitlement.
Parents must be provided Prior Written Notice at the completion of each manifestation determination explaining
the decision made by the team.
Address the decision(s) made in the current IEP team meeting. Explain why the decision(s) were made.
Teams are instructed to be specific as to the options considered/rejected and why.
For statement III, include the types of tests administered (cognitive, educational, adaptive behavior, etc.),
observations, screenings, informal assessment, review of records, etc.
Prior Written Notice DEC 5 (2 of 3)
Student:
Grade:
School:
EDUCATIONAL PLACEMENT/CHANGE IN EDUCATIONAL PLACEMENT
Initial educational placement is
.
Educational placement is being changed from
to
.
No longer meets eligibility criteria and will be exited from the special education program.
Is graduating with an NC Diploma and will be exited from the special education program.
Has reached the maximum age of entitlement (22 years old) and will be exited from the special education program.
Has not graduated with an NC Diploma or reached the maximum age of entitlement (22 years old); however, is
exiting school with a graduation certificate. (Please be aware that students with disabilities are entitled to attend
school until reaching maximum age of entitlement (22 years old) or graduating with an NC Diploma. Eligible
students who return to school will continue to receive specially designed instruction through their entitlement
period.)
DISCIPLINARY CHANGE IN PLACEMENT
Conduct is a manifestation of
’s disability.
Conduct is not a manifestation of
’s disability.
CHANGES IS THE PROVISION OF FAPE/OTHER DECISION: (Provide Proposals or Refusals)
Proposals:
Refusals:
EXPLANATION OF ACTION(S) PROPOSED OR REFUSED: (Each action must be specifically addressed in I-II-IIIIV-V.)
I. The IEP Team or other group of appropriate individuals decided the action(s) stated above on pages 1-2 because:
II. The IEP Team or other group of appropriate people also considered the following option(s) including the continuum
of alternative education placements if applicable, and rejected these options because:
III. Describe each evaluation procedure, test, record or report, used as basis for the action stated above on pages 1-2:
IV. Describe other factors that are relevant to the agency’s proposal or refusal:
Prior Written Notice DEC 5 (3 of 3)
Student:
Grade:
School:
The following individuals were present during the development of this Prior Written Notice on
Name
/
/
:
Position
This is the final action (decision) of the local education agency. If you disagree, you, as the parent or adult
student, are entitled to the due process rights that are described in your Handbook on Parents’ Rights
(www.ncpublicschools.org/ec/policy/resources/rights). The deadline for filing a petition for a due process
hearing is one year (1 year) from receipt of this notice.
If you do not have a copy of the Handbook on Parents’ Rights or would like another one, please contact
your school principal or call the local director of Exceptional Children Programs. The principal or
director can also help you understand your rights if you have any questions, or you can call the
Exceptional Children’s Assistance Center, 1-800-962-6817. Please save this notice for your records.
If you have any questions, please feel free to call: Name:
This decision will be implemented on
/
/
Prior Written Notice was given to the parent by
Prior Written Notice was sent to the parent by
Method of delivery:
.
, Phone Number:
on
on
/
/
/
/
.
Student:________________________________School:________________Date::__________
page _____of______
IEP COMMITTEE MINUTES – DEC 5
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
(White – E.C. Folder, Pink – Parent; Yellow – E.C. Office)
Student:________________________________School:________________Date::__________
page _____of______
IEP COMMITTEE MINUTES
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
_____________________________________________________________________________________________
(White – E.C. Folder, Pink – Parent; Yellow – E.C. Office)
Prior Written Notice – Disciplinary Change in Placement (DEC 5a)
Directions
This form must be completed and delivered on the day a proposed disciplinary removal constitutes a
change in placement (greater than ten (10) consecutive days or a series of short-term removals
constituting a change in placement).
It is completed and sent by school personnel as determined by the LEA, along with a copy of the
Handbook on Parents’ Rights.
The meeting date scheduled on this form serves as the invitation to the manifestation meeting.
The LEA is not prohibited from sending a second notice for manifestation meeting; however, the
meeting must occur within 10 school days.
The contact person is determined by the LEA.
Prior Written Notice-Disciplinary Change in Placement-DEC 5(a)
PRIOR WRITTEN NOTICE
Decisions of the Local Education Agency (LEA)
Student:
DOB:
School:
/
/
Grade:
Dear
:
State and federal laws regarding students with disabilities require that the Local Education Agency (LEA) notify and inform you if
certain changes are being made to your child’s educational program. You must be informed when the school district proposes a
change to the educational placement of your child.
Today, school personnel determined that
(Student name) is subject to a disciplinary removal that will constitute a
change in placement. A meeting with you, the parent, and relevant members of the IEP Team will be held within 10 school
days to determine if the behavior in question is a manifestation of
’s disability. The team may also consider revising you
child’s IEP, based on the conclusion of the manifestation meeting.
The manifestation meeting is scheduled for:
/
/
EXPLANATION OF ACTION(S): (Items I-II must be addressed.)
I.
School personnel decided the action(s) stated above because:
II. Describe the reasons and length of the proposed removal:
It is expected that the following individual(s) will be present at the manifestation determination meeting:
Name
Position
Enclosed is a copy of the Handbook on Parents’ Rights. The principal or Director of Exceptional Children Programs can help
you understand your rights if you have any questions, or you can call the Exceptional Children’s Assistance Center, 1-800962-6817. Please save this notice for your records.
If you have any questions, please feel free to call: Name:
Prior Written Notice was given to the parent by
Prior Written Notice was sent to the parent by
Method of delivery:
.
, Phone Number:
on
/
/
on
/
/
.
Parent/Guardian Response:
Please respond to this notice by checking the appropriate option below and return one copy of this form as soon as possible.
I will attend the meeting as scheduled.
I will participate in the meeting by phone or other means. I can be reached at the following phone number on the
date/time mentioned above:
.
I cannot attend or participate in the meeting.
I have received a copy of the Handbook on Parents’ Rights.
Parent/Guardian Signature:
Copy: EC File
Date:
Special Education Services
Change in Placement Worksheet
Moore County Schools
CHANGE IN PLACEMENT WORKSHEET
FOR A SERIES OF SHORT-TERM SUSPENSIONS GREATER THAN 10 TOTAL DAYS PER YEAR
NAME ___________________________ NCWISE#: ______________ SCHOOL YEAR: ___________ TO ____________
SCHOOL: _______________________ Dates of This Proposed Short-Term Suspension : ___/____/___ TO ___/____/____
PREVIOUS SUSPENSIONS* (SEE
Begin
Date
To
End
Date
Days of
Suspension
BOTTOM)
Reason for Suspension
__
__
__
__
__
TOTAL DAYS SUSPENDED: ________
I. Change of Placement Determination:
1. Will the suspension result in removal for more than 10 cumulative days in the school year?
□ YES
2.
s
□ NO:
Title
If no, there is no change of placement.
If yes, was the student’s behavior in this incident substantially similar to the child’s behavior in the previous incidents
that have resulted in suspension this year?
□ YES
□ NO
If no, there is not a pattern resulting in a change of placement.
3.
If yes, based upon:
the length of each suspension,
the total of time the student has been suspended, and
the proximity of the suspensions to one another,
Will the proposed suspension result in a significant disruption in the child’s education services?
□ YES, there is a change of placement.
□ NO, there is not a change of placement.
II. School Manifestation Determination. If there is a change of placement, an IEP Team must convene to conduct a
MANIFESTATION DETERMINATION within 10 school days of the suspension, and a DEC 5a must be completed and sent
to the parent along with a Handbook on Parent’s Rights.
III. Education Service Plan. Whenever a special education student is removed from school for over 10 days in the school year,
educational services must be continued to allow the student to appropriately progress in his educational program and a behavioral
intervention plan developed as appropriate. Describe below the educational services that will be provided during the period of
suspension:_________________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
SIGNATURE
ADMINISTRATOR
__________________________________________________________________________________________
SIGNATURE
SPECIAL EDUCATION TEACHER
__________________________________________________________________________________________
SIGNATURE
REGULAR EDUCATION TEACHER
__________________________________________________________________________________________
SIGNATURE
POSTION
__________________________________________________________________________________________
*Include days of in-school suspension IF student did not receive services specified in the IEP, including access to the general curriculum. Also a bus
suspension must be counted as OSS if transportation is part of a student’s IEP and no alternative transportation is provided.
*Retain record in
the confidential folder.
Revised March 2009
Special Education services
MDR
Moore County Schools
MANIFESTATION DETERMINATION REVIEW
Name: ________________________NCWise#____________ Grade: ____School: ______________
DOB: ___/ ___/ ___
Area of Disability: ________________________
Date of Suspension: ___/___/___ Date of MDR: ___/___/___
Length of Suspension: _____________________
Total # of Days of Previous Suspensions: _____________________
I. BEHAVIOR THAT LED TO DISCIPLINARY ACTION
a.
Describe the behavior that led to this suspension. (Attach the Suspension Notice)
_________________________________________________________________________________
_________________________________________________________________________________
II. MANIFESTATION DETERMINATION
Relationship between the conduct in question and the child’s disability:
Date of most recent (re)evaluation (This is the date of the last eligibility meeting) ____ / ____ / ____
a.
Summarize the concerns noted during the most recent evaluation, including review of DEC3, psychological report,
and other evaluation records. ___________________________________________________________________
_______________________________________________________________________________
_______________________________________________________________________________
s
Title
_______________________________________________________________________________
b.
Summarize results of any FBA conducted on the student. _____________________________________________
_______________________________________________________________________________
c.
Summarize Individualized Education Program (IEP) goals [including BIP objectives]
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
d.
List any medical/health diagnosis and whether prescription medication is used.
_______________________________________________________________________________________________
e.
Has this or similar behaviors been exhibited in the past; If so, describe the pattern of behaviors.
_______________________________________________________________________________________________
_______________________________________________________________________________________________
f. List any additional information from parents or staff
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
Summary Question #1: Was the conduct in question caused by, or had direct and substantial relationship to, the
child’s disability?
□ YES
□ NO
(IF YES, PROCEED TO SECTION III)
Student Name:________________________ School: __________________Today’s Date: _________
RELATIONSHIP BETWEEN CONDUCT IN QUESTION AND THE FAILURE TO IMPLEMENT THE IEP:
a.
Individualized Education Program (IEP) date: _____________________ to ______________________
b.
Has a Behavior Intervention Plan been developed?
If so, has it been implemented?
c.
Was the Individualized Education Program, including modifications and supplementary services, being implemented?
□ Yes
□ Yes
□ Yes
□ No
□ No □ n/a
□ No
If NO, describe what part of the IEP was not implemented_________________________________________
___________________________________________________________________________________________
Summary Question #2: Was the conduct in question a direct result of the LEA’s failure to implement the IEP?
□ YES
□ NO
III.
MANIFESTATION STATEMENT: CHECK ONE
If the answer to EITHER of the summary questions is YES, then the behavior IS a manifestation of the student’s disability.
If the answer to BOTH of the summary questions is NO, then the behavior IS NOT a manifestation of the student’s
disability.
Was a manifestation of the student’s disability
Based on the information considered,
the IEP team determined that the misbehavior
Was not a manifestation of the student’s disability
If the incident WAS a manifestation, student may not be suspended. Required actions:
Develop new FBA/BIP or review/revise
existing BIP, as necessary, to address the
behavior.
Complete DEC5/Prior Written Notice
Student returns to the placement prior to suspension
UNLESS subject to 45-school day interim alternative
educational setting OR IEP team agrees to a change in
placement as part of a behavioral intervention.
If the incident WAS NOT a manifestation student may be suspended. Required actions:
IV.
NAME
Determine the services needed to enable the
student to participate in the general curriculum
and to progress towards IEP goals while on
suspension
Complete DEC5/Prior Written Notice
Address the IEP and/or develop a behavioral
intervention plan as appropriate
SIGNATURES
POSITION
LEA Representative
Special Education Teacher
Regular Education Teacher
Parent
DATE
Consent for Services (DEC 6) Directions
One initial “Consent for Services” is required to be in the confidential record of each student with a
disability.
Informed parental consent must be obtained before the initial provision of special education and related
services.
LEAs must document that parents or legal guardians have been given the Handbook on Parent’s Rights.
If the parent agrees for the student to receive the services proposed by the IEP team, they should check
“agree,” sign and date.
The LEA should ensure that the information indicated by each bullet below “I agree,” has been given
and explained to the parent.
If the parent(s) deny consent for the provision of services, they should check the box indicating “I do not
agree”. The LEA should ensure that the parent(s) understand the information in the paragraph and have
been given all indicated information. The parent(s) should sign and date.
Indicate if the copy was sent or given to the parent(s) by circling the choice. The name of the person
giving/sending the copy should be indicated along with the date the copy was given/sent
(month/day/year). If sent, the “return to” information should be provided giving the name and location
of the individual on the lines provided.
Consent for Services DEC 6
CONSENT FOR INITIAL PROVISION OF SPECIAL EDUCATION AND RELATED SERVICES
Dear
:
Re:
DOB:
/
/
The screenings and evaluations of your child have been completed. Your child is eligible for special education and related
services (if required to benefit from special education).
PARENTAL CONSENT
I agree for my child to receive special education and related services, if required to benefit from special education, and:
• Have received a copy of the evaluation report(s), summary of evaluation(s) and a copy of the Prior
Written Notice.
• Have received a copy of the Handbook on Parents’ Rights.
• Understand that I have had or will have an opportunity to participate in the development of the initial IEP
for my child.
• Understand that an IEP team, of which I am a member, will review and revise, as appropriate, the
educational program and educational placement of my child at least annually.
• Understand that an IEP team, of which I am a member, will conduct a reevaluation of my child at least
once every three years.
• Understand that providing my consent is voluntary and can be revoked at anytime. I understand that if I
revoke consent and the LEA has reason to believe my child continues to be eligible for special education
and related services, that the LEA can choose to utilize dispute resolution mechanisms such as the
facilitated IEP process, mediation, or due process in an attempt to resolve the dispute and to continue
providing special education and related services (if required to benefit from special education).
_____/_____/_____
(Date)
(Parent Signature(s))
I do not agree for my child to receive special education and related services. I have received a copy of the evaluation
report(s), summary of evaluation(s) and a copy of the Prior Written Notice. In addition I received a copy of the
Handbook on Parents’ Rights. I understand my child will not receive any services or protections provided by the
Individuals with Disabilities Education Act (IDEA) for students with disabilities.
_____/_____/_____
(Date)
(Parent Signature(s))
Copy given/sent to parent(s) by
on (date)
/
/
.
Reevaluation (DEC 7) Directions
The North Carolina Policies Governing Services for Children with Disabilities states that
“Reevaluation” is the process of examining existing data, and if determined necessary, gathering
additional data in order to:
determine continuing eligibility for special education;
assure that the continuing individual needs of a student are identified; and
assure appropriate educational programming (review and/or revision of IEP).
The reevaluation process must occur at least once every 3 years and may not occur more than
once a year, unless the parent and the LEA agree otherwise.
The reevaluation of children identified as Developmentally Delayed shall occur at least once
every 3 years following placement or prior to turning eight years of age, or prior to entering third
grade (whichever comes first).
Complete all information requested about the student: full name, date of birth, school, grade, and
disability category.
List the IEP Team members by name and position. Each should be dated to reflect the date of
participation.
The IEP team must document that existing data has been reviewed. Each of the following five
areas of information should be considered as the team reviews pertinent information:
review of all EC and cumulative records,
summary of previous evaluations/assessments,
parent provided information,
classroom information (assessments and observations),
information based on the observations of teachers and other service providers.
Additional pages/reports may be attached to the form to document the team’s findings.
To just indicate “yes” or “we discussed this area” is not sufficient. Include specific summary
statements of the discussion.
Based on the review of the existing data, the IEP team must decide if additional information is
needed and answer yes or no to the 4 questions at the bottom of the form indicated by A, B, and
C.
Reevaluation DEC 7
REEVALUATION
Student:
DOB:
School:
Grade:
The following members of the IEP Team participated in the reevaluation process on
Name:
/
/
Current Eligibility Category(s):
/
/
Position:
:
Date of Participation:
/
/
/
/
/
/
/
/
/
/
Review of Existing Data
Record Review (e.g. attendance, past and current grades, work samples, state and district-wide assessment data, relevant
medical/health information, discipline reports, IEP progress):
Summary of previous assessment(s) (If attaching the most current summary of evaluation/eligibility worksheet, results must be
discussed below):
Summary of evaluations and information provided by the parent(s):
Summary of classroom based assessments and observation:
Summary of observations by teachers and service providers:
Determination of Needed Additional Data, if any
Is additional data needed to determine:
A) Continued eligibility for special education and related services:
If the student continues to have such a disability and educational needs?
If the student continues to need special education and related services?
B) Present level of academic achievement and developmental needs?
C) Whether any additions or modifications to special education and/or related services
are needed to meet measurable annual goals and participation in the general curriculum?
Yes
Yes
Yes
No
No
No
Yes
No
If yes to any of the above, which will occur? (check one or both and discuss):
Collection of the following data without formal assessment: (Complete Eligibility Worksheet(s), Complete Eligibility
Determination, Address IEP, and Complete Prior Written Notice.)
Collection of the following data through formal assessment: (Obtain Parental Permission. Complete Eligibility Worksheet(s),
Complete Eligibility Determination, Address IEP, and Complete Prior Written Notice.)
If no additional data or assessment is needed, explain why: (Complete Eligibility Determination, Address IEP and Complete
Prior Written Notice.)
I disagree with the IEP Team decision to obtain no additional assessment information concerning my child. I request that
additional assessment(s) be completed prior to determining continuing eligibility.
(Parent Signature)
Copy to: Parent(s) / EC File
_____/_____/_____
(Date)
Moore County Re-evaluation Forms
The following forms are required by Moore County schools as a part of the gathering of information for the
reevaluation process.
MOORE COUNTY SCHOOLS
Parent Re-evaluation Questionnaire
Student Name _______________________________
Grade_________
School _____________________________________
Date__________
Name of Parent Completing this Form_______________________________________________
1. What concerns do you have (if any) about your child’s academic progress?
2. What concerns do you have (if any) about your child’s school behavior?
3. Do you feel your child’s current Exceptional Education placement has been helpful?
4. Are there ways the current Exceptional Education placement can be improved? If yes, please explain.
5. What additional information do you believe we need about your child?
MOORE COUNTY SCHOOLS
Student Re-evaluation Questionnaire
Student’s Name______________________________________
School_________________________________
Grade_______________
Teacher_______________
Date______________
1. Are the special services you are receiving helping you in school?
2. Could the services you are receiving be changed to help you better? How?
3. What extra or different things do your teachers do to help you learn better?
4. Are there other things your teachers could be doing to help you learn better?
5. What concerns do you have about how you are doing in school?
6. Do you think you need more extra help? What kind would be most helpful?
7. Would you like more extra help? With what?
MOORE COUNTY SCHOOLS
Teacher Re-evaluation Questionnaire
Student Name_________________________________________
Grade___________
Teacher Name_________________________________________
Date ____________
1. What are your current concerns about this student?
2. What are this student’s academic and/or behavioral strengths?
3. What are this student’s academic and/or behavioral weaknesses?
4. What modifications is the student currently receiving in the classroom and what (if any) changes in
modifications would you recommend?
5. Describe this student’s academic skill level relative to other students in your class.
6. Describe this student’s rate of academic progress under the current placement?
7. What (if any) changes would you make to this student’s current placement?
8. What additional information (if any) do you need to answer any of the above questions?
MOORE COUNTY SCHOOLS
Student Record Review Form
For re-evaluations
Student Name_______________________________________School_____________________
Grade:_____Date of Birth:__________________Teacher______________________________
School History (at least last 3 years, if applicable):
Grade
Absences
Days Enrolled
Tardies
Grades Received (at least last 3 years, if applicable):
Year
Grade
Reading
Math
Writing
Science
State Test Data (at least last 3 years, if applicable):
ELEMENTARY
Year
Grade
Reading EOG Math EOG
Writing
HIGH SCHOOL
Year
Grade
Biology
English I
Algebra
USHx
ELPSA
Social Stu.
English II
Record any other standardized group testing results within the past 3 years_____________
______________________________________________________________________________
Health Information
Describe any current medical condition or needs____________________________________
_____________________________________________________________________________
Is this student on any medication(s)? Yes/No If, yes, explain__________________________
Most recent vision and hearing screening results
Visual acuity: Far
pass/fail
date_________________
Near pass/fail
date_________________
Hearing
pass/fail
date_________________
Worksheet 1 (Page 1 of 2)
COMMUNICATION PLAN WORKSHEET FOR STUDENT WHO IS DEAF OR HARD OF HEARING
Student:
DOB:
School:
/
/
Grade:
Primary Area of Eligibility:
Secondary Area(s) of Eligibility: (if applicable)
Date of IEP meeting when Communication Plan Worksheet was completed:
/
/
.
I. CONSIDER THE STUDENT’S LANGUAGE AND COMMUNICATION NEEDS.
1. The student’s primary language is one or more of the following (check all that apply):
Receptive Expressive
English
American Sign Language
Native language
2. The student’s primary communication mode is one or more of the following (check all that apply):
Receptive
Auditory
Conceptual signs (e.g. American Sign Language, Pidgin Signed English (PSE) also referred to as CASE)
English signs (e.g. Manually Coded English such as Signed English or Signing Exact English)
Fingerspelling
Gestures
Speechreading
Tactile
Cued Speech
Other, please explain:
Expressive
Conceptual signs [e.g. American Sign Language, Pidgin Signed English (PSE) also referred to as Conceptually Accurate
Signed English (CASE)]
English signs (e.g. Manually Coded English such as Signed English or Signing Exact English)
Fingerspelling
Gestures
Speechreading
Tactile
Cued Speech
Other, please explain:
3.
What language(s) and mode(s) of communication do the parents use with their child? What modes does the child use with
peers?
4.
Comments (optional):
II. CONSIDER OPPORTUNITIES FOR DIRECT COMMUNICATIONS WITH PEERS AND PROFESSIONAL
PERSONNEL AND OPPORTUNITIES FOR INSTRUCTION IN THE CHILD’S LANGUAGE AND
COMMUNICATION NEEDS.
1.
Describe opportunities for direct communication with peers.
2.
Describe opportunities for direct communication with professional staff and other school personnel.
3.
Describe opportunities for direct instruction.
Direct language/communication/instruction occurs person to person, not through an additional source (e.g., educational
interpreter, captioner. These social, emotional and academic opportunities may be provided by the school or family.)
Worksheet 1 (Page 2 of 2)
Communication Plan Worksheet for Student Who Is Deaf or Hard of Hearing
Student:
School:
DOB:
/
/
Grade:
III. CONSIDER ACADEMIC LEVEL.
1.
Does the student have the communication and language necessary to acquire grade-level academic skills and concepts in the
general education curriculum?
Yes
No
If yes, what supports are needed to continue proficiency in grade-level academic skills and concepts of the general education
curriculum?
If no, what supports are needed to increase the student’s proficiency in his/her language and communication to acquire gradelevel academic skills and concepts of the general education curriculum?
IV. CONSIDER FULL RANGE OF NEEDS.
1.
Does the child have access to all educational components of the school (regular education classes, related services, guidance
counseling, recess, lunch, assemblies, extra curricular activities, etc.)? If not, what supports are needed to allow for access?
2. Are adult language models available who communicate in the student’s language/communication mode?
3. What accommodations/modifications are being provided? What additional accommodations/modifications were considered?
V. CONSIDER AMPLIFICATION NEEDS.
Personal hearing devices (hearing aid, cochlear implant, tactile device)
Personal FM system
FM system/auditory trainer (w/o personal hearing device)
Soundfield system
No Amplification needed
Place Completed Worksheet in EC Folder
Moore County Schools
ESY Determination
Worksheet 1
IDEA requires the consideration of extended school year services for each student with a disability. The IEP team determines
on an individual basis, annually, what services, if any, are necessary.
LEAs must ensure extended school year services are available as necessary to provide FAPE.
ESY services are provided beyond the scope of the traditional school year, outlined in the IEP, and are provided at no cost to
the parent.
The LEA cannot limit the services to certain categories of disability, nor can the LEA unilaterally limit the type, amount or
duration of the services. ESY services may be provided at any time during the calendar year other than the instructional day.
This ESY worksheet allows the IEP team the opportunity to examine the data available and respond to the following.
EXTENDED SCHOOL YEAR DETERMINATION
Student:
Primary Area of Eligibility:
School:
Date:
/
/
Secondary Area of Eligibility: (if applicable)
Data is required. Data must be documented and summarized for consideration of ESY services.
I.
ESY Services Determination
A. The student regresses or may regress during extended breaks from instruction, cannot relearn the lost skills within a
reasonable time and the gains made during the regular school year will be significantly jeopardized.
yes
no
Summarize the data considered when determining the need for ESY services.
Instructional Break/Recoupment Formula Guide:
3 months = 9 weeks to regain skill
1 month = 3 weeks to regain skill
3 weeks = 2 ½ weeks to regain skill
2 weeks = 1 ½ weeks to regain skill
1 week = 3 ½ days to regain skill
Does the data show that after a break of ________weeks it takes LONGER THAN _________weeks for the student to relearn
skills lost over the break.
The following questions may be used to help guide the IEP team to elaborate on the data presented:
Does the student need extensive review to demonstrate previously learned skills?
What inconsistencies does the student demonstrate in mastered or partially acquired skills?
Has the student reached a critical point of instruction where a break in programming would have serious, detrimental effects?
Does the student demonstrate behaviors or deficits that would cause regression if breaks in programming occur?
Is there a medical condition that might cause regression? How does this affect rate and maintenance of progress?
Will a break in programming jeopardize the student’s placement in the LRE?
Will a break in programming cause significant problems for the child who is learning a critical skill (like reading)?
B. The student is demonstrating emerging critical skill acquisition (“window of opportunity”) that will be lost without the
provision of an educational program during extended breaks from instruction.
yes
no
Summarize the data considered when determining the need for ESY services.
The IEP team reviews all IEP goals targeting emerging critical skills to determine whether any of these skills are at a
breakthrough point. When skills are at this point, the IEP team needs to determine whether the interruption in
services and instruction on those goals or objectives is likely to prevent the student from receiving benefit from his/her
educational program during the regular school year without these services.
C. Based on the information above, the IEP Team has determined the student ____is ____is not in need of ESY Services.
(Need for ESY service requires one affirmative answer to the statements above.)
One blank must be checked.
II. ESY Services Description : Describe the ESY program for this student by indicating the type of service (special education
and/or related service), the number of sessions, length of sessions, and location of sessions (School or Home)
Type of Service
SPECIAL EDUCATION
Specify HI or VI
Specify if work packet with monitoring,
In-home consultation/instruction
RELATED SERVICES
Specify OT, PT or Speech
Place completed worksheet in EC folder.
Copy given/sent to parent(s): / /
1/09
Number of Sessions
Length of Sessions
Location of Sessions
How many sessions
over the break?
Duration of each
session
School or Home
Moore County Schools
ESY Determination
Worksheet 1
EXTENDED SCHOOL YEAR DETERMINATION
Student:
School:
Primary Area of Eligibility:
I.
Date:
/
/
Secondary Area of Eligibility: (if applicable)
ESY Services Determination
A. The student regresses or may regress during extended breaks from instruction, cannot relearn the lost critical skills within a
reasonable time and the gains made during the regular school year will be significantly jeopardized.
yes
no
Summarize the data considered when determining the need for ESY services.
B. The student is demonstrating emerging critical skill acquisition (“window of opportunity”) that will be lost without the
provision of an educational program during extended breaks from instruction.
yes
no
Summarize the data considered when determining the need for ESY services.
C. Based on the information above, the IEP Team has determined the student ____is ____is not in need of ESY Services.
(Need for ESY service requires one affirmative answer to the statements above.)
II. ESY Services Description : Describe the ESY program for this student by indicating the type of service (special education
and/or related service), the number of sessions, length of sessions, and location of sessions (School or Home)
Type of Service
Number of Sessions
SPECIAL EDUCATION
RELATED SERVICES
Place completed worksheet in EC folder.
Copy given/sent to parent(s):
/
Last Updated 1/28/09
/
Length of Sessions
Location of Sessions
Moore County Schools
ESY Determination
Worksheet 2
ESY STUDENT INFORMATION CHECKLIST
(Please Address All Listed Information With Either An Answer Or With N/A. Leave No Items Blank.)
Name
Parent/Guardian Name and Number (Work and Home)
IDENTIFYING INFORMATION
NC Wise #
Home Address (Street, City, Zip Code)
Emergency Contact & Number
TRANSPORTATION
Is Transportation Needed: Yes___ No___
AM Address
PM Address
Special transportation factors. (Child safety restraint system, lift bus, car seat, air conditioning,
etc).
MEDICAL INFORMATION
Medication(s) – (Where given & when)
Allergies
Seizures
Other (Attach info. if needed.)
Current School
Current Teacher
Can we reach you this summer?
PRESENT EDUCATIONAL INFORMATION
Type of class
Grade
Email
Yes ___ No ___
Phone
Is extra TA assistance needed for ESY?
Yes ___ No ___
If yes, explain why extra TA assistance is needed for ESY and the duties that person would need
to perform. Be brief but specific.
Is current TA willing to work ESY?
Yes ___, TA Name _______________________ No ___
WHAT TO SEND & WHO TO SEND IT TO
ESY Determination Worksheets 1 and 2 to Laura Dendy
Entire IEP /objectives that need to be worked on underlined with sample data collection,
Progress Report, ( FBA/BIP, Health Plan, if appropriate). All to Laura Dendy
Information regarding method of communication and/or Assistive Technology, schedules,
toileting, work systems, etc., that would help in teaching child (use back) to Laura Dendy
If student will be served by a teacher other than yourself send all work materials to Laura Dendy by
June 8.
*This form was completed by: __________________________________________________________
Services Plan for Parentally-Placed Private School Student Directions
(Workseet 3 pg.1)
Moore County schools meets its requirements of serving privately placed students through our Speech
Language referrals in private placements; therefore this form in only used by our Speech Pathologists.
Select the purpose of the Services Plan and check the appropriate box.
Complete the dates for the duration of the services plan, not to exceed the end of the current school year.
Complete the student’s full name, date of birth, site of private school, and grade.
Write in the name of the LEA and the services that the LEA determined that it will provide for the school year.
Write the school year that services will be provided. Write in the student’s full name.
List the student strengths indicated by members of the IEP team including parents. The strengths should be
based on academic skills, functional skills, and personal skills.
Parent(s) should be given the opportunity at the meeting to address concerns about he student’s education.
The special factors area should be discussed and completed by the IEP team.
The present level of performance should include strengths and needs applicable to the areas provided by the
service plan.
Worksheet 3
Services Plan (Page 1 of 2)
SERVICES PLAN FOR PARENTALLY-PLACED PRIVATE SCHOOL STUDENT
Purpose:
Initial Eligibility
Annual Review
Duration of Services Plan: From:
Student:
Site:
Primary Area of Eligibility:
/
Reevaluation
/
To:
/
Addendum
/
DOB:
/
/
Grade:
Secondary Area of Eligibility: (if applicable)
(LEA) has determined that it will make available
services to eligible parentally placed private school students with
disabilities during the
school year. This Services Plan describes the specific services to be provided to
.
Student’s overall strengths:
Concerns of the parent for enhancing the student’s education:
Describe any special factors (behavior, English Language proficiency, communication needs, assistive technology/services) that are
relevant to this student:
Present Level of Academic Achievement and Functional Performance: Consider the results of the initial or most recent evaluation and other relevant
data. Include specific descriptions of strengths and needs that apply to the current academic, developmental, and functional performance, behaviors, and social
emotional development. State how the child’s disability affects the child’s involvement and progress in the general education curriculum. For preschool children, as
appropriate, state how the disability affects the child’s participation in appropriate activities.
Services Plan for Parentally-Placed Private School Student Directions
(Workseet 3 pg.2)
The academic or functional goal(s) for the student must be written in measurable terms.
Data must be collected to show progress toward the particular goal. Documentation must be maintained.
Examples of measuring progress could be formal and informal assessments, work samples, etc.
Completion of this section is only required if the LEA’s schedule for progress monitoring is different than at
issuance of report cards.
The number of sessions per Week/Month/ or Semester should be indicated. The time per session should be
addressed in minutes or hours. A range of time may not be used. For example, the location should indicate
general education classroom if the services are to be offered at the private school in the child’s classroom.
Location indicates the place in the LEA that the parent and LEA agreed upon for delivery of services.
Explain if the LEA is to provide transportation to the child. If the LEA provides transportation, the cost may be
calculated as part of the required proportionate share.
While signatures are not required, participants in the meeting and their positions must be captured. LEAs are
not prohibited from requiring signatures. Moore County Schools does require signatures on this document.
Worksheet 3
Services Plan (Page 2 of 2)
Annual Academic or Functional Goal 1:
Method of Measuring Progress:
Annual Academic or Functional Goal 2:
Method of Measuring Progress:
Unless otherwise described below, progress toward the annual goal(s) will be reported at the issuance of report cards.
Anticipated Frequency and Location of Services:
Type of Service
# Sessions
Week
Month
Semester
Time per Session
Is transportation necessary for the child to benefit from or participate in the service?
If yes, explain:
The following individuals participated in developing the Services Plan:
Name
Position
The following individuals participated in developing an addendum to the Services Plan:
Name
Position
yes
Location
no
Date
/
/
/
/
/
/
/
/
Date
/
/
/
/
/
/
/
/
Special Education services
MDR
Moore County Schools
MANIFESTATION DETERMINATION REVIEW
Name: ________________________NCWise#____________ Grade: ____School: ______________
DOB: ___/ ___/ ___
Area of Disability: ________________________
Date of Suspension: ___/___/___ Date of MDR: ___/___/___
Length of Suspension: _____________________
Total # of Days of Previous Suspensions: _____________________
V. BEHAVIOR THAT LED TO DISCIPLINARY ACTION
a.
Describe the behavior that led to this suspension. (Attach the Suspension Notice)
_________________________________________________________________________________
_________________________________________________________________________________
VI.
MANIFESTATION DETERMINATION
Relationship between the conduct in question and the child’s disability:
Date of most recent (re)evaluation (This is the date of the last eligibility meeting) ____ / ____ / ____
a.
Summarize the concerns noted during the most recent evaluation, including review of DEC3, psychological report,
and other evaluation records. ___________________________________________________________________
_______________________________________________________________________________
_______________________________________________________________________________
s
Title
_______________________________________________________________________________
b.
Summarize results of any FBA conducted on the student. _____________________________________________
_______________________________________________________________________________
c.
Summarize Individualized Education Program (IEP) goals [including BIP objectives]
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
d.
List any medical/health diagnosis and whether prescription medication is used.
_______________________________________________________________________________________________
e.
Has this or similar behaviors been exhibited in the past; If so, describe the pattern of behaviors.
_______________________________________________________________________________________________
_______________________________________________________________________________________________
f. List any additional information from parents or staff
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
Summary Question #1: Was the conduct in question caused by, or had direct and substantial relationship to, the
child’s disability?
□ YES
□ NO
(IF YES, PROCEED TO SECTION III)
Student Name:________________________ School: __________________Today’s Date: _________
RELATIONSHIP BETWEEN CONDUCT IN QUESTION AND THE FAILURE TO IMPLEMENT THE IEP:
d.
Individualized Education Program (IEP) date: _____________________ to ______________________
e.
Has a Behavior Intervention Plan been developed?
If so, has it been implemented?
f.
Was the Individualized Education Program, including modifications and supplementary services, being implemented?
□ Yes
□ Yes
□ Yes
□ No
□ No □ n/a
□ No
If NO, describe what part of the IEP was not implemented_________________________________________
___________________________________________________________________________________________
Summary Question #2: Was the conduct in question a direct result of the LEA’s failure to implement the IEP?
□ YES
□ NO
VII.
MANIFESTATION STATEMENT: CHECK ONE
If the answer to EITHER of the summary questions is YES, then the behavior IS a manifestation of the student’s disability.
If the answer to BOTH of the summary questions is NO, then the behavior IS NOT a manifestation of the student’s
disability.
Was a manifestation of the student’s disability
Based on the information considered,
the IEP team determined that the misbehavior
Was not a manifestation of the student’s disability
If the incident WAS a manifestation, student may not be suspended. Required actions:
Develop new FBA/BIP or review/revise
existing BIP, as necessary, to address the
behavior.
Complete DEC5/Prior Written Notice
Student returns to the placement prior to suspension
UNLESS subject to 45-school day interim alternative
educational setting OR IEP team agrees to a change in
placement as part of a behavioral intervention.
If the incident WAS NOT a manifestation student may be suspended. Required actions:
VIII.
NAME
Determine the services needed to enable the
student to participate in the general curriculum
and to progress towards IEP goals while on
suspension
Complete DEC5/Prior Written Notice
Address the IEP and/or develop a behavioral
intervention plan as appropriate
SIGNATURES
POSITION
DATE
LEA Representative
Special Education Teacher
Regular Education Teacher
Parent
Revised March 2009
Moore County Schools
Special Education Services
Monthly Review of Home/Hospital Instruction (Change of Placement due to Discipline)
Name of Student:
NCWISE#:
DOB:
/
/
School:
Grade:
Beginning/Ending Dates of Student’s Current IEP
From:
/
/
To:
/
/
NC 1504-2.9: If a change of placement occurs under the discipline requirements of Policies Governing Services for Children with
Disabilities, the local educational agency shall not assign a student to homebound instruction without a determination by the
student’s IEP team that the homebound instruction is the least restrictive alternative environment for that student. If it is
determined that the homebound instruction is the least restrictive alternative environment for the student, the student’s IEP team
shall meet to determine the nature of the homebound educational services to be provided to the student. In addition, the continued
appropriateness of the homebound instruction shall be evaluated monthly by the designee or designees of the student’s IEP team.
Initial Date of Home/Hospital Instruction:
Date of Review:
/
/
/
/
This is the date that
Home/Hospital Services
begin as documented on
the student’s IEP.
(This review is to be held within 30 days of initial date or date of last review)
Review must take place within 30 days of initial
date as documented on the student’s IEP. If
student continues on H/H then a review must be
conducted every 30 days.
Description of Data* Reviewed by Designee(s):
__________________________________________________________________________________________
__________________________________________________________________________________________
Data described here can include progress data on the student’s
__________________________________________________________________________________________
IEP goals, attendance information, description of student’s
courses on H/H and grades within each course, review of
__________________________________________________________________________________________
current services provided based on the student’s IEP, review
__________________________________________________________________________________________
of data from district and course assessments, etc.
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________
*Data reviewed should include progress data on student’s IEP goals, completion of assignments, attendance information, grades, and
progress in North Carolina Standard Course of Study (general education curriculum).
Moore County Schools
Special Education Services
Monthly Review of Home/Hospital Instruction (Change of Placement due to Discipline)
Name of Student:
NCWISE#:
DOB:
/
/
School:
Beginning/Ending Dates of Student’s Current IEP
Results of Review (Choose One):
Grade:
From:
/
/
To:
/
/
Signature(s) and Title(s) of Designee(s)Date:
Home/Hospital Instruction will continue,
review will be conducted within 30 days.
Based on review of data,
designee(s) determine that H/H
continues to be appropriate.
H/H plan is being implemented
as determined by IEP Team.
Home/Hospital will continue with the
following action(s), review will be
conducted within 30 days:
Based on review of data, designee(s)
determine that H/H continues to be
appropriate. However, additional
action(s) need to be taken. For
example: H/H services are taking place
in the student’s home and based on
review a new location would be less
distractible; there is no formal system
for communicating assignments with
the parents so a communication system
will be developed, etc.
*Changes to the IEP must be done through the IEP Process.
Home/Hospital will continue, IEP Meeting
will be scheduled to discuss
appropriateness of H/H services within 10
school days.
Based on review of data,
designee(s) can not determine
whether H/H continues to be
appropriate. Continue H/H
services until the IEP team
meets (within 10 school days of
review) to discuss concerns and
amend current plan or develop
a new plan for services.
IEP Team LEA should designate at least one
person to review the H/H services monthly. If
additional designees are needed to provide data,
discuss progress, etc. they should be included as
needed at each review.
Review forms should be
completed every 30 days.
All Review Forms should be
placed in the student’s
Confidential File with the
current IEP documenting
Home/Hospital services. These
forms are subject to review by
IEP LEA/School Administrators,
WCPSS Compliance Team
and/or NCDPI Monitoring
Team(s).
Moore County Schools
Special Education Services
Monthly Review of Home/Hospital Instruction (Change of Placement due to Discipline)
Name of Student:
NCWISE#:
DOB:
/
/
School:
Beginning/Ending Dates of Student’s Current IEP
Grade:
From:
/
/
To:
/
/
NC 1504-2.9: If a change of placement occurs under the discipline requirements of Policies Governing Services for Children with
Disabilities, the local educational agency shall not assign a student to homebound instruction without a determination by the
student’s IEP team that the homebound instruction is the least restrictive alternative environment for that student. If it is
determined that the homebound instruction is the least restrictive alternative environment for the student, the student’s IEP team
shall meet to determine the nature of the homebound educational services to be provided to the student. In addition, the continued
appropriateness of the homebound instruction shall be evaluated monthly by the designee or designees of the student’s IEP team.
Initial Date of Home/Hospital Instruction:
/
/
Date of Review:
/
/
(The review is to be held within 30 days of initial date or date of last review)
Description of Data* Reviewed by Designee(s):
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________
*Data reviewed should include progress toward a student’s IEP goals, completion of assignments, attendance information, grades, and
progress in North Carolina Standard Course of Study (general education curriculum).
Results of Review (Choose One):
Home/Hospital Instruction will continue,
review will be conducted within 30 days.
*Home/Hospital will continue with the
following actions, review will be conducted
within 30 days:
*Changes to the IEP must be done through the IEP Process.
Home/Hospital will continue, IEP Meeting
will be scheduled to discuss
appropriateness of H/H services within 10
school days.
Signature(s) and Title (s) of Designee(s)/Date:
DEC 9
MOORE COUNTY SCHOOLS
Programs for Exceptional Children
MAINTENANCE OF AND ACCESS TO RECORDS
Parental consent is required prior to release of records except the following:
(1)
School officials within the local educational agency who have legitimate educational interests.
(2)
School officials of other local educational agencies in which the student intends to enroll or obtain
services.
(3)
Certain authorized representatives of the state and federal government who are determining eligibility of
the child for aid as provided under Public Law 93-380.
(4)
All other persons may gain access to a student’s record only with the specific written consent of the
parent(s) or guardian(s) or eligible student.
(5)
Recipients of student records should be cautioned that student information may not be released to third
parties without the consent of the parent or legal guardian.
Name of Student ______________________________________
I have inspected the records of the above student.
Signature
_______________________
_______________________
_______________________
_______________________
_______________________
_______________________
_______________________
_______________________
Date
___________
___________
___________
___________
___________
___________
___________
___________
Purpose
____________________________
____________________________
____________________________
____________________________
____________________________
____________________________
____________________________
____________________________
Authorized By:
________________________
________________________
________________________
________________________
________________________
________________________
________________________
________________________
DEC 10
PARENT CONTACT LOG
DATE
REASONS
P.O. Box 1180 ● Carthage, North Carolina 28327 ● 910-947-2976 ● FAX 910-947-3011
RELEASE TO SHARE INFORMATION
This is to state that I give my permission to ___________________________________
(Agency/School/Institution)
to release *information to ________________________________________________
(Agency/School/Institution)
concerning ____________________________________ _______________________
(Name of Student)
(Date of Birth)
Disclosure of this information will facilitate identification and placement decisions for my
child. All information will be carefully and confidentially handled. I am entitled to all the
due process rights in the Handbook of Parent Rights, which I have received or may
obtain an additional copy from my child’s school upon request.
________________________________
(Parent/Guardian Signature)
________________________________
(Date)
*Check Requested Items
___Pre-referral
___Referral
___Consent to Evaluate
___Screenings/Evaluations
___Summary of Evaluations
___Invitation to Conference
___Individual Education Plan
___Consent to Place
___Medical Records (current)
___Other (Specify)
_____________________________
____________________________
**********************************************
RETAIN A COPY IN CHILD’S FOLDER
**********************************************
DEC 21
Moore County Schools
Programs for Exceptional Children
REQUEST FOR SCREENING/EVALUATION
Date:____________
Student:____________________________Grade:_____ School:________________________
The above named student has been referred for consideration for exceptional education
services. The following assessment is needed to help the School-Based Committee make a
placement recommendation or to complete an evaluation.
Thank you for your help.
Screening/Evaluation Needed:
(
(
(
(
(
(
(
(
(
)
)
)
)
)
)
)
)
)
Intellectual/Ability/Cognitive
Educational/Achievement
Motor screening/Evaluation
Behavioral/Emotional Evaluation
Adaptive Behavior Evaluation
Hearing Screening/Evaluation
Physical Therapy Evaluation
Occupational Therapy Evaluation
Other________________________
(
(
(
(
(
(
(
(
(
)
)
)
)
)
)
)
)
)
Social Developmental History
Analysis of Grades
Vocational Assessment
Vision Screening/Evaluation
Speech Language Screening/Eval.
Auditory Processing Evaluation
Health Screening
Medical Evaluation
Other_________________________
____________________________________________
Signature – IEP Team Chairperson
Results:_______________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
__________________________________________
Evaluator's Signature
_______________________
Date
Document Receipt Form Directions
This form is to be used any time a parent requests copies from the student’s EC folder other than
just the current IEP. Parents have a right to ask for any part of their child’s folder, however it is
important to document when it was given.
MOORE COUNTY SCHOOLS
DEPARTMENT OF EXCEPTIONAL EDUCATION
DOCUMENT RECEIPT FORM
Student Name: ___________________________________________________________
Date of Birth: ____________________________________________________________
School: _________________________________________________________________
Document/s given to Parent/Guardian/Student:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
Date requested by Parent/Guardian/Student: ____________________________________
Date given to Parent/Guardian/Student: _______________________________________
Signature of Parent/Guardian/Student: ________________________________________
Signature of School Employee giving documents: _______________________________
(A copy of this form is to be given to the parent/guardian/student; a copy is to be placed in the
student’s EC file; and a copy is to be sent to the Exceptional Education Office.)
MCS/EC/FY04.1
Folder Order (Left Side) (Initial Placement Paperwork Only)
Last Name, First Name, Date of Birth (Write on Folder Tab)
Top
DEC 10 Parent Contact Log
Invitation
DEC 1 Special Education Referral
DEC 2 Consent for Evaluation
DEC 5 Prior Written Notice
SST Documentation or Infant Toddler Documentation and Preschool (Documentation from Previous
State if Out of State Transfer)
Minutes
Invitation
Psychological and/or other evaluation reports
DEC 3 Worksheet
DEC 3 Eligibility Determination Sheet
DEC 4 IEP (with progress notes once completed)
COSF (Child Outcome Summary Form)
Review of Accommodations Form
DEC 5 Prior Written Notice
Minutes
DEC 6 Consent for Services
DEC 9 Maintenance and Access of Records
Bottom
Folder Order Right Side
Progress reports attached to IEP to which goals it documents.
Each meeting is placed in chronological order as it occurs.
Each subsequent meeting is placed on top of prior meeting with a completed cover sheet.
*Protocols should not remain in the new folders if discussed in a report. These may be kept in a working
folder.
Samples:
Annual Review
Cover sheet
Invitation
DEC 4
COSF
Review of Accom.
Progress Notes
DEC 5
Minutes
Reeval. w/ Testing
Cover Sheet
Invitation
Questionnaires
DEC 7
DEC 2
DEC 5
Minutes
Invitation
Evaluation Reports
DEC3 Worksheet and
Eligibility Det.
DEC 4
DEC 5
Minutes
Reeval. w/o Testing
Cover Sheet
Invitation
Questionnaires
DEC 7
DEC 3 Elig. Det.
DEC 4
DEC 5
Minutes
IEP Progress Report Directions
This progress report can be copied and saved into its own document in order for
you to type your progress reports.
NOTE: This form is to be used as an interim until you are able to complete
IEP progress on CECAS.
Moore County Schools
Individual Education Plan Progress Report
Student:
School:
Teacher:
Present Grade:
CODES
DATE:
Annual Goals/Objectives
Comments
1st Nine
Weeks
Date:
2nd Nine
Weeks
Date:
3rd Nine
Weeks
Date:
4th Nine
Weeks
Date:
School Year:
Report of Progress: MS=Mastered
SP=Slowly Progressing NP=No Progress
1st
Progress
Report
1st
Report
Card
2nd
Progress
Report
2nd
Report
Card
3rd
Progress
Report
P=Progressing
NA=Not Addressed Yet
3rd
Report
Card
4th
Progress
Report
4th
Report
Card
Graduation Documentation/Exit Forms
The following is a letter explaining the Summary of Performance in detail. There
are also directions included for completing the summary of performance and a
blank Moore County Summary of Performance Form.
Guidance for Developing a Summary of Performance
The following information may be used as a guide to assist LEAs in meeting the IDEA 2004
requirements for students whose special education eligibility terminates due to graduation or
exceeding the age of eligibility. Under these new provisions, the LEA shall provide the student
with a summary of the student’s academic achievement and functional performance, which
includes recommendations on how to assist the student in meeting his/her desired postsecondary
outcomes.
Student ________________
Date _________________
LEA ___________________
School _______________
Reason for termination of eligibility (check one):
Graduated with a diploma □
Exceeds age limit □
Provide a written summary of the following:
A. Student’s academic achievement:
This may include, but is not limited to the following:
Reading – basic reading/decoding, reading comprehension, and reading speed;
Math – calculation skills and math problem solving;
Written language – written composition, written expression, and spelling;
Class participation, note taking, keyboarding homework management, time
management, study skills, and test taking skills;
General ability and problem solving – reasoning, attention and executive functioning
– energy level, sustained attention, processing speed, impulse control, and activity
level; and
Communication – speech/language and augmentative communication.
NOTE: The high school transcript should be included to document credits earned, course of
study, and grades earned.
B. Student’s functional performance:
This may include, but is not limited to the following:
Social skills and behavior, interaction with teacher/peers;
Level of initiation in asking for assistance;
Responsiveness to services and accommodations;
Involvement in extracurricular activities;
Emotional or behavioral issues related to learning and/or attention;
Self-care;
Mobility and Self-determination;
Safety; and
Technology use and skills, etc.
C. Recommendations on how to assist the student in meeting his/her desired postsecondary
outcomes:
This may include, but is not limited to the following:
Essential accommodations and modifications;
Assistive technology;
Activities such as attending college orientation and meeting with vocational rehabilitation
counselor;
Independent living/daily living;
Employment; and
Community experiences.
Moore County Schools
P. O. Box 1180
Carthage, NC 28327
919-947-2976
Summary of Performance
Student___________________________________________Date__________________
LEA_____________________________________________School_________________
Reason for termination of eligibility (check one):
Graduated with a diploma □
Reached age limit
□
Provide a written summary of the following:
A. Student’s academic achievement:
B. Student’s functional performance:
C. Recommendations on how to assist the student in meeting his/her desired
postsecondary outcomes:
Completed by: _____________________________Position:______________________
Date Completed: _____________________________
SUMMARY OF STUDENT PERFORMANCE
The Summary of Performance provides students who are either graduating with a diploma or exiting due to
age with a summary of current academic achievement and functional performance, including
recommendations on how to assist the student in meeting postsecondary goals.
Student:____________________________ Date of Birth:____________ Graduation Date/Exit:________
LEA:______________________________ School:_____________________________________
Reason for Termination of Eligibility:
___Graduated with diploma
___Reached Age Limit
Summary of Academic Achievement
Oral Reading:
Independent Skill____
Assistance required____
Nonreader____
Reading Comprehension: Independent Skill____
Assistance required____
Nonreader____
In the area of reading, the student:
____demonstrates consistent performance in a superior manner clearly beyond that required to be proficient
____demonstrates consistent mastery of knowledge and skills
____demonstrates inconsistent mastery of knowledge and skills
____does not yet have sufficient mastery of knowledge and skills
Reading Skills Mastered
Reading Skills in Progress
Written Expression: ____Accurately communicates using appropriate writing conventions
____Requires editing assistance
____Requires use of word processor or other assistive technology
____Communicates in writing only with the support of a scribe
In the area of written expression, the student:
____demonstrates consistent performance in a superior manner clearly beyond that required to be proficient
____demonstrates consistent mastery of knowledge and skills
____demonstrates inconsistent mastery of knowledge and skills
____does not yet have sufficient mastery of knowledge and skills
Written Expression Skills Mastered
Mathematics Level:
Written Expression Skills In Progress
____Has successfully completed General Education Math courses
(Algebra or above) with minimal or no assistance
____Has successfully completed Occupational Math courses
____Is independent with basic math computations
____Is independent with basic math computations only when using a calculator
____Requires assistance with operations beyond basic computation
____Unable to do basic computation or functionally demonstrate math skills
In the area of mathematics, the student:
____demonstrates consistent performance in a superior manner clearly beyond that required to be proficient
____demonstrates consistent mastery of knowledge and skills
____demonstrates inconsistent mastery of knowledge and skills
____does not yet have sufficient mastery of knowledge and skills
Mathematic Skills Mastered
Mathematic Skills In Progress
Learning and Work Skills:
____Participates in class
____Performs well on tests
____Has good time management skills
____Enjoys learning
____Works in a timely manner
____Attends well to academic tasks
____Works cooperatively in a group
____Organized
____Pays attention in class/job site
____Shows interest/motivation in work
____Is punctual
____Accepts criticism and makes changes
____Has an acceptable energy level
____Completes assignments ____% of the time.
____Takes notes
____Can maintain sustained attention (___ minutes)
____Studies and prepares
____Behavior is appropriate and acceptable
____Attends well to hands-on tasks
____Works well independently
____Shows initiative (does what is needed before being asked)
____Begins assignments on time in class and on job site
____Gives best effort when completing work/tasks
____Dependable (can be counted on to what is needed)
____Is flexible (adapts to schedule changes/unexpected events)
____Has an acceptable stamina level
Vocational Assessments Administered:
____Interest (Describe:__________________________________________________________________)
____Aptitude (Describe:_________________________________________________________________)
____Learning Styles (Describe:___________________________________________________________)
____Other (Describe:___________________________________________________________________)
Social Skills/Self-Determination
____ Interacts well with adults
____Interacts well with peers
____ Initiates asking for assistance
____ Shares information in conversation/turn-taking
____Recognizes the feelings of others
____Uses good manners
____Refrains from inappropriate touching ____Uses good judgment when frustrated or challenged
____Uses an appropriate voice level
____Uses appropriate language in the classroom/job site
____Accepts feedback appropriately
____Cooperates with classmates/teachers/supervisors
____Sets goals for the future
____Can develop plans and take actions related to achieving goals
____Can self-advocate
____Is comfortable making choices regarding routine life events
____Has good problem-solving skills
____Is comfortable making choices about major life events
____Exhibits acceptable impulse control
School Attendance:
Safety Awareness:
____ A Strength
____ A Strength
____ Satisfactory
____ Satisfactory
____ Needs Improvement
____ Needs Improvement
Transportation after graduation will consist of:
____ Driver’s license
____ Family/Friends
____ Public Transportation
____ Private Transportation
____ Ride Share
____Walking
____ Bicycle
____ Other (________________________________)
Accommodations that have been effectively utilized:
___Calculator
___Dictation to a Scribe
___Spell Check Device
___Visual/Verbal Cues
___Picture Schedule
___Extended Test Time
___Written Checklists
___Repeated Instructions
___Graphic Organizers
___Visual Modifications
___Sign Language Interpreter
___Small Group Instruction
___Computer/Word Processor
___Braille/Enlarged Print
___Grading
___CCTV (Visually Impaired)
___Amplification System
___Modified Assignments
___Alternative Materials
___Read Aloud
___Use of portfolios
___Audio Tapes
___Preferential Seating
___Video Cassette
___Cranmer-Abacus
___Magnification Devices
___Translation
___Demonstration Teaching
___Students Marks in Test Booklets ___Study Guides
___Multiple Test Session
___Testing in Separate Room
___One Test Item per Page
___Augmentative Communication Device/Assistive Technology (___________________________)
___Other:_________________________________________________________________________
Related Services/Therapies:
____ Student did not receive related services/therapies during high school
____ Student did receive related services/therapies during high school (If checked, please complete
Attachment 1: Related Services Exit Summary.)
Teacher Reflections Regarding Student’s Overall Academic Ability, Motivation, Self-Determination,
Socio-Emotional Adjustment, and Communication Skills:
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
Attach a copy of the student’s transcript to document credits earned, course of study, and grades earned.
Additional information about this student will be provided, given a signed record release, by contacting:
Name:_________________________________________________________________________________________
Address:_______________________________________________________________________________________
Telephone:___________________ Fax:_______________________ Email:_________________________________
Completed by:____________________________________ Position:_____________________________________
Date prepared:____________________________________ Date Given to Student:__________________________
Post-Secondary Plans/Recommendations:
Area
Employment:
Post-School Goal for Employment
________________________________________________________________________________________
Recommendations
1.____________________________________________________________________________________
2.____________________________________________________________________________________
3.____________________________________________________________________________________
____________________________________________________________________________________________________________________________________
Area
Post-Secondary
Education/Training:
Post-School Goal for Education/Training
Recommendations
1.____________________________________________________________________________________
2.____________________________________________________________________________________
3._____________________________________________________________________________________
Area
Independent Living:
Post-School Goal for Independent Living
Recommendations
1._____________________________________________________________________________________
2._____________________________________________________________________________________
3._____________________________________________________________________________________
CECAS Information
(back to top)
Table of Contents
Part C to B Workflow Chart (Preschool)
CECAS Snapshots of Part C to B for Special Ed. Screen
Initial Placement Workflow Chart
Directions for Entering an Initial Referral on the Special Ed. Screen
CECAS Snapshots of explanation of each section of Special Ed. Screen
CECAS Snapshots of Initial Referral on Special Ed. Screen
Reevaluation Workflow Chart
Annual Review Workflow Chart
IEP DEC 4 Quick Start Guide
Active Student Exit Workflow Chart
Additional Training Documents (on-line only) https://www.nccecas.org/training/trainingdownloads.html
Entering an Initial Referral/Placement on the
Special Ed Screen in CECAS
Conduct a State Wide Search
1. Complete the Child Demographics screen and click the Save button
2. Navigate to the Special Ed screen
3. Enter General data on the Special Ed screen
a. Select Case Manager
b. Select Attending School----If student is PreK or attends private or home
school, select your (LEA) school as Attending School and select a
“Placement Type”
c. Enter the Begin Date ----The first day the child attended this school, or
for referrals from Part C to B, use the day you are informed of the child
(whichever is earlier)
d. Select Grade
e. Click the Save button----Status will be “Pending”
4. Enter Referral Data on Special Ed Screen
a. Enter Referral Received by School Date (Date referral is received from
team or parent) top of Page 3 of DEC1
b. Enter Referral Determination Date (Signature date of DEC1)
c. Select “Yes” or “No” for Referral for Evaluation
d. Click the Save button----Status will be “Referral in Progress” or “No EC
Services- Referral for Evaluation”
5. Enter Evaluation Data on Special Ed Screen
NOTE: This section can be left blank, if applicable
a. Enter Consent to Eval Date (DEC2)
b. Select Consent to Eval Purpose
c. Select response for Consent to Eval Given
d. Click the Save button ----Status will be “Determining Eligibility” or “No
EC Services- Consent to Eval”
6. Enter Eligibility Data on Special Ed Screen
a. Select Evaluation purpose
b. Enter Eligibility Determination Date (DEC3)
c. Select “Yes” or “No” by “Eligible”
d. Select Primary Disability
e. Click the Save button ----Status will be “Developing Plan” or “No EC
Services- Eligibility”
7. Go to the Plans screens and enter a Plan or document an IEP/DEC4 to
closed/verified
8. Enter Placement Data on the Special Ed Screen
a. Enter Consent for Placement Date (DEC6)
b. Select response for Consent for Placement Given
c. Enter Date under “Initial Placement Date” (DEC5)----If the date differs
from Meeting Date for the DEC4
d. Click the Save button----Status will be “Active” or “No EC Services –
Consent to Placement”
e. Yellow fields are populated AFTER a Plan is entered or a DEC4 is
closed/verified if student is eligible.
PROCEDURES
(back to top)
Table of Contents
Transfer Procedures
Reevaluation Procedures
Annual Review Procedures
Continuum of Services
Extended School Year
Surrogate Parent
Summer Testing
Transitions
Occupational Course of Study
Vocational Rehabilitation
MCS E.C. DEPARTMENT
PROCEDURES FOR PROCESSING TRANSFER
STUDENTS
E.C. FACILITATOR INITIALLY HANDLES ALL TRANSFER RECORDS UNTIL A
CASE MANAGER IS ASSIGNED FOR STUDENT
STUDENT MUST HAVE A CURRENT IEP IN ORDER TO BE SERVED
FAX COPIES ARE NOT LEGAL DOCUMENTS – MUST OBTAIN HARD COPY
#1. STUDENT TRANSFERS FROM SCHOOL ‘A’ TO SCHOOL ‘B’ IN MOORE CO.
A. The RECEIVING SCHOOL’S FACILITATOR completes the
EC Data Sheet showing date student arrived @ School “B”
B. Facilitator, sends EC Data Sheet to EC Compliance/Data Manager at the Ed. Center
#2. STUDENT WITHDRAWS FROM MOORE COUNTY SCHOOLS
moves (including home school, charter school), drops out or deceased
Case Manager sends DATA SHEET to the EC Compliance/Data Manager at the Ed.
Center.
#3. North Carolina Student transfers TO Moore County FROM another LEA in NC
(Academy of Moore & STARS are processed here)
A. Student’s records arrive complete with current IEP, psychological, documentation of
eligibility as E.C. student and consent to place.
a. A.S.A.P. – School Facilitator sends an EC Data Sheet to Data Manager at the Ed.
Center to have “pending primary” set in CECAS.
b. IEP team reviews current IEP and addresses any changes via an addendum
meeting.
c. Student’s Case Manager will update student record in CECAS including
entering the current IEP or addendum IEP and close/verifying
d. Case Manager sends to Compliance/E.C.Data Manager:
EC Data Sheet
B. Student’s records arrive with incomplete documentation, BUT does have a current IEP
( DEC 4 can be in CECAS or a hard copy )
a. A.S.A.P. - Facilitator send an EC Data Sheet to Data Manager at the Ed. Center to
have “pending primary” set in CECAS.
b. Records should be reviewed for compliance and an immediate attempt is made to
secure the required documents.
c. An IEP Team meeting must be held within a reasonable amount of time to review
the IEP.
d. An eligibility ( DEC 1 – REFERRAL ) meeting may need to be held to begin
eligibility documentation if additional required documentation is not available
from previous LEA.
e. Eligibility established via previous LEA documentation or new Referral Process ,
IEP is entered into CECAS by Case Manager
f. EC Data Sheet is sent to EC Compliance/Data Manager
#4. STUDENT TRANSFERS FROM OUT OF STATE
a. School Facilitator or case manger conducts a Statewide Search in case this
student is a re-entry into North Carolina. If student is in CECAS please contact
our EC Compliance/Data Manger at the Ed. Center.
b. Student is to be initialized in CECAS with Demographics and Special Ed screens
completed based on information available at the time.
c. Records are complete –
1. IEP Team MUST meet in order to review the current IEP and North
Carolina Eligibility status. If the IEP team determines testing is current
and relevant, the team can use the DEC 1 as a review and on page 4
select option 2. CW Data sheet is sent to EC Compliance/Data Manager.
IEP is entered into CECAS Form DEC 4 by Case Manager and
closed/verified. If this option is used this is the new eligibility date and
will set a new three year clock.
2. If the team determines testing is no longer relevant then the team will
complete a DEC 1 and DEC 2. The team can serve based on the current
goals while testing occurs. When testing is complete an eligibility
meeting will be held.
d. Records are incomplete - IEP Team meeting is held to review IEP, and
complete a DEC 1 Referral in order to evaluate the student’s EC eligibility under
NC Guidelines. This begins the 90 day timeline. Comparable services must be
given during this time.
1. Eligibility under NC Guidelines is established at IEP Team eligibility meeting.
DEC 3 must be completed and signed.
2. IEP is developed or amended and a DEC 5 & 6 are completed.
3. IEP is entered into CECAS by case manager and closed/verified
e. Data Sheet completed and sent to EC Compliance/Data Manager @ the Ed. Center.
8/06/09
Three Year Reevaluation Procedures
It is the policy of Moore County schools to start all three year reevaluation procedures at least 4 months
(120 days) in advance of it needing to be complete. This gives ample time for the team to gather data as
necessary and make decisions.
Annual Review
The process for completing the annual review should start no less than 45 days before the expiration of
the current IEP to allow ample time for the meeting to occur. This allows time for the scheduling of a
second meeting if needed and still meet legal requirements.
Continuum of Services Information
The law states that a school day is from bell to bell. Based on this all Moore County schools have a
seven hour day. Based on the percentage of time for services this is the breakdown for each continuum
that they can be removed from non-disabled peers.
Regular – up to 84 minutes
Resource – 85 to 252 minutes (4 hours and 12 mins.)
Separate - 253 min. or more
Required forms for Initial Placement and Reevaluation
Initial Placement
Invitation to Conference
DEC 3 Worksheet
Eligibility Determination DEC 3
DEC 4
DEC 5
DEC 6
DEC 9
DEC 10
C/W Data Sheet
Minutes
Revaluation if no Evaluation Conducted
Invitation to Conference
Parent Questionnaire
Student Questionnaire
Teacher Questionnaire
Student Record Review Form
DEC 7
Eligibility Determination DEC 3
DEC 4 (if needed)
DEC 5
Minutes
C/W Data Sheet
Reevaluation Determination with Formal/Informal Data Collection
Invitation to Conference
Parent Questionnaire
Student Questionnaire
Teacher Questionnaire
Student Record Review Form
DEC 7
DEC 2
DEC 5
Minutes
Reevaluation Meeting
Invitation to Conference
DEC 3 Worksheet
Eligibility Determination DEC 3
DEC 4 (for addendum purposes)
DEC 5
Minutes
C/W Data Sheet
Surrogate Parent Information
When is a surrogate parent needed?
The child’s parents or guardian are not known.
The child is a ward of the state. (Termination of parental rights has taken place.)
Only after the school has made reasonable efforts to contact the parent and cannot.
Who can be a surrogate parent?
Cannot be an officer, agent or employee of the school district, the State Education Department or
the agency which is involved in the education or care of the child.
May be an employee of a nonpublic agency that only provides non-educational care for the child.
May be the foster parent of a child.
NOTE: A surrogate parent must be trained!! This training is provided by the EC Department of
Moore County Schools.
Training normally takes one hour
You must allow at least 10 days prior to the desired meeting date for a surrogate to be appointed
and trained.
Failure to provide adequate advance notice may result in the delay of the meeting and ultimately,
a file being out of compliance!
Summer Testing Information
Moore County Schools does offer a limited amount of summer testing during the month of June. These
referrals must be on students who you feel certain the parent will bring in for testing and have a current,
working phone number. A behavioral and emotional evaluation cannot be completed during the
summer.
What information must be provided for summer testing to occur?
Initial Referral
I.
II.
III.
IV.
V.
VI.
VII.
Summer testing request form
SST paperwork
Referral
Testing information and grades from cumulative folder
Final report card
Vision and hearing screen
Permission to test
Re-evaluations
1.
2.
3.
4.
5.
6.
7.
Summer testing request form
DEC 7
Permission to test
Record review
Vision and hearing screen
Previous psychological report
Final report card
Summer Testing Request Form
School:______________________________________________________
Person Completing Request:_____________________________________________________
Summer Phone Number for Person Completing Request:_____________________________
Student Name:_________________________________________________________________
Date of Birth:__________________________________________________________________
Grade:_______________________________________________________________________
Parent Name:_________________________________________________________________
Home Address:________________________________________________________________
Parent Telephone Number: Home________________________Work___________________
Please attach a copy of the following for initial referrals:
VIII. SST paperwork
IX. Referral
X. Testing information and grades from cumulative folder
XI. Final report card
XII. Vision and hearing screen
XIII. Permission to test
Please attach a copy of the following for re-evaluations:
8. DEC 7
9. Permission to test
10. Record Review
11. Vision and hearing screen
12. Previous psychological report
13. Final report card
INFORMATION MUST BE RECEIVED BY PAM CARTER BY JUNE 11, 2008.
Student Services Office Use Only
Parent contacts:______________________________________________________________________
____________________________________________________________________________________
Evaluation Scheduled for:_____________________________________________________________
Transition Information
The following is additional information for use in transitions with all students.
Transition Assessments
One of the many things that the state and federal government is looking at
in the continuous improvements audits in regard to transition planning is:
“Evidence that the measurable post-secondary goals are based on ageappropriate transition assessments.”
This can be easily documented on the first page of the Transition Plan in
the IEP. In section “A” “Indicate how information was attained in the
development of post-school goals and transition activities.” Check the
appropriate line and then on the right hand side write out what assessment
was used.
Interest Skills and Inventories—would be paper/pencil questionnaires or
websites with career inventories.
Situational Assessments—would be when a student tries out a job (i.e.—
OCS students in the community).
Formal Assessments—would be a work assessment completed by LCI or VR.
Rating Scales—would be an assessment based on a scale.
Interviews—would be asking the students questions, re: post-school goals.
Enclosed are examples of different assessments that teachers can pull from
to fulfill this requirement. A student should complete the assessment prior
to the IEP meeting. It can be done as part of a class as well (i.e.—many
assessments are used in OCS classes), but teachers need to remember to
note them on the Transition Plan. You may use other assessments that you
find and think are appropriate. This information can be a starting point.
If you have any questions about Transition Assessments contact:
Kassia Stubbs, Compliance and Transition Coordinator—947-2342
email—kstubbs@ncmcs.org
Career Interest Inventory
Circle the letter in front of each statement that best describes you. Circle as many as you wish, but
try to limit your choices to the statements you feel strongest about.
(A)
(B)
(C)
(D)
(E)
(F)
I like playing sports
I like solving puzzles.
I like being the leader in a group.
I like to talk.
I enjoy drawing pictures.
I ask a lot of questions.
(A) I like to spend my free time outdoors.
(B) Math is my favorite subject.
(C) When I grow up I want to be my own boss.
(D) I enjoy being part of a group and solving problems
(E) I would rather be in a play than watch one.
(F) Science is my favorite subject in school.
(A) I like to make things out of wood, paper,
metal, sloth, etc.
(B) I like to make lists of things I need to do.
(C) When I grow up, I want to run my own
business.
(D) I enjoy helping other people.
(E) I enjoy making up stories.
(F) I can sit and watch birds at a bird feeder
for a long time.
(A) I like working with plants and animals
(B) My handwriting is clear and neat.
(C) I would enjoy being the mayor of my hometown.
(D) I like putting my feelings into writing.
(E) I would rather work by myself than in a group.
(F) I like to solve complicated puzzles and problems.
(A) I like to build models.
(B) I enjoy working on a computer.
(C) I enjoy doing group projects in school when
(A) I like to work with tools.
(B) I feel better when my room is neat and tidy.
(C) I am happier playing in a group than by myself.
I’m the leader.
(D) I enjoy meeting new people and making new friends.
(E) Music is my favorite subject.
(F) I would enjoy traveling to faraway places to learn
how people live.
(D) I’m never shy about telling my friends what
I think.
(E) I would enjoy decorating my house.
(F) I enjoy reading the encyclopedia.
Count the number of letters you circled and record the results in the blanks below.
A________
B________
C________
D________
E________
F________
If you have a score of four or more next to any one letter, you might be interested in learning more about the
careers similar to those in the clusters listed below. If you did not score four in any category, your interests are
still developing.
A
Coach
Mechanic
Farmer
Forester
Veterinarian
Plumber
Electrician
Pilot
Carpenter
B
Computer programmer
Computer operator
Accountant
Secretary
Banker
Editor
Banker
Editor
C
Salesperson
Business owner
Business manager
Lawyer
Politician
Military officer
School principal
D
Teacher
Social worker
Doctor
Nurse
Paramedic
Newspaper writer
Advertising agent
TV/Radio reporter
E
Actor/Actress
Artist
Fashion designer
Architect
Musician
Photographer
F
College professor
Researcher
Archaeologist
Anthropologist
Engineer
Detective
Student/Parent Questionnaire
The following questions will help you (and your parents) think about your preferences
and interests as well as services you will need after leaving high school. School staff will
use your answers to assist you in planning and locating services that match your future
plans. Your parent/guardian can help you answer these questions.
1. Please give your age, grade level, and date of graduation:
______Age
______Grade
_______Date of Graduation
2. What do you plan to do after you leave school?
3. What are your preferences and interests in moving into the adult world?
4. What do you want for yourself during the next year after leaving school:
in 5 years? 10 years?
Employment:
Education:
Living Arrangements:
5. What most concerns you about your future?
6. Are you presently in contact with any agencies that will or may be involved with you
after graduation? Do you plan to make or maintain contact?
7. Do you feel you can advocate for yourself when you graduate from high school, or
does your parent/guardian or someone else need to advocate for you on your behalf?
8. With whom and where would you like to live?
9. Where would you like to work? What kind of work would you like to do?
10. What recreational/leisure facilities have you used? Which ones would you like to
use when you graduate from high school?
11. In what areas do you feel that you will need assistance to plan for when you leave
school?
_____Vocational
_____Work training
_____Residential placement
_____Social relationships
_____Transportation
_____Financial
_____Recreation/leisure
_____Independent living
Student Name:___________________________________ Date Completed:__________
Am I ready for College Inventory
Completed by : ____________________________________________
_____________
Date:
Before making a commitment to college education, you should take the time to consider
your preparedness for becoming a full-time, part-time or distance education student.
Consider the following questions.
Place the appropriate number (1, 2, or 3) in the box next to each question.
(1 = I have completed this step; 2 = I have started this step-it needs more work; 3 = I
have not started/ thought about this step; I need help).
I have identified my short-term and long-term goals.
I have identified a career choice.
I know the specific credentials/ certificates/ degree I will need in
order to qualify for a particular job.
I know which course, certificate or diploma will help me succeed
in my chosen field.
I know whether or not my chosen career requires a college
education or some other type of training.
I can clearly explain why I have chosen to pursue a college
education.
I have considered other options for furthering my education?
I know the basic entrance requirements for being admitted into
the college/ training program of my choice.
I am prepared for College?
I know how college classes and study skills differ from high
school classes and study skills.
I have passed the classes necessary to gain for college.
I have taken the PSAT/SAT or entrance exam for college
My grades reflect that I am academically prepared for college?
I know how to study
I am financially prepared to support myself while pursuing my
studies?
I have completed the FAFSA.
I know what support services are available to me at the college
or training program of my choice?
THINGS I NEED TO KNOW ABOUT MYSELF TO BE
SUCCESSFUL
Learning Style: (visual, hands on, listening, etc.
Achievements: (What have you done that you are proud of?)
Learning Strengths: (Do you have a good memory?, Are you organized?, Can
you problem solve?, etc.)
School Work:
What subjects do you do well?
What subjects do you have difficulty with?
Special Needs: (What helps you to learn better?)
Work Habits:
Problem Solving Skills: (How do you handle difficult situations?)
What is important to me?
What are my plans for the future?
About Me
(To be completed by student prior to IEP Team Meeting
1. In school, it’s easy for me to . . .
2. In school, it’s difficult for me to . . .
3. My special talents are . . .
4. I’m really interested in . . .
5. I learn best when . . .
6. Accommodations I need and will use are . . .
7. I’m proud of myself because . . .
Getting to Know You
Please complete the following sentences. There are no right or wrong answers.
1. During the summers I most enjoy ________________________________________.
2. I wish I could _______________________________________________________.
3. What I like to do most is _______________________________________________.
4. The thing I enjoy best about school is _____________________________________.
5. I am happiest when ___________________________________________________.
6. My favorite television program is ________________________________________.
7. I learn best when _____________________________________________________.
8. My favorite sports are _________________________________________________.
9. One thing I do well is _________________________________________________.
10. One thing I would like to do better is ____________________________________.
11. I dislike school when ________________________________________________.
12. When I grow up I hope to be __________________________________________.
Name__________________________________
Date______________________
Student Interview for Transition Planning
Italics indicate the corresponding area on the IEP
Name:_____________________________________Date:__________________
School:___________________________________________________________
Interests, Preferences and Strengths:
Post-Secondary Living (Independent Living)
I plan to move away from home when I am __________(age).
I plan to live in ____a large city, ____a small town, ____country (rural area)
If you have a particular place in mind, list it here:________________________
Places I will go in my community:
____banks
____movie theaters
____restaurants
____work
____friends’ houses ____video rental store
____grocery stores ____parks/recreational spots
____night spots
____employment agency
____discount stores ____community agency
____public library
____shopping malls
____church
____golf courses
____vote
____other________
When I live on my own, I plan to live in:
____an apartment
____a condominium
____a mobile home
____a house
____dormitory
____other_________
I want to live:
____alone
____with parents
____with someone to assist me
____with my husband/wife
____with one or more roommate(s)
To reach this goal, I will need to:_____________________________________
These are the skills which I currently demonstrate at home:
____cleaning
____cooking
____grocery shopping
____laundry
____checking account
____scheduling appointments
____debit card
____savings account
____taking medications
____budgeting
____clothes shopping
____cell phone
____home repairs
____paying bills
____other______________
____computer use
____video games
______________________
When I live on my own, I plan to get around by:
____driving my own car
____riding my bike
____riding a motorcycle
____riding with a relative
____riding public transportation
____riding with friends
I currently have a: ____driver’s permit
____driver’s license
____walking
____other
____neither
To reach this goal, I will need to:_____________________________________
Post-Secondary Training/Education
Right after high school, I plan to:
____go right to work full-time
____receive on-the-job training
____work part-time
____learn a hands-on trade
____attend a technical/trade school
____join the military
____attend a 2-year college
____attend a 4-year college/university
To reach this goal, I will need to:____________________________________
Post-Secondary Working (Employment)
I have earned money with the following part-time jobs (mowing lawns, babysitting, farm work,
etc.___________________________________________
I am interested in these job areas:_______________________________________
After I have completed my education (high school and past high school), the career I would like to
have is:__________________________________________
Employability Skills (Working Results)
Please indicate your use of these skills: 1=Rarely, 2=Sometimes, 3=Always
____punctuality ____attendance ____accountability ____follows directions
____stays on task ____completes tasks ____accepts constructive criticism
____works independently ____works as part of a team
To improve my job skills and increase opportunities for employment, I will:
Attend college: ____2 year
____4 year
Become an apprentice____
____Look for a job coach
Seek employment that offers on the-job training _____
Enroll in workshops at a community college_____
Course of Study
To be prepared to live and work on my own in the future, it would be beneficial for me to take
the following classes and be involved in these activities:
If appropriate, which of these adult service providers will you use?
____Vocational Rehabilitation
____WIA (Workforce Investment Act)
____Case Management
Recreation and Leisure (Independent Living)
After I graduate from high school, these are the things that I will do in my free time:
____bowling
____dining out
____golfing
____dating
____camping
____traveling
____volunteering
____fishing
____hunting
____partying
____skiing
____dancing
____watching IV
____reading
____cooking
____sewing
____crafts
____woodworking
____sporting events
____visiting friends
____talking on phone
____going to movies
____renting videos
____exercising regularly
____driving around
____playing sports
____joining a health club
____listening to music
____playing video games
____use computer
____skateboarding
____horseback riding
____other____________________
other______________________
To reach these goals, I will need to (get my driver’s license, earn spending money, take craft
instruction, etc.):_________________________________
Student Mapping Form
Student Name: __________________________________
Review Date: _______________________
_______________________
_______________________
Initial Date: _______
_________________________
_________________________
_________________________
Parent(s) Guardian Name: _____________________________________________
Anticipated Date of Graduation: ________________________________________
What are your dreams for your child? List them no matter how big they are.
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
What are your fears for your child?
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
What are your child’s needs?
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
List at least three things that you would like your child to work on during the the time
he or she is in high school.
___________________________________________________________________
____________________________________________________________________
___________________________________________________________________
What one thing could we teach your child at school that would make life easier at
home? ____________________________________________________________
__________________________________________________________________
What do you see as Post-school goals for your child in each of the following areas?
Employment:
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
Education: ___________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
Residential: __________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
Recreation: __________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
Go back over your comments? Are they functional, meaningful, a choice of your
child’s, useful in a variety of settings?
Used by permission of Shelby City Schools/Cleveland County Schools (revised 2001)
Modified from information received at the Western Region Transition Services
Institute in Charlotte, March 3-5, 1993.
Date_________________
Intense Needs Planning Survey
Student Name: ________________________
School: ______________________________
Completion Dates
Anticipated Graduation Date: _________
Teacher: __________________________
Completed By
The following questions will be used to assist in transition planning activities and to determine postschool goals.
Employment/Training:
This young person will likely work in:
Full time regular job (competitive employment)
Part time regular job (competitive employment)
A job that has support and is supervised, full or part time (supported employment)
Volunteer Work
Productive activities based on interests with habilitative supports (Please describe:
_________________________________________________________________________
_________________________________________________________________________
How many hours a week do you think this young person’s stamina and endurance would allow him or
her to work:
_____________________________________________________________________________
List this young person’s vocational interests:
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
What types of vocationally-related skills does this young person need to develop?
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
What types of supports would this young person need to engage in employment or productive activities
in the community?
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
Date____________________
Education:
Future education/therapy for this young person should include (check all that apply):
Vocational Training at a Vocational School
On-the-Job Training
Continuing Education classes at the Community College in an area of interest
Compensatory Education classes at the Community College
Habilitation training
Physical Therapy
Speech Therapy
Occupational Therapy
List his young person’s educational strengths:
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
What types of academic skills would you like to see this young person develop?
1. _________________________________________________________________________
2. _________________________________________________________________________
3. _________________________________________________________________________
4. _________________________________________________________________________
What types of supports would this young person need to engage in educational activities after
graduation?
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
Independent Living:
After graduation this young person will likely live:
With a roommate in a house or an apartment
In a supervised living situation (group home, supervised apartment)
With parents
With other family members
Other: ____________________________________
List this young person’s independent living skill strengths:
1. _________________________________________________________________________
2. _________________________________________________________________________
3. _________________________________________________________________________
4. _________________________________________________________________________
Date____________________
Participation in household chores/tasks:
Household Chores/Tasks
Performs
Now
Could
Perform
What types of daily living or adult living skills would you like to see this young person develop?
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
What types of supports would this young person need to be more independent in their place of
residence?
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
What concerns/fears do you have about this young person’s living arrangements in the future?
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
Recreation and Leisure:
When this young person graduates, I hope he/she is involved in (check all that apply):
Independent recreational activities
Activities with friends
Organized recreational activities (club, team sports)
Classes (to develop hobbies, and explore areas of interest)
Supported and supervised recreational activities
Other: _________________________________________
Date______________________
Indicate the student’s present and potential recreational and leisure interests:
Recreation and Leisure Interests
Present
Future
What types of supports would this young person need to engage in recreation and leisure activities in
the community?
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
When I think of the free time this young person will have after graduation, I am afraid that:
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
Transportation:
When this young person graduates, he/she will (check all that apply):
Receive transportation support from family
Receive transportation support from friends
Participate in ride-sharing
Participate in a special transportation program
Other: _________________________________
What types of supports would this young person need to have adequate transportation after graduation?
1. _________________________________________________________________________
2. _________________________________________________________________________
3. _________________________________________________________________________
Date______________________
Self-Determination
What types of choices does this young person make on a regular basis?
____ Food
____ Community Outings
____ Schedule
____ Clothing
____ Music
____ Personal Belongings
____ Leisure Activities
____ Friends
____ Purchases
Medical/Health Issues:
Please describe any medical/health issues this young person has which may impact transition from
school to adult life:
1.
2.
3.
4.
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
Personal Preferences:
1.
Indicate this young person’s preference or dislike of the following environmental characteristics
by putting a check for preference and an X for dislike:
___ Noisy
___ Brightly Lit
___ Solitary
___ Interactive with others
2.
___ Having conversations
___ Joking/Laughing
___ Interacting with peers
___ Interacting with special
friends
___ Interacting with caregivers ___Listening to conversations
___ Making eye contact
___ Answering questions
Indicate this young person’s preference or dislike for the following types of community activities
by putting a check for preference and an X for dislike:
___ Shopping
___ Church
___ Festivals
4.
____ Dimly Lit
____ Small group of people
____ Active
Indicate this young person’s preference or dislike for the following types of social interactions by
putting a check for preference and an X for dislike:
___ Being alone
3.
____ Quiet
____ Large groups of people
____ Stimulating in smells
___ Eating Out (Formal)
___ Movies
___ Choral events/concerts
___ Eating Out (Informal)
___YMCA
___ Parties
Indicate the natural supports this young person will have after graduation.
1. _________________________________________________________________________
2. _________________________________________________________________________
3. _________________________________________________________________________
Strengths & Skills Inventory
Name:__________________________________Date:____________
How well does each statement describe you?
Very Somewhat
much
like me
like me
Not
like
me
Very
unlike
me
I like to read.
I can talk easily in a group.
I enjoy playing a musical
instrument.
I like sports.
Math is easy for me.
I’m good at fixing things
around the house.
I like to sew.
It is easy for me to listen
while others speak.
I enjoy cooking.
I like to write.
I make friends easily.
I like to paint (or do other
kinds of art).
I would like to be a class
officer or a leader of a club.
I’m good at putting things
together that come in parts.
I get good grades in school.
I like to work on mechanical
things.
I like caring for animals and
having pets.
I enjoy helping others.
I like science.
Contributed by Nancy Jones
Who Makes the Choices
Student-led IEPs
SELF-DETERMINATION CHECKLIST
Student Self-Assessment
Student Name: ____________________________________ Date: _________
Directions: Use the scale below to answer the following questions. There are no wrong
answers. In the column titled “Level of Assistance” circle the choice that best describes
how you accomplish each item.
5 = Always
4 = Most of the time
3 = Sometimes
2 = Rarely
1 = Never
Score
1. Do you tell teachers, staff, and family what
you like to do?
Level of Assistance
(circle one)
Independent
Help from family/friends
Help from staff
2. Do you make choices regarding supports,
accommodations, and activities you want or
need?
Independent
Help from family/friends
Help from staff
3. Can you describe your disability?
Independent
Help from family/friends
Help from staff
4. Do you ask for help when you need it?
Independent
Help from family/friends
Help from staff
5. Do you tell paid and unpaid supports how you
want them to help you?
Independent
Help from family/friends
Help from staff
6. Can you describe your strengths?
Independent
Help from family/friends
Help from staff
7. Can you describe your rights under IDEA
and ADA?
Independent
Help from family/friends
Help from staff
8. Do you have a circle of support, including
family and friends, who help you accomplish the
things you want?
Independent
Help from family/friends
Help from staff
9. Do you work with your IEP manager about
developing and managing your IEP?
Independent
Help from family/friends
Help from staff
10. Can you keep track of how you’re working
toward the IEP goals?
Independent
Help from family/friends
Help from staff
TOTAL SCORE
What are you doing better now than you were doing the last time you assessed
your self-determination skills? ________________________________________
________________________________________________________________
________________________________________________________________
________________________________________________________________
What do you feel like you still need to practice? _________________________
________________________________________________________________
________________________________________________________________
How can the people around you (friends, teachers, staff, family) help you to build
your self-determination skills? _______________________________________
________________________________________________________________
________________________________________________________________
Student Dream Sheet
Student Name: _____________________________
School: ___________________________________
Initial Date:___________________
Teacher: ______________________
Review Dates: _____________________________
_____________________________
_____________________________
_____________________________
_____________________________
_____________________________
Anticipated Date of Graduation: _____________________________________
The following questions will be used to assist in transition planning activities and to determine postschool goals.
1. Where do you want to live after graduation? ______________________________________
____________________________________________________________________________
What kind of housing?__________________________________________________________
2. How do you intend to continue learning after graduation? ____________________________
_____________________________________________________________________________
_____________________________________________________________________________
What types of things do you want to learn after graduation? _____________________________
_____________________________________________________________________________
_____________________________________________________________________________
Where do you want this learning to occur? ___________________________________________
______________________________________________________________________________
______________________________________________________________________________
3. What kind of job do you want now? ______________________________________________
______________________________________________________________________________
______________________________________________________________________________
4. What kind of job do you want when you graduate? __________________________________
________________________________________________________________________________
____________________________________________________________________________
5. Where do you want to work? ___________________________________________________
______________________________________________________________________________
6. What type of work schedule do you want? _________________________________________
______________________________________________________________________________
7. What type of pay and benefits do you want from your future job? ______________________
______________________________________________________________________________
______________________________________________________________________________
(continued)
Student Dream Sheet (continued)
8. What types of chores do you do at home? _________________________________________
______________________________________________________________________________
______________________________________________________________________________
________________________________________________________________________________
____________________________________________________________________________
9. What equipment/tools can you use? ______________________________________________
______________________________________________________________________________
______________________________________________________________________________
10. Do you have any significant medical problems that need to be considered when determining
post-school goals? ______________________________________________________________
_____________________________________________________________________________
_____________________________________________________________________________
11. What choices do you make now? _______________________________________________
_____________________________________________________________________________
_____________________________________________________________________________
12. What choices are made for you that you would like to make for yourself? _______________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
13. What kind of transportation will you use after graduation? ___________________________
________________________________________________________________________________
____________________________________________________________________________
14. What do you do for fun now? __________________________________________________
______________________________________________________________________________
______________________________________________________________________________
15. What would you like to do for fun in the future?___________________________________
_____________________________________________________________________________
_____________________________________________________________________________
Reprinted with permission from Cleveland County Schools (Revised 2003)
Student IEP Input Form
Date:____________ Name:________________________________________
Grade Next Year:__________
I am good at:
Speech
Science
Math
Reading
Writing
Social Studies
Spelling
Language
Gym
I need extra help with:
Science
Math
Writing
Speech
Social Studies
Language
Gym
Reading
Spelling
When I have free time, I really like to:
It helps me when the teacher:
It helps me when I: (circle as many as you want)
Sit near the front
have a shorter spelling list
have a teacher repeat the directions
use a math chart
have highlighted directions
have things read to me
use a calculator
use a student dictionary
have choices for test questions
have work sheets have help organize notebook
have extra time to complete my work
I work best when I work:
with a partner
by myself
in a small group
I am good at:
telling stories
typing/keyboarding
drawing
being a helper
reading stories
remembering
numbers
counting
public speaking
It’s hard for me to: tell how I feel
do basic computer skills
color
wait for my turn
write stories
understand a story
cut with scissors
make friends
I love to:
play outside
use the computer
look at books
play sports
watch television
do word puzzles
make friends
Who Makes the Choices?
Student-led IEPS
cook/eat
(Contributed by Karen L. Hinds via a teacher in Chicago, IL
. . . MORE EXAMPLES OF TRANSITION ACTIVITIES
Employment
Off-Campus Vocational Experiences (e.g. job shadowing, paid/non-paid community-based
training, internships)
On-Campus Vocational Experiences (e.g. school-based enterprise, on-campus jobs)
Participate in Career Training for Exceptional Children to provide the opportunity for offcampus or on-campus vocational training
Participate in Occupational Preparation classes through the Occupational Course of Study
Taking and completing Career/Technical Education courses in a pathway based on interests.
WIA related activities (i.e. work xperience, summer employment, leadership training,
mentoring, etc.
Participate in work adjustment activities on the school campus funded by VR.
Referral to Vocational Rehabilitation for employment related services (job coaching,
vocational counseling, vocational assessment, supported employment)
Referral to the local management entity (mental health) for case management services and
other possible funding for employment-related services (e.g. CAP-MR)
Establishment of case management services for long-term follow-up through Medicaid
reimbursement for supported employment.
Receive training in job-seeking skills
Receive training in job maintenance skills
Receive training in employment related social skills
Receive vocational training in the skills required for a specific vocational area (e.g. learning
clerical skills needed to operate office equipment.)
Receive work behavior and work habit training (e.g. soft skills such as staying on time,
accepting feedback from a supervisor, self-monitoring/evaluation)
Registration at Employment Security Commission (Job Link Centers)
Vocational evaluation/assessment (e.g. interest inventories, aptitude testing, etc.)
Observe Situational assessment.
Assistance in understanding the results of vocational evaluations/assessments
Assistance in understanding work-related forms/paperwork
Training in academic sills related to employment settings
Learn and practice self-advocacy skills
Seek career counseling
Establishment of natural supports on the job site
Receive training in employment related laws and legislation related to persons with
disabilities
Receive training in employment goal-setting
Receive assistance in completing employment-related forms
PASS or IRWE development and approval (SSI work incentive programs)
Develop transportation arrangements for vocational training or employment
Participate in volunteer or community-service activities
Develop a resume
Develop and present a career portfolio
. . . EXAMPLES OF TRANSITION ACTIVITIES (cont.)
Post-Secondary Education/Training
Referral to Vocational Rehabilitation for financial assistance
Enrollment in and completion of a high school course of study
Obtaining a high school diploma
Obtain tutoring services
Determine and receive classroom accommodations, modifications and supports
Participate in career development activities for the purpose of choosing a college major
or post-secondary vocational training program (vocational assessment, job shadowing,
paid employment, volunteering)
Obtain assistive technology to support learning needs
Research appropriate sources of financial assistance for post-secondary
education/training
Obtain assistance with application/financial aid forms
Obtain assistance with selecting an educational institution
Obtain assistance in understanding the criteria for admission and deadlines for
application
Contact the student support services personnel at the college and learn about services for
students with special needs
Effectively express education, physical, sensory and medical limitations and needs
Obtain information about civil rights, confidentiality, and personal rights as they relate
to post-secondary education/training
Receive training in budgeting skills
Participate in remedial classes in academic areas
Participate in social skill training relevant to college campus life
Obtain information about residential options for post-secondary education/training
Visit campus(es) and/or participation in prospective student weekends
Participate in pre-college summer sessions
Participate in summer camps on campus
Arrange transportation to post-secondary education/training
Prepare for college admission tests
Take the PSAT
Assist in arranging accommodations/modifications for college/university admission tests
Receive self-advocacy training
Receive study skills training (e.g. note-taking, outlining, etc.
Obtain test-taking skills training
Complete the enrollment process for compensatory education classes or adult basic
education classes
Take a Huskins course
Obtain college credits prior to high school graduation through participation in the dualenrollment college
Use the internet to investigate and determine appropriate post-secondary
education/training matches based on interests and needs
Participate in habilitative training (e.g. community access, communication, social skills, mobility
skills, etc.) after school with CAP-MR funding
Participate in cooking/nutrition classes through the local Agriculture Extension Agency
Participate in a college-mentoring program
. . . Examples of Transition Activities (cont.)
Independent Living
Seek assistance in understanding social security benefits
Receive training in clothing care
Receive training in household maintenance (e.g. cleaning, simple repairs, contacting a
repairman, etc.)
Receive cooking skills training
Learn and practice menu planning
Receive training in money-related skills (e.g. opening a bank account and using banking
services, budgeting, comparison shopping, checkbook management, use of coupons,
credit and loans, purchasing major items, paying bills, etc.)
Develop yard work skills
Receive first aid training
Receive training in obtaining medical/health care
Receive training in budgeting skills
Learn how to open a savings account
Participate in community service utilization training
Participate in telephone usage training
Tour residential living options
Learn how to do a referral to the local management entity (mental health) for assistance
in locating residential placement
Learn about criteria for subsidized housing
Receive training in completing paperwork associated with living arrangements
Participate in community-based classes in a hobby or area of special interest
Develop hobby-specific skills
Evaluate natural supports t determine potential access to community events/activities
Obtain exposure to and training in community recreational activities
Obtain assistance in enrolling/joining community recreational organization
Receive social skill training
Learn how to arrange for a recreational buddy
Receive training in budgeting for recreational/leisure activities
Receive training in how to make and keep friends
Learn how to evaluate personal recreational interests
Participate in school sports
Join a community sports team
Participate in a church-related activity
Administer recreational/leisure assessments and surveys
Join a hobby club
Join the YMCA
Tour community recreation site
Arrange for transportation to community events/activities
TRANSITION—
It’s for EVERY SPECIAL EDUCATOR.
1. A student who has graduated with a certificate CAN be readmitted to pursue a
diploma as long as that student is NOT 22 years old.
2. State monitoring of student involvement in the IEP process will be measured by
BOTH student invitation AND Student attendance. (Indicator 13)
3. Family characteristics and special challenges facing families have significant
influence when developing student vision and post-school goals during transition
planning.
4. To implement IDEA 2004, every special educator should have a knowledge of
transition education.
TRANSITION—
It’s MORE than the OCS—Occupational Course of Study
The preparation of students for life after high school MUST encompass ALL students in ALL
categories or disability. Implementation of the OCS has shifted some focus from other
categories of students, primarily the SED, LD, OHI and the significantly “at risk”. We must
focus on ALL students with disabilities if we are to comply with, and produce the performance
and results expected through implementation of IDEA 2004.
P. O. Box 1180
Carthage, NC 28327
Student ______________________________
Birth Date: ________________
School: ______________________________
Moore County Schools must invite a representative of any agency that is likely to be
responsible for providing or paying for transition services. Parental consent (or student
consent if age 18, age of majority) is required for a representative of any such agency to be
invited.
Please complete the following:
_____ I/We give consent for a representative from ______________________ (agency) be
invited to the Individualized Education Plan (IEP) meeting where transition services will be
discussed.
_________________________________________
____________________
(Parent/Eligible Student Signature)
(Date)
_______ I/We
do not give consent for a representative from ____________________ (agency)
to be invited to the Individualized Education Plan (IEP) meeting where transition services
will be discussed.
_________________________________________
____________________
(Parent/Eligible Student Signature)
(Date)
Please return to:
_______________________________
_______________________________
_______________________________
_______________________________
Student Led IEP—Getting Started
1.
Begin by greeting everyone and stating the purpose of the meeting.
“Welcome to my meeting. Today we are going to plan my program for next year.”
2.
Introduce yourself and others at the meeting.
“My name is ____________________________ and I am a student at ____________________
in _________ grade. I’d like to introduce _______ (names of people at meeting)
OR
“Please introduce yourselves, starting with _________________.”
3.
Review how you have been doing in school.
“Things that have worked well for me this year are
_______________________________________________________________________
______________________________________________________________________.”
“Things that haven’t worked very well for me are
________________________________________________________________________
________________________________________________________________________.”
4. Share data from your goals and objectives, transition services activities, class work, class
credit, attendance or other useful information.
“I have a _____________ (chart, picture, paper) that shows how or what I have been doing.”
5. Participate in discussions.
6. Ask questions.
7. Answer questions.
8. Request input from other participants in the meeting.
“Does anyone want to comment on how my program has been going?”
(Note to student: Ask questions if you don’t understand something that is said.)
9. Identify your post-school goals:
“When I finish high school, I want to _______________________________
______________________________________________________________.”
Any comments or questions?”
10. Identify your goals for this year:
“This year in school and transition activities I want to ________________
______________________________________________________________.”
11. Identify the supports you need to be successful:
“For me to be successful in school and transition planning this year I need to
________________________________________________________
______________________________________________________________.”
“Any comments or questions?”
12. Summarize your goals:
“In summary, my future plans are to______________________________
_____________________________________________________________.”
“For me to make progress toward these goals, I will do these things this year
_____________________________________________________
_____________________________________________________________.”
13. Review support needs and finalize program.
“The things that need to be in my program to help me succeed are _____
____________________________________________________________.”
(Note to student: Discuss differences and agree on final program.
14. Conclude meeting.
“Thank you all for coming to my meeting.”
“This year I am going to work hard to accomplish my goals.”
“I appreciate your help.”
Self-Rating Level of Involvement
Attended
_____ Physically present
_________ Limited
eye contact
_________ Limited responses to questions and/or discussion
Actively Participated
______ Shared the purpose of the meeting
______ Introduced myself
______ Introduced others or asked them to introduce themselves
______Shared how you are doing in school
______Asked others to share about program
Led My IEP
______ Attended
______ All items listed under actively participated
______ Participate in discussions
______ Asked questions
______ Answered questions
______ Identify your post-school goals
______ Identify your goals for this year
______ Summarize your goals
______ Review support needs
______ Finalize program
______ Thank everyone for coming
______ Let them know you appreciate their help.
My IEP
My IEP
My IEP
Welcome to My IEP Meeting!
Here is my welcome and thank you to you for coming to my meeting
Introductions
Here are the names of the people who are at this meeting, and what their role is at this
meeting
Why are we here?
Here’s what an Individualized Education Plan is in my own words
and what we will be doing at this meeting
Created for you by Becky Wilson Hawbaker, Malcolm Price Laboratory School, University of Northern Iowa
My Vision for the Future
After I graduate from high school, this is what I see in my future:
More School? (College? Technical School? Apprenticeship?)
Career Possibilities:
Family Possibilities
(marriage? Children? Near parents/siblings?)
Places I would like to live:
How I will get around—transportation
Things I will do for fun
Created for you by Becky Wilson Hawbaker, Malcolm Price Laboratory School, University of Northern Iowa
Goal #1:
This year’s goal is:
This is the exact wording of my goal from my official IEP
Table of Contents:
a list of the things I have chosen to put in my portfolio to
demonstrate my progress
My Final Evaluation of this goal
1
2
3
I made no
progress on
my goals
I improved a little
but was far from
meeting my goal
(complete this part a few days before your meeting)
I improved, but
didn’t quite meet
meet all parts of the goal
Explain:
How should this goal change for next year?
Goal #2:
4
I improved and
I met all parts of the goal
This year’s goal is:
This is the exact wording of my goal from my official IEP
Table of Contents:
a list of the things I have chosen to put in my portfolio to
demonstrate my progress
My Final Evaluation of this goal
1
2
3
I made no
progress on
my goals
I improved a little
but was far from
meeting my goal
(complete this part a few days before your meeting)
I improved, but
didn’t quite meet
meet all parts of the goal
4
I improved and
I met all parts of the goal
Explain:
How should this goal change for next year?
Goal #3:
This year’s goal is:
This is the exact wording of my goal from my official IEP
Table of Contents:
a list of the things I have chosen to put in my portfolio to
demonstrate my progress
My Final Evaluation of this goal
1
2
3
I made no
progress on
my goals
I improved a little
but was far from
meeting my goal
(complete this part a few days before your meeting)
I improved, but
didn’t quite meet
meet all parts of the goal
4
I improved and
I met all parts of the goal
Explain:
How should this goal change for next year?
Created for you by Becky Wilson Hawbaker, Malcolm Price Laboratory School, University of Northern Iowa
Goal #4:
This year’s goal is:
This is the exact wording of my goal from my official IEP
Table of Contents:
demonstrate my progress
a list of the things I have chosen to put in my portfolio to
My Final Evaluation of this goal
1
2
3
I made no
progress on
my goals
I improved a little
but was far from
meeting my goal
(complete this part a few days before your meeting)
4
I improved, but
didn’t quite meet
meet all parts of the goal
I improved and
I met all parts of the goal
Explain:
How should this goal change for next year?
Created for you by Becky Wilson Hawbaker, Malcolm Price Laboratory School, University of Northern Iowa
Goal #5:
This year’s goal is:
This is the exact wording of my goal from my official IEP
Table of Contents:
a list of the things I have chosen to put in my portfolio to
demonstrate my progress
My Final Evaluation of this goal
(complete this part a few days before your meeting)
1
I made no
progress on
my goals
2
I improved a little
but was far from
meeting my goal
3
4
I improved, but
didn’t quite meet
meet all parts of the goal
I improved and
I met all parts of the goal
Explain:
How should this goal change for next year?
Created for you by Becky Wilson Hawbaker, Malcolm Price Laboratory School, University of Northern Iowa
Goal #6:
This year’s goal is:
This is the exact wording of my goal from my official IEP
Table of Contents:
a list of the things I have chosen to put in my portfolio to
demonstrate my progress
My Final Evaluation of this goal
1
2
3
I made no
progress on
I improved a little
but was far from
(complete this part a few days before your meeting)
I improved, but
didn’t quite meet
4
I improved and
I met all parts of the goal
my goals
meeting my goal
meet all parts of the goal
Explain:
How should this goal change for next year?
Created for you by Becky Wilson Hawbaker, Malcolm Price Laboratory School, University of Northern Iowa
Goal #7:
This year’s goal is:
This is the exact wording of my goal from my official IEP
Table of Contents:
a list of the things I have chosen to put in my portfolio to
demonstrate my progress
My Final Evaluation of this goal
1
2
3
I made no
progress on
my goals
Explain:
I improved a little
but was far from
meeting my goal
(complete this part a few days before your meeting)
I improved, but
didn’t quite meet
meet all parts of the goal
4
I improved and
I met all parts of the goal
How should this goal change for next year?
Created for you by Becky Wilson Hawbaker, Malcolm Price Laboratory School, University of Northern Iowa
Accommodations and Modifications
Here are my IEP-required accommodations and modifications that were in place this year:
These
accommodations
worked the best for me
(list and explain):
Here are ideas about new accommodations and modifications I’d like to try next
year:
Future Ready Core Course of Study
The following units will be required for graduation under the Future-Ready Core:
UNITS
4 Mathematics Units
SUBJECTS
· Algebra I, Geometry, Algebra II
OR
· Integrated Math I, II, III
· 4th Math Course to be aligned with the student's post high school plans
(At the request of a parent and with counseling provided by the school, a
student will be able to opt out of this math sequence. He/she would be
required to pass Algebra I and Geometry or Integrated Math I and II and two
other application-based math courses.)
4 English Units
3 Social Studies Units
· World History
· US History
· Civics and Economics
3 Science Units
· Biology
· An earth/environmental science
· A physical science
1 Health and Physical Education Unit
6 Elective Units
Two electives must be any combination of Career Technical Education, Arts
Education or Second Language
4 Unit Concentration
As part of this core, the State Board of Education strongly recommends that
local superintendents assist students in developing a four-course
concentration focused on student interests and postsecondary goals. The
concentration would provide an opportunity for the student to participate in
a rigorous, in-depth and linked study. The concentration would not limit a
student's access to opportunities provided through community college
concurrent enrollment, Learn and Earn early college, Huskins or university
dual enrollment. Local superintendents or their designees would approve
student concentrations.
All totaled, students will be required to earn a minimum of 21 units of credit.
The Occupational Course of Study will continue to be available for those students with disabilities who are specifically identified for
this program. There are no changes to the Occupational Course of Study.
In addition to the Future-Ready Core, students will continue to be required to successfully complete a graduation project and to score
proficient on the end-of-course assessments in Algebra I, Biology, English I, Civics and Economics and US History. Local school
districts have the option of adding other requirements for graduation as well.
Occupational Course of Study (OCS)
WHICH STUDENTS SHOULD BE CONSIDERED FOR THE OCS (OCCUPATIONAL
COURSE OF STUDY)?
1. The curriculum was written for students with a 50-69 IQ. The goals and objectives do not go above a fourth
grade level. Students functioning above a fourth grade level or with a 70 plus IQ will need to be carefully
considered by the IEP team. We must make sure that the student is placed in his/her least restrictive
environment.
2. The program was written for the typical EMD self-contained classroom. LD and BED students may be
considered if they are functioning like an EMD student. We will need to have adaptive behavior scores in
the MR range in order to justify considering the student with LD or BED for the OCS program.
3. Placement in the OCS program is an IEP decision. Please consult with the IEP team before making any
commitment for students in the OCS program.
Statement of Understanding
For Enrollment in the Occupational Course of Study (OCS)
I understand that successful completion of the following Occupational Course of
Study requirements must be met:
Successful completion of 28 units of credit, including:
Passing grades in all required OCS coursework:
OCS English I, II, III, IV
OCS Introductory Math, OCS High School Math A, OCS Financial
Management III
Occupational Prep I, II, III, IV
OCS Applied Science and OCS Biology
OCS Social Studies I, II
Also:
Health & Physical Education
Passing grades in four career/technical education courses
Passing grades in additional elective classes
300 hours of successful school-based vocational training hours
240 hours of successful community-based vocational training hours
360 hours of successful competitive paid employment hours
Career portfolio completion of all required components
Any other local requirements
I understand that required Occupational Course of Study coursework credits will not
transfer to another course of study except at electives. However, any successfully
completed course credits from another course of study will transfer to OCS.
I understand that in order for competitive employment hours to be counted toward
meeting the requirements for the OCS, the placement must meet the following guidelines:
1. All employment placements must have prior approval from the OCS teacher or
transition facilitator if hours are going to count toward graduation.
2. All employment placements must be in an integrated setting within the
community.
3. Student must be paid at or above minimum wage for all work performed.
4. The employment placement must meet child labor regulations under the Fair
Labor Standards Act.
5. The employment placement must be open to evaluation of student performance
by the OCS teacher, transition facilitator or employer.
6. It is the student’s responsibility to submit pay stubs to OCS staff to document
paid hours.
(continued)
7. Students may receive supported employment or work adjustment job coaching
if needed.
8. To be counted as “successful” competitive employment, the student must
receive a grade of average or above on job performance evaluations, and
required hours must be completed at no more than three different job sites.
9. Students who are competitively employed during the summer months must
submit pay stubs to OCS staff within the first month of school and employer
evaluations must be successful.
I understand that the vocational training requirements for the Occupational Course of
Study are expected to be completed in a manner that involves moving from school-based
to community-based training, culminating in competitive employment during the last two
years of high school.
I understand that the students and their family members are expected to work
collaboratively and cooperatively with school personnel in obtaining and maintaining a
competitive employment placement. This may involve but not be limited to:
participation in transition planning meetings, follow-up on referrals to outside agencies,
provision of transportation outside of school hours, and completion of all required
paperwork for the school and service providers.
I understand that obtaining a competitive employment placement may require
collaboration with the following agencies:
Social Security Administration if SSI or SSDI payments are being received
Vocational Rehabilitation if supported employment, community-based work
adjustment, or any other service related to competitive employment is needed
Mental Health if case management is needed
Department of Social Services if WorkFirst services are needed
Collaboration with appropriate persons if Workforce Investment Act services are
needed
I understand that in order to obtain competitive employment a valid social security
number or appropriate work permits from U.S. Immigration will be required.
I understand that a work permit from the Department of Social Services will be required
if employment is being obtained for a student under the age of 18.
I understand that successful completion of the Occupational Course of Study will result in
the awarding of the North Carolina high school diploma based on the completion of the
Occupational Course of Study. The OCS is designed to prepare students for employment
and is not considered appropriate for any student who plans to enroll in a curriculum
major at a community college or a four-year university. However, student may still be
eligible for other non-curriculum programs at a community college such as compensatory
education, continuing education, and adult basic education classes.
I understand that successful completion of the requirements for the Occupational Course
of Study may require enrollment in school longer that the traditional four years.
(continued)
This Statement of Understanding was explained on _______________________ by
___________________________ and all parties have indicated their understanding.
Student Signature:
__________________________________________
Parent/Guardian Signature:
__________________________________________
LEA Representative Signature: __________________________________________
Regular Ed. Teacher Signature: __________________________________________
EC Teacher Signature:
__________________________________________
Annual Review of Statement of Understanding:
Date of Review:
Student Signature:
Parent/Guardian Signature:
Regular Ed. Teacher Signature:
EC Teacher Signature:
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Annual Review of Statement of Understanding:
Date of Review:
Student Signature:
Parent/Guardian Signature
Regular Ed. Teacher Signature
EC Teacher Signature:
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Annual Review of Statement of Understanding:
Date of Review:
Student Signature:
Parent/Guardian Signature
Regular Ed. Teacher Signature
EC Teacher Signature
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Annual Review of Statement of Understanding:
Date of Review:
Student Signature:
Parent/Guardian Signature
Regular Ed. Teacher Signature
EC Teacher Signature
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
What are my responsibilities as
a parent of an OCS student?
Attend IEP meetings
Encourage successful student involvement and completion of their course of study
Be sure that your student has the proper attire for working at job sites
Encourage appropriate work behaviors and attitudes
Provide assistance with transportation for your student to work
Parent/adult support is essential for successful completion of the OCS.
Moore County Schools
Mission Statement
Our mission is to provide a safe learning environment where academics and integrity are expected from all. We challenge
all students to reach their full learning potential and inspire them to become productive members of our society .
For more information, contact:
Judy Clendenin, Transition Facilitator
(910) 947-2342
jclendenin@mcs.k12.nc.us
OCS
Occupational
Course of
Study
Moore County Schools
Exceptional Children’s Department
160 Pinckney Road
Carthage, NC 28327
(910) 947-2342
What is the
Occupational
Course of
Study?
The Occupational Course of Study (OCS) is one of four pathways to earn a high school diploma in the North Carolina public school system. The
other three are
Career Prep,
College Tech Prep, and College/University Prep.
The OCS curriculum prepares students to be competent, dependable employees and independent, responsible adults. It focuses on the
development of functional academic skills and hands-on job training with the goal of transitioning the student from high school into competitive
employment.
Who determines eligibility for the OCS?
Eligibility for the Occupational Course of Study is determined by the Individualized Education Plan (IEP) team including the student and the parent(s). The OCS
should be considered only after the other courses of
aids and services.
study are determined to be inappropriate even with the use of modifications, supplemental
Which students should consider the OCS?
Students who enroll in the Occupational Course of Study should be those who:
are being served in the Exceptional Education program
have a post-school outcome goal for competitive paid employment upon graduation from high school
wish to pursue a course of study that provides functional academics and hands-on job training.
currently are not having their needs met by the NC Standard Course of Study
What are the course requirements for the OCS?
Occupational English I-IV (4 credits)
Occupational Math I-III (3 credits)
Occupational Preparation (6 credits)
Occupational Science I, II (2 credits)
Occupational Social Studies I II (2 credits)
Health/PE (1 credit)
Career/Technical Education (4 credits)
Six electives (local requirement)
28 total credits required
Are there any additional exit requirements for the OCS?
Students must complete:
a career portfolio
all IEP goals and objectives
300 hours of school-based work training
240 hours of community-based job training
360 hours of paid employment
¿Cuáles son mis responsabilidades como el padre de un estudiante OCS?
Asistir a las reuniones IEP
Alentar el envolvimiento exitoso del estudiante y completar su curso de estudio
Asegurar que el estudiante tenga la vestimenta apropiada para los lugares de trabajo
Alentar comportamiento y actitudes de trabajo apropiados
Proveer asistencia con la transportación para que el estudiante pueda trabajar
El Apoyo de los Padres/Adultos es esencial para completar
con éxito el OCS.
Moore County Schools
Declaración de la Misión
Nuestra misión es proveer un ambiente de aprendizaje seguro a donde la integridad y educación sean esperadas por todos.
Retamos a todos los estudiantes a lograr su máximo potencial de aprendizaje e inspirarlos a convertirse en miembros
productivos de nuestra sociedad.
Para más información, comuníquese con:
Judy Clendenin, Transition Facilitator
(910) 947-2342
jclendenin@mcs.k12.nc.us
OCS
Curso de Estudio
Ocupacional
Moore County Schools
Exceptional Children’s Department
160 Pinckney Road
Carthage, NC 28327
(910) 947-2342
¿Qué es el Curso de Estudio Ocupacional?
El Curso de Estudio Ocupacional (OCS) es una de cuatro formas de obtener el diploma de escuela superior en el sistema escolar público de
North Carolina.
Los otros tres son:
Carrera Preparatoria
Colegio Técnico Preparatoria, y
Preparatoria Colegio/Universidad
El plan de estudio OCS prepara estudiantes para ser competentes, empleados dignos de confianza, y adultos responsables. Se enfoca en el
desarrollo de las destrezas académicas funcionales y entrenamiento con las manos con la meta de transición del estudiante desde Escuela
Superior a un empleo competente
¿Quién determina elegibilidad para el OCS?
Elegibilidad para el Curso de Estudio Ocupacional es determinada por el equipo del Plan Educacional Individual (IEP) incluyendo el padre(s) y el
estudiante. El OCS debe ser considerado solamente después de que se determine que otros cursos de estudio son inapropiados aún con el uso de
modificaciones, ayuda suplementaria y
servicios.
¿Cuáles estudiantes deben considerarse OCS?
Estudiantes matriculados en el Curso de Estudio Ocupacional deben ser aquellos que:
Se le está dando servicios en el Programa de Educación Excepcional
Tienen una meta para un empleo pagado competitivo después de graduarse de Escuela Superior
Desea perseguir un curso de estudio que provea estudios y entrenamiento
¿Cuáles son los requisitos de curso para el OCS?
Inglés Ocupacional I-IV (4 créditos)
Matemática Ocupacional I-III (3 créditos)
Preparación Ocupacional (6 créditos)
Ciencia Ocupacional I, II (2 créditos)
Estudios Sociales Ocupacional I II (2 créditos)
Health/PE (1 créditos)
Educación Técnica/Carrera (4 créditos)
Seis electivas (requisitos locales)
28 total de créditos requeridos
¿Hay requisitos de salida adicionales para el OCS?
Estudiantes tienen que completar:
Un portafolio de carrera
Todos los objetivos y metas del IEP
300 horas de entrenamiento de trabajo en la escuela
240 horas de entrenamiento basado en la comunidad
360 horas de empleo pagado
Moore County Schools
P.O. Box 1180 Carthage, North Carolina 28327
Occupational Course of Study
Career Portfolio Presentation Evaluation
Our mission is to provide a safe learning environment where academics and integrity are expected from all. We challenge all students
to reach their full learning potential and inspire them to become productive members of our society.
Student Name: ______________________________________________________
Evaluation Team
_______________________________________
________________________________________
_______________________________________
________________________________________
_______________________________________
________________________________________
_________________
Date
Portfolio
Forms completed appropriately:
Presentation
Personal Appearance:
□ Cover Sheet
□Appropriately Dressed for Interview
□ Personal Information
□ Appropriately Groomed for Interview
□ Educational Information
Introduction:
□ Employment Information
□ Name
□ Reference Information
□ Area of occupational interest
□ Resume
□ Description of portfolio contents
□ High School Transcript
□ Knows contents of portfolio
□High School Record – Summary of CTE
Training Summary:
□High School Record Extracurricular
□ Explanation of school-based work
Participation and Community Activity
□ Record of School Based Job Hours and
Record of School-Based Job Experience
With Evaluation
□ Explanation of community-based work
□ Explanation of competitive work
Response to Questions:
□ Appropriately answered questions
□Record of Community-Based Job Hours
□ Answered in appropriate length of time
and Record of Job Sites with Evaluation
□ Maintained composure during questions
□Record of Competitive Employment
Communication Skills:
□ Record of Competitive Evaluation
□ Maintained eye contact
□ Confidential Divider
□Spoke in complete sentences
□ Personal Documents
□ Clear, easy to understand
□Used proper grammar
□ Used appropriate voice tone
□ Expressed points clearly and logically
□ PORTFOLIO COMPLETE
□ PRESENTATION COMPLETE
VOCATIONAL REHABILITATION
GOAL
North Carolina Vocational Rehabilitation provides counseling, training, education, medical, transportation, and
other support services to persons with physical or mental disabilities in order to help them become independent
or job-ready and place them into employment.
TARGET POPULATION
N.C Vocational Rehabilitation is based on the presence of a physical or mental impairment, which for the
individual constitutes or results in a substantial impediment to employment.
The individual must require vocational rehabilitation services to prepare for, enter, engage in, or retain gainful
employment. It is presumed that an individual can benefit from VR services in terms of an employment
outcome. Individuals receiving SSI or SSDI are presumed eligible.
There is no specific upper or lower age limit and some services may begin prior to the current employable age
of 16 years of age.
FUNDING
Vocational Rehabilitation in North Carolina is both federal and state funded.
STAFFING
VR Counselor—1 per Moore County Schools, may vary by county size; some counties may share. Case
Worker Asst. position Vocational Evaluator—tests to find strengths and weaknesses, and office assistant.
All over Moore County there are five VR counselors, two office assistants, one case work assistant, one job
placement specialist, one case work technician, and one community rehabilitation specialist. VR counselors
must have their Masters degree. They work in hospitals, schools, mental health, ex-prisoners, etc.
EVALUATION
Evaluations used by NC Vocational Rehabilitation are vocational evaluation, driving evaluation, psychological
assessment, work sampling, and medical evaluation.
Behavior Management
(back to top)
Table of Contents
Functional Behavioral Assessment Information
Behavior Intervention Plan Information
FBA/BIP Form
Manifestation Information
Physical Restraints
Functional Behavior Assessment
Functional Behavioral Assessments (FBA) have been used to try and determine why individuals exhibit specific
behaviors and how the environment interacts with the individual and those behaviors.
Moore County views this to be a critical piece for any of its students who are exhibiting problematic behaviors,
especially if several of the following apply:
Referred to SST for behavior.
Referred to SST for academics, but also has behavior issues.
Repeated suspensions for like behavior.
Required by law after an identified student has been suspended for more than 10 days.
Note: A child in which an IEP team identifies to be SED should have an FBA/BIP in place through SST prior to
initial placement.
The FBA components are as follows:
Identify student strengths
Define the target behavior
Collect data
Understand the context of the behavior
Determine the function of the behavior
Write a hypothesis statement
Once data is collected an IEP team must meet to develop the hypothesis statement.
Behavioral Intervention Plan
A behavioral intervention plan (BIP) is designed to try to help a child learn to change behavior. Once the
function of the student’s behavior has been determined an IEP team should develop a BIP.
The purpose of a BIP is to:
Identify proactive strategies to prevent not suppress undesired behaviors
Develop interventions that are logically related to the functional categories
Teach replacement behaviors rather than suppress behaviors through punishment
The BIP is a part of the IEP and therefore should be developed in an IEP team meeting. It should also be
reviewed by the team periodically.
Functional Behavioral Assessment
And
Behavioral Intervention Plan
Students Name:________________________
School:_____________________________
Date:___________________________
Grade:____________________________
ID Number:______________________
Functional Assessment:
I). What are the student’s strengths (academic and behavioral)?:
1. _______________________________________________________________________________________
2. _______________________________________________________________________________________
3. _______________________________________________________________________________________
4. _______________________________________________________________________________________
II).
A.
Problem Behavior
Concrete Definition
of Behavior
Frequency
Intensity
Duration
Problem Behavior: Identify the problem behaviors that most interfere with the student’s functioning.
Concrete Definition: Define behavior in concrete terms that are easy to communicate and simple to record/measure.
Frequency: Examples: every 10 minutes, 4 of 5 days, 4 x per hour, 1 x per day, etc…
Intensity: On a scale of 1 to 10 (1 being low intensity and 10 high intensity).
Ex: 3 = touched kid gently, 10 = gave kid a black eye
Duration: How long does the entire episode last? Example: Fred gets upset, leaves class, & runs through the halls yelling
and screaming. The episode begins when Fred get upset and ends when he is able to get control of himself. Duration =
approximately 35 minutes.
B. Circle or highlight the problem behavior, from the concrete definition list, that the committee would like
to work on changing. Most likely, this will be the behavior that is highest in frequency, intensity and duration.
C. From the list below, indicate the triggers (antecedents), concurrent events, medical/home factors,
consequences used, and functions of the behavior (does the student want to escape, gain attention, or control)
that seems to be supporting the problem behavior by placing a check mark in the appropriate space.
Problem Behavior:
.
(Write the problem behavior in the space above.)
What triggers the behavior?
__ Lack of social attention
__ Demand/ Request
__ Does not understand task
__ Transition between tasks
__Transition between settings
__ Interruption in routine
__ Negative social interaction with peers
__ Consequences imposed for neg. behavior
__ Inability to process directions
__ Other (specify):__________________________
During what concurrent event(s) does the behavior occur?
__Independent seat work
__ Large group instruction
__ Small group instruction
__ Crowded setting
__Unstructured activity
__ Structured activity
__Specific time of day ________
__With a specific teacher(s)___________________
__A specific subject _________________________
__Other (specify):___________________________
Are there any Medical/Home factors that are contributing to this behavior?
__Medication (change/not taking)
__ Change in home/family dynamics
__ Medical conditions
__Other (specify):___________________________
What consequences have been implemented for problem behavior?
__ Behavior ignored
__Reprimand/Warning
__Stated expectation
__Time-out
__Loss of privileges
__Sent to office
__Communications with home
__Discipline referral
__ In-School suspension
__Out-of-School suspension
__Other (specify):___________________________
Does the student try to escape she he/she misbehaves? If so, why?
__ Avoid a demand or request
__Avoid and activity/task (if known)
__Avoid a person
__Escape the classroom/setting
__Escape the school
__Other (specify):___________________________
Does the student try to gain control when he/she misbehaves? If so, why?
__Get desired item/activity
__Gain adult attention
__Gain peer attention
__Get sent to preferred adult
__Gain power
__ Gain revenge
__Other (specify):_______________________
III). Develop a hypothesis (best guess) about the function or purpose of the student’s problem behavior. This
hypothesis predicts the general conditions under which the behavior is most and least likely to occur
(antecedents), as well as the probable consequences that serve to maintain it.
Hypothesis Statement:
IV). Behavioral Intervention Plan:
Develop a Behavioral Intervention Plan (BIP) using information from functional assessment.
A).
Replacement Behaviors
B).
C).
Activities/Modifications
D).
Reinforcements
Consequences
1.
2.
3.
E).
How will BIP be monitored
How often
By Whom
How many days will BIP be in effect before evaluated:___________________________________________
Date of next meeting:______________________________________________________________________
Signatures of IEP Team members who attended this meeting on: _______________________
LEA Rep. _____________________________________
Special Ed. Teacher______________________________
Reg. Ed. Teacher________________________________
Parent/Gaurdian_________________________________
Student: _______________________________________
V). Evaluation of Behavioral Intervention Plan
A. Describe student’s progress toward goal:
B. Were the steps in the BIP implemented as indicated (be specific):
C. Describe any modifications, deletions, or revisions that the committee feels would enhance the effectiveness of the
plan based on new information gained from initial BIP:
D). Revised BIP
Replacement Behavior
Activities/Modifications
Reinforcements
Consequences
1.
2.
How many days will BIP be in effect before evaluated:_____________________________________________________
Date of next meeting for revised BIP:___________________________________________________________________
Signatures of IEP Team members who attended the meeting on: ______________________________________________
LEA Rep.____________________________________________________________
Special Ed. Teacher____________________________________________________
Reg. Ed. Teacher______________________________________________________
Parent/Guardian_______________________________________________________
Student:______________________________________________________________
Other:________________________________________________________________
**At the next meeting, the IEP Team may choose to continue to use the BIP (including any revisions), revise the BIP again or start the
process over (new functional assessment and BIP) based on new information.
Manifestation Determination
Things to remember
A student with a disability may be removed for up to 10 days for violating the Student Code of Conduct,
just as you would for a non-disabled student.
During this “FAPE free zone” services are not required
School personnel may also impose additional removals of the child of not more than 10 school days in a
row in that same school year for separate incidents of misconduct, as long as those removals do not
constitute a change of placement.
Disciplinary Change in Placement
Occurs when a child is removed for more than 10 consecutive days (long-term suspension)
May be when a child has a series of removals that have a pattern and constitute a change in placement
Key Points of Manifestation
Conducted in order to determine if the student can be removed (suspended) for their disciplinary
infraction.
Must be completed within 10 school days of any decision that constitutes a change in placement.
The manifestation team must review all relevant information in the student’s file, including the child’s
IEP, any teacher observations, and any relevant information provided by the parents to determine if
o the conduct in question was caused by, or had a direct and substantial relationship to the child’s
disability
o the conduct in question was the direct result of the LEA’s failure to implement the IEP
NOTE: Please refer to the forms section of this handbook for more information and guidance in
completing the form.
Physical Restraints
Although the Law does allow for physical restraint of a student under certain circumstances, this should be
rare and must be documented using the following form. Below is the definition of physical restraint and
what the law states about its use.
Definition:
"Physical restraint" means the use of physical force to restrict the free movement of all or a portion of a
student's body.
Physical Restraint:
(1)
Physical restraint of students by school personnel shall be considered a reasonable
use of force when used in the following circumstances:
a.
As reasonably needed to obtain possession of a weapon or other dangerous
objects on a person or within the control of a person.
b.
As reasonably needed to maintain order or prevent or break up a fight.
c.
As reasonably needed for self-defense.
d.
As reasonably needed to ensure the safety of any student, school employee,
volunteer, or other person present, to teach a skill, to calm or comfort a student,
or to prevent self-injurious behavior.
e.
As reasonably needed to escort a student safely from one area to another.
f.
If used as provided for in a student's IEP or Section 504 plan or behavior
intervention plan.
g.
As reasonably needed to prevent imminent destruction to school or another
person's property.
(2)
Except as set forth in subdivision (1) of this subsection, physical restraint of students
shall not be considered a reasonable use of force, and its use is prohibited.
(3)
Physical restraint shall not be considered a reasonable use of force when used solely
as a disciplinary consequence.
(4)
Nothing in this subsection shall be construed to prevent the use of force by law
enforcement officers in the lawful exercise of their law enforcement duties.
Documentation of Physical Restraint / Therapeutic Hold
Student:_________________________
Teacher:_______________________
Date of Incident:________ Time Restraint Began:_________ Time Restraint Ended:________
Type of Restraint Used:________________________________________________________
Staff Involved with the Restraint:__________________________________________________
1. Give a brief description/account of the circumstances and actions that led up to the incident
(Specify behavior which warranted the Physical Restraint.)
2. Briefly describe the student’s behavior during the restraint.
3. Briefly describe the de-escalation process and the student’s behavior after the Restraint.
4. Were other parties called in and why?
TESTING
(back to top)
Table of Contents
Accommodations
NCExtend1
Additional Information
-District-wide Tests
-Exemptions
- Cluster Students
Accommodations
Accommodations are changes to the administration of an assessment that does not change the construct
intended to be measured by the assessment or the meaning of the resulting scores.
Accommodations are meant to allow student with disabilities to demonstrate their true abilities; however,
students must not receive unnecessary or inappropriate accommodations.
Accommodations designated for the test should be routinely used with class instruction and similar classroom
assessments.
Refer to the Testing Students with Disabilities manual for specific details on each accommodation.
The testing matrix (DEC 4, page 6) must be filled out in detail when describing certain accommodations
such as read aloud, multiple test session, extended time, etc.
NC Extend 1
Description
The NCEXTEND1 Alternate Assessment is a performance-based alternate assessment designed to assess
students with significant cognitive disabilities. NCEXTEND1 Alternate Assessment items are grade-level
performance items that measure the standards specified in the North Carolina Standard Course of Study (SCS)
Extended Content Standards. These Extended Content Standards are available for download at the following
address: http://www.ncpublicschools.org/ec/.
Who is Eligible?
Students who:
• Have a current IEP;
• Are enrolled in grades 3–8 or 10 according to the Student Information Management System (e.g., SIMS/NC
WISE);
• Are instructed in the North Carolina Standard Course of Study Extended Content Standards in ALL assessed
content areas; and
• Have a SIGNIFICANT COGNITIVE DISABILITY (i.e., exhibit severe and pervasive delays in ALL areas of
conceptual, linguistic and academic development and also in adaptive behavior areas, such as communication,
daily living skills, and self-care).
For whom is Extend1 NOT appropriate?
Students who:
• are being instructed in ANY OR ALL of the general grade level content standards of the North Carolina
Standard Course of Study;
• demonstrate delays only in academic achievement;
• demonstrate delays due primarily to behavioral issues;
• demonstrate delays only in selected areas of academic achievement; or
• if in high school, are pursuing a North Carolina high school diploma (including students enrolled in the
Occupational Course of Study).
The NCEXTEND1 Alternate Assessment is designed for students who have a severe intellectual disability;
it is NOT designed for students who have a specific learning disability.
Additional information may be found at:
http://www.ncpublicschools.org/accountability/policies/tswd/ncextend1
Additional Testing Information
District-wide assessments
According to IDEA, all students with disabilities must be included not only in all statewide assessments but also
in all district-wide assessments. Participation may be through the general test administration with
accommodations or by an alternate assessment. All students with disabilities must participate, including those
with the most significant cognitive disabilities.
Exemptions
An exemption is very rare and is normally only for medical reasons. The EC office must be contacted if you
think a child is in need of an exemption.
Cluster EC Students/Cross Enrollment
A student that has been placed at a school by an IEP team that is not their home school must be cross enrolled
so that their test scores will be returned to what is their home school. The school must electronically identify
(using the cluster file) the appropriate schools for these student’s test results prior to the opening of the end-ofgrade testing window. (Please make sure you talk with your school’s Test Coordinator and your NCWISE
Data Manager. They should be aware of this!)
Review of Accommodations (Form found in Form Section)
Column 1 of this form is to be filled out prior to testing. The rest of the form is completed during or after
testing and a copy should then be kept with the EC folder.