Disease Spread Model
advertisement

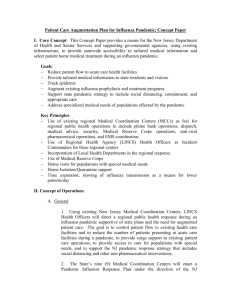
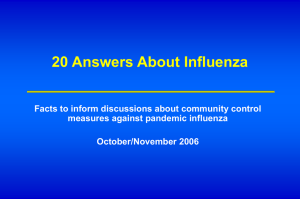
TECHNICAL APPENDIX Modeling Seasonality and Viral Mutation in an Influenza Pandemic Agent-based Model As introduced in the main text, we developed a spatially and temporally explicit agent-based model to simulate the disease spread and tested it with data from the state of Georgia. Agent-based models, also known as individual-based models, can simulate an entire population (and the dynamics within) at the scale of a single individual. Such models have been used to investigate strategies at the regional/national levels for containing an emerging pandemic influenza strain at its source (1).The agent-based model consists of two parts: (i) the natural disease progression within an infected individual (i.e. “agent”), and (ii) the contact network of each individual (agent) in the population. Natural disease progression We used a detailed SEIR (Susceptible-Exposed-Infected-Recovered) model for part (i) when mutation is not considered (1). Each infected individual progresses from S (susceptible) through E (exposed but not yet infectious) to status IP (presymptomatic). The individual has probability pA of not developing symptoms and becoming IA (infectious and asymptomatic), or enters status IS (infectious and symptomatic) with probability (1–pA). With probability pH a symptomatic individual is hospitalized (H) and with probability pD a hospitalized individual dies (D). R is the state of recovered 1 and a recovered individual is immune. This natural disease progression for influenza is depicted in Figure 1 of (1). When mutation is taken into account, we assumed recovered individuals are not fully immune to the mutant virus so that they may become susceptible again with probability p(t), which is a function of time t. The susceptible individual, if infected, goes over the same process as we described in the above SEIR model (see Figure 1). We assume that each individual can be infected at most two times (once by the original strain and once by the new strain). p(t) IA pA S E R IP 1-pH 1-pA H IS pH Figure 1. 1-pD D pD Natural disease history for influenza at day t (the probability p(t) changes over time) As pointed out by (2, 3), the “reinfection probability” p(t) increases with the time t. We use the “reinfection rate” δ instead of setting a constant reinfection probability p. Every day each of the “candidates” (recovered individuals who have not re-entered susceptible yet) become susceptible with probability δ. The day T, when such a 2 candidate re-enters the susceptible pool, is a geometric random variable with probability distribution: Prob (T = t)= (1 – δ)(t– t*-1)·δ Correspondingly, the reinfection probability at time t (t>t*) is p(t) = 1– (1 – δ)(t– t*) which increases as t increases since 0<δ<1. The estimates of pA, pH, and pD and the duration of each stage in the SEIR model are as outlined in (1) (details can be provided upon request). The estimates of δ (we tested 0.5%, 1.5%, 5%, 8%, 10%, 20% in the simulation) follow from (2, 4). Contact network We used a group model to construct the contact network in part (ii) (see Figure 2). There are 3 levels of mixing for each individual: household, peergroup (classroom for children and workplace for working adults) and community. Hence, a susceptible individual can get infected through contacts with his/her family members, classmates/colleagues, or randomly meets someone when going to public places such as grocery stores, theaters, etc. 3 Figure 2. An example of the contact network The model is age-structured as we divided the population into 5 age groups: 0-5, 6-11, 12-18, 19-64, 65+. The first 3 groups represent children who are assumed to have higher susceptibility and infectivity compared to adults. The average classroom sizes are 14, 20, and 30 for these 3 children’s groups, respectively (5). Individuals in the 4th group are working adults. The workplace size for working adults is a Poisson random variable with mean 20 (maximum 1000). The last age group is constituted by elderly and they do not mix in peer groups. To calibrate the model of the contact network, we estimated the values of 5 parameters: R0 (reproductive number), θ (the proportion of transmission by people who are either presymptomatic or asymptomatic), ω (the proportion of infections generated by those who are not symptomatic), γ (the proportion of transmission that 4 occurs outside the households) and δ (the proportion of transmission outside the home that occurs in the community). The estimates of these 5 parameters are from Wu et al. (see Table 1 of (1)). Based on these estimates, we used a similar nonlinear technique (1) to calculate the other parameters. We adjusted the calculation for our age-based model using the age-based parameters (calculation details can be provided upon requests). In summary, our basic disease spread model is similar to several other simulation models used for influenza pandemic in the literature (1, 6, 7, 8); however, different from some of the others we consider seasonality and mutation. References 1. Wu JT, Riley S, Fraser C, et al. Reducing the impact of the next influenza pandemic using household-based public health interventions. PLoS Medicine 2006;3:1532-40. 2. Casagrandi R, Bolzoni L, Levin SA, et al. The SIRC model and influenza A. Mathematical Biosciences 2006;200:152-69. 3. Pease C. An evolutionary epidemiological mechanism, with applications to type A influenza. Theoretical Population Biology 1987;31:422-30. 4. Finkenstadt BF, Morton A, Rand DA. Modelling antigenic drift in weekly flu incidence. Statistics In Medicine 2005;24:3447-61. 5 5. Commission GA. 2008. (http://www.coe.uga.edu/gac). (Accessed May 5, 2008). 6. Ferguson NM, Cummings DA, Fraser C, et al. Strategies for mitigating an influenza pandemic. Nature 2006;442:448-52. 7. Germann TC, Kadau K, Longini IM, et al. Mitigation strategies for pandemic influenza in the United States. Proceedings of the National Academy of Sciences of the United States of America 2006;103:5935-40. 8. Longini IM, Halloran ME. Strategy for Distribution of Influenza Vaccine to High-Risk Groups and Children. American Journal of Epidemiology 2005;161:303-6. 6